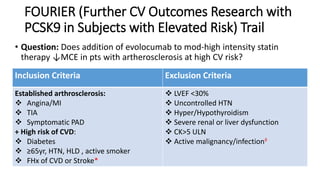
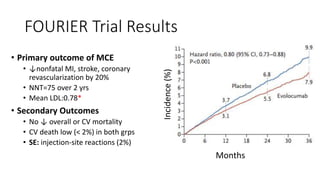
This document summarizes the cardiovascular benefits of evolocumab, a PCSK9 inhibitor, based on the FOURIER trial. The FOURIER trial found that adding evolocumab to moderate or high-intensity statin therapy reduced major cardiovascular events like heart attack, stroke, and coronary revascularization by 20% over 2 years compared to placebo in high-risk patients. Evolocumab lowered LDL cholesterol by 60% on average and had an acceptable safety profile with only injection site reactions occurring in more than 2% of patients. While evolocumab did not reduce overall or cardiovascular mortality, it provides an effective additional option to further lower LDL and reduce cardiovascular risk when added to statin therapy.

























































![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)


















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



