




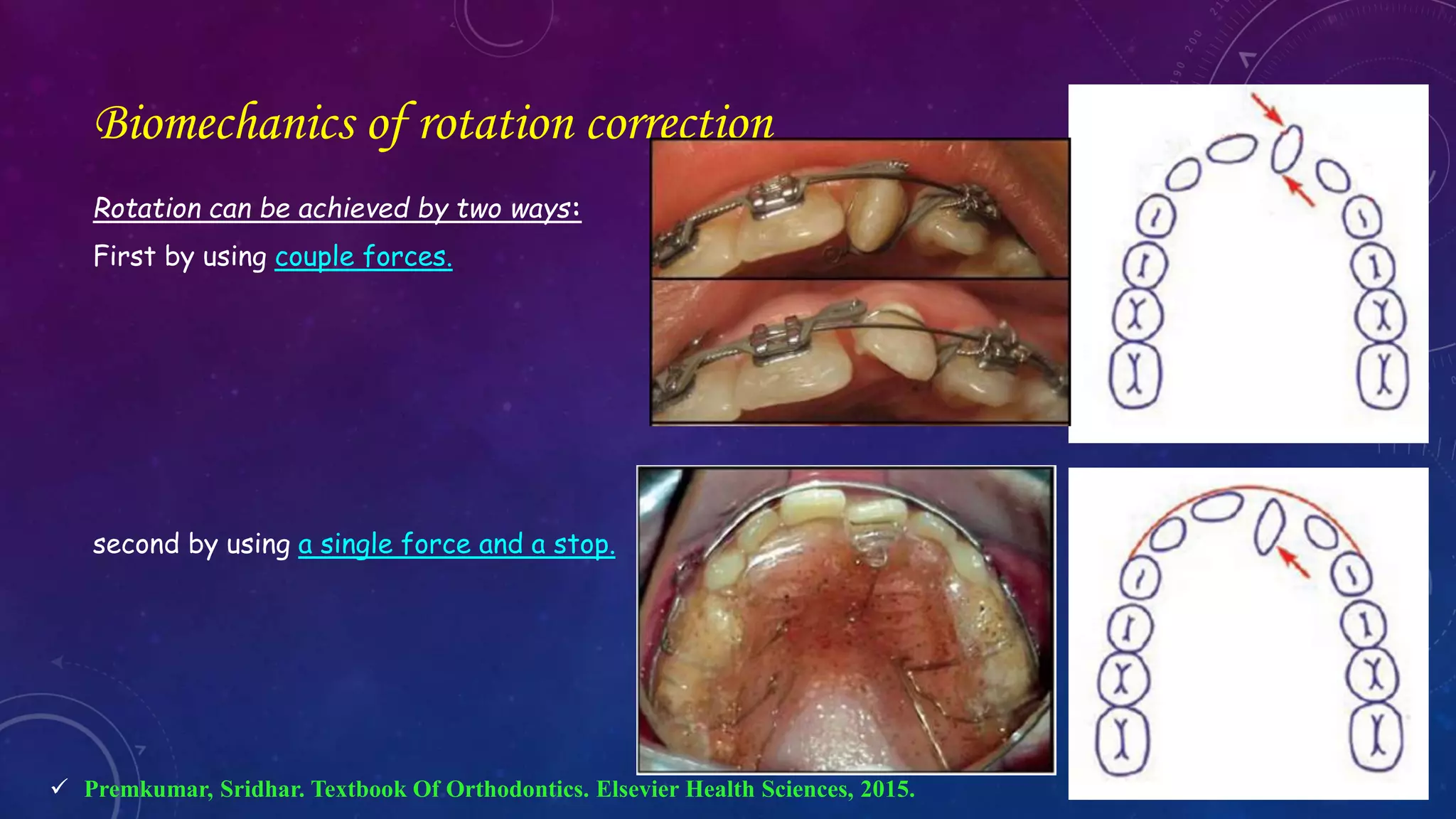
