This document discusses anti-glaucoma medications. It begins by outlining the goal of glaucoma treatment which is to preserve vision by lowering intraocular pressure. Several classes of medications are described including prostaglandin analogues, beta-blockers, alpha agonists, carbonic anhydrase inhibitors, parasympathomimetics, and others. Specific drugs within each class are explained along with their mechanisms of action, dosing, efficacy, and side effects. Target intraocular pressure ranges are discussed based on factors like baseline pressure and damage level.









![Target IOP calculation
The Collaborative Initial Glaucoma Treatment Study equation:
Target IOP = 1 – ( [Reference IOP + VF score]/100 x reference IOP)
Alternative formula
Target IOP = Initial IOP([100 – Initial IOP]/100) – D
D - a constant based on the level of glaucomatous damage
D = –6 for no evidence of damage, 0 for mild damage, 3
for moderate damage, and 6 for severe damage
11
12/16/2023
Dr Moti](https://image.slidesharecdn.com/anti-glaucomamedications-231216192055-c9ff1a56/75/ANTI-GLAUCOMA-MEDICATIONS-pptx-Moti-pptx-11-2048.jpg)
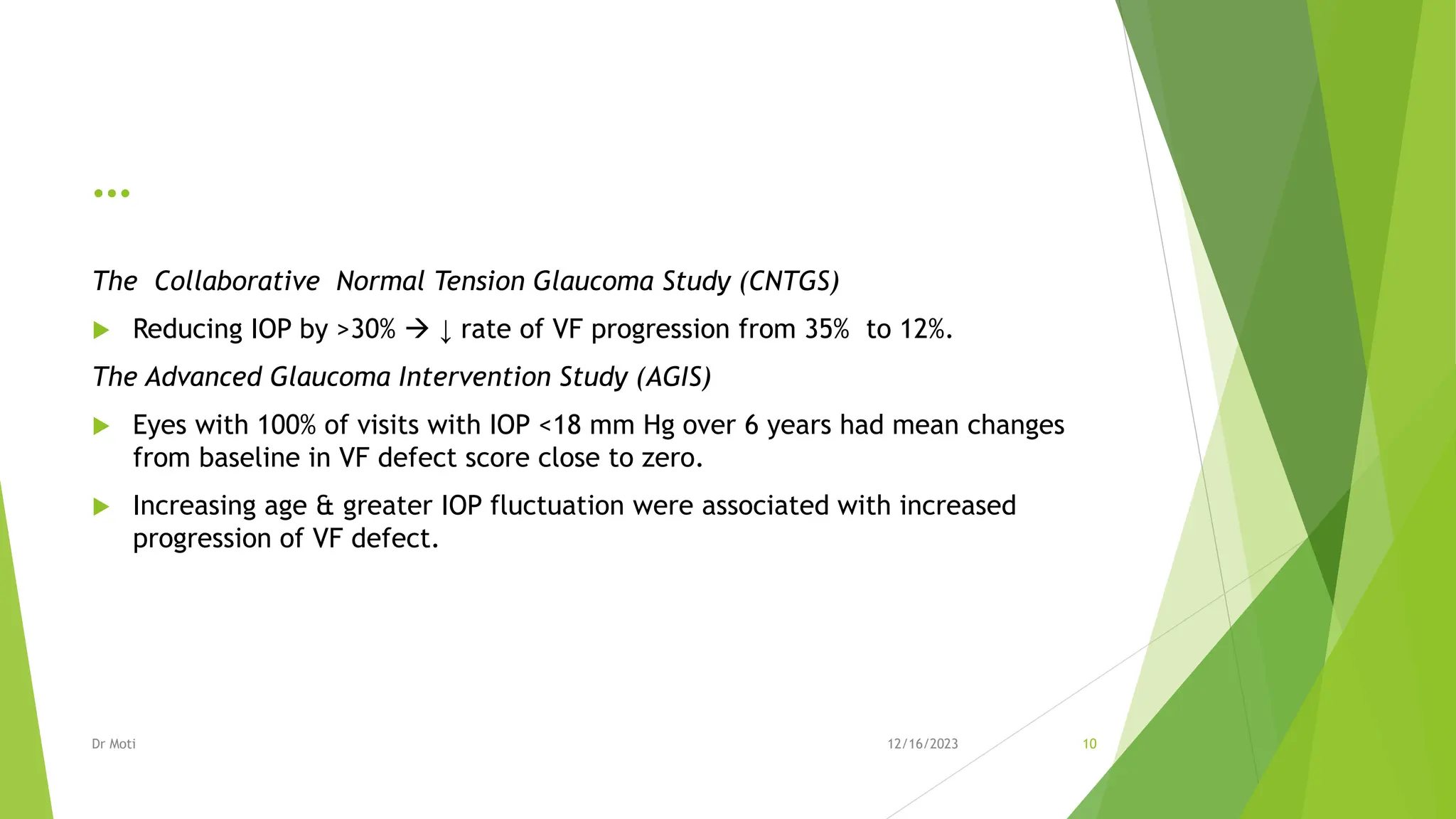
![…
Initial IOP
(mmHg)
Level of damage & target IOP
None Mild Moderate Severe
15 18 12-13 9-10 6-7
20 22 16 13 10
25 24-25 18-19 15-16 12-13
30 27 21 18 15
40 30 24 21 18
12
TABLE . Target IOP (mmHg) Based on target IOP = initial IOP[(100 - initial IOP)/100] -D, where D = -6 for no
damage, 0 for mild damage, +3 for moderate damage, and +6 for severe damage, from Duane’s Clinical
Ophthalmology 2013 edition page 5613
12/16/2023
Dr Moti](https://image.slidesharecdn.com/anti-glaucomamedications-231216192055-c9ff1a56/75/ANTI-GLAUCOMA-MEDICATIONS-pptx-Moti-pptx-12-2048.jpg)