Download to read offline

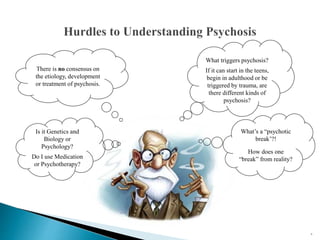
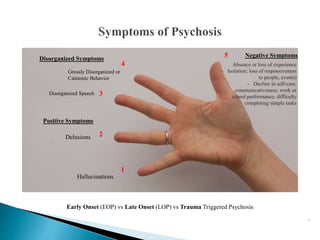
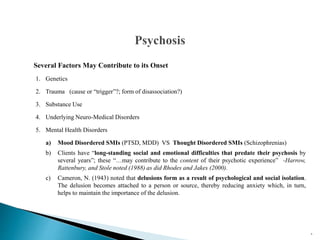
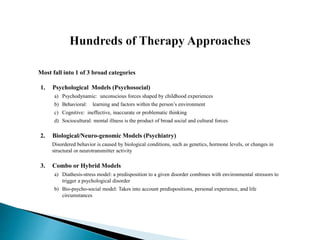
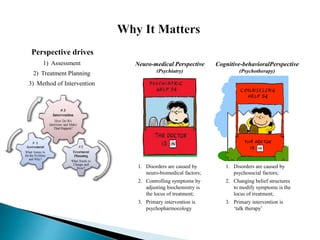
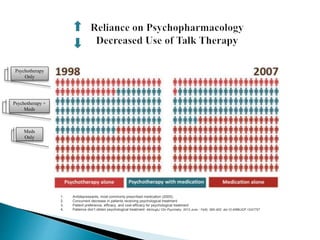
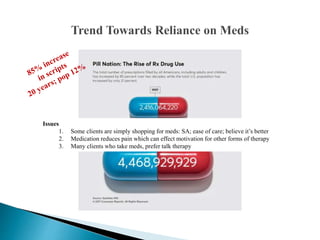
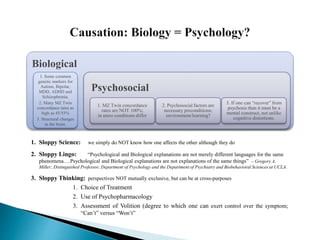

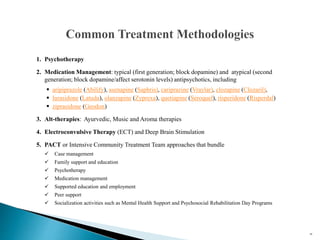
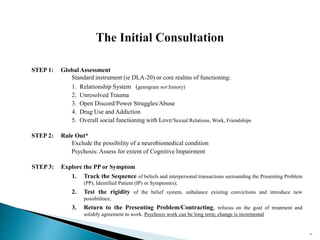






The document discusses the philosophy and practice of clinical outpatient therapy. It begins with a disclaimer stating the purpose is to improve therapy practice through a deeper understanding of methods. It then provides biographical information about the author, including their experience and training in substance abuse counseling, community mental health, and family therapy models from the 1970s-1990s. The document goes on to discuss perspectives on the causes of psychosis, including biological, psychological, and hybrid models. It also addresses the debate around treating psychosis primarily through medication versus psychotherapy.

















































