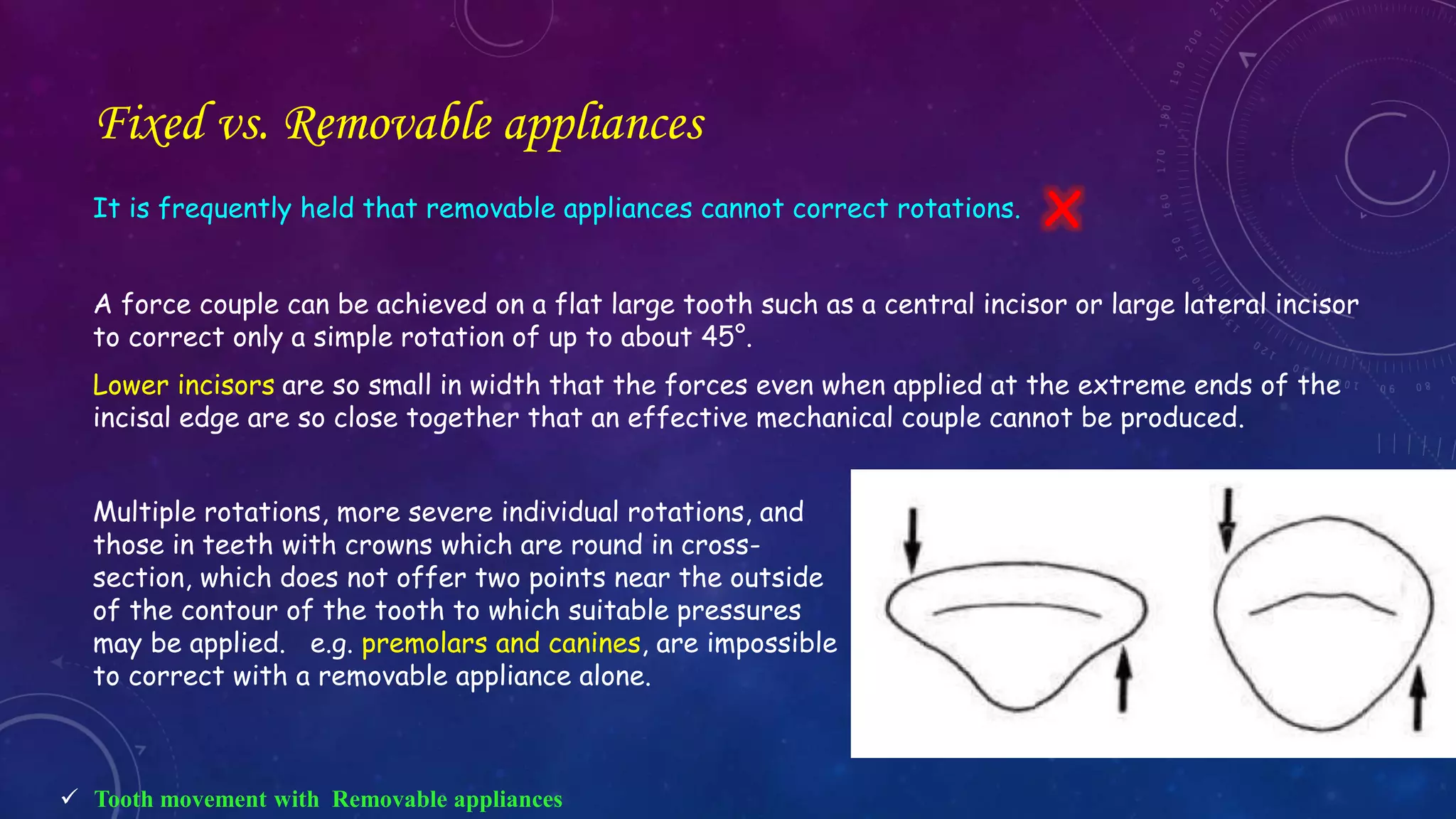
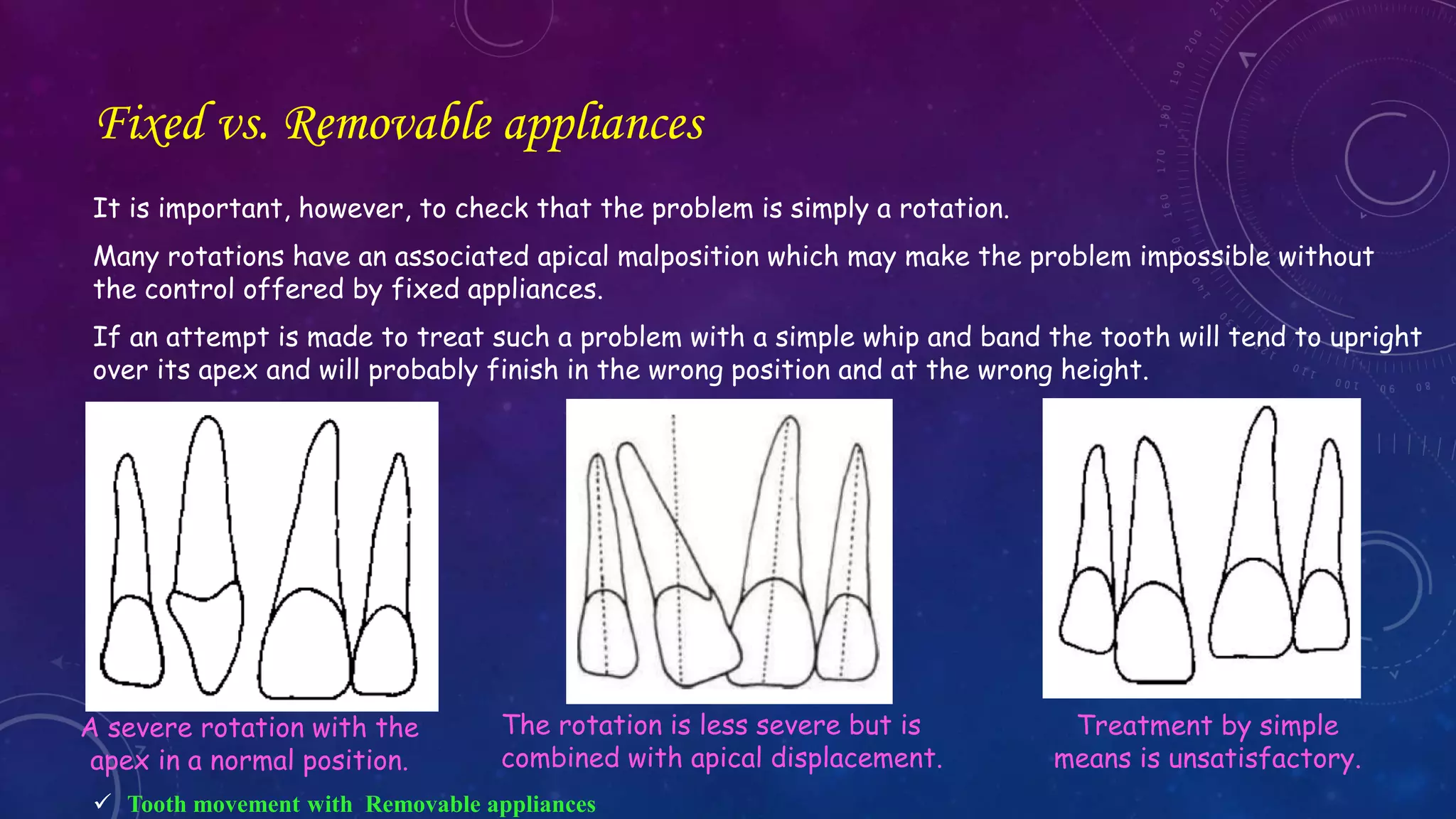
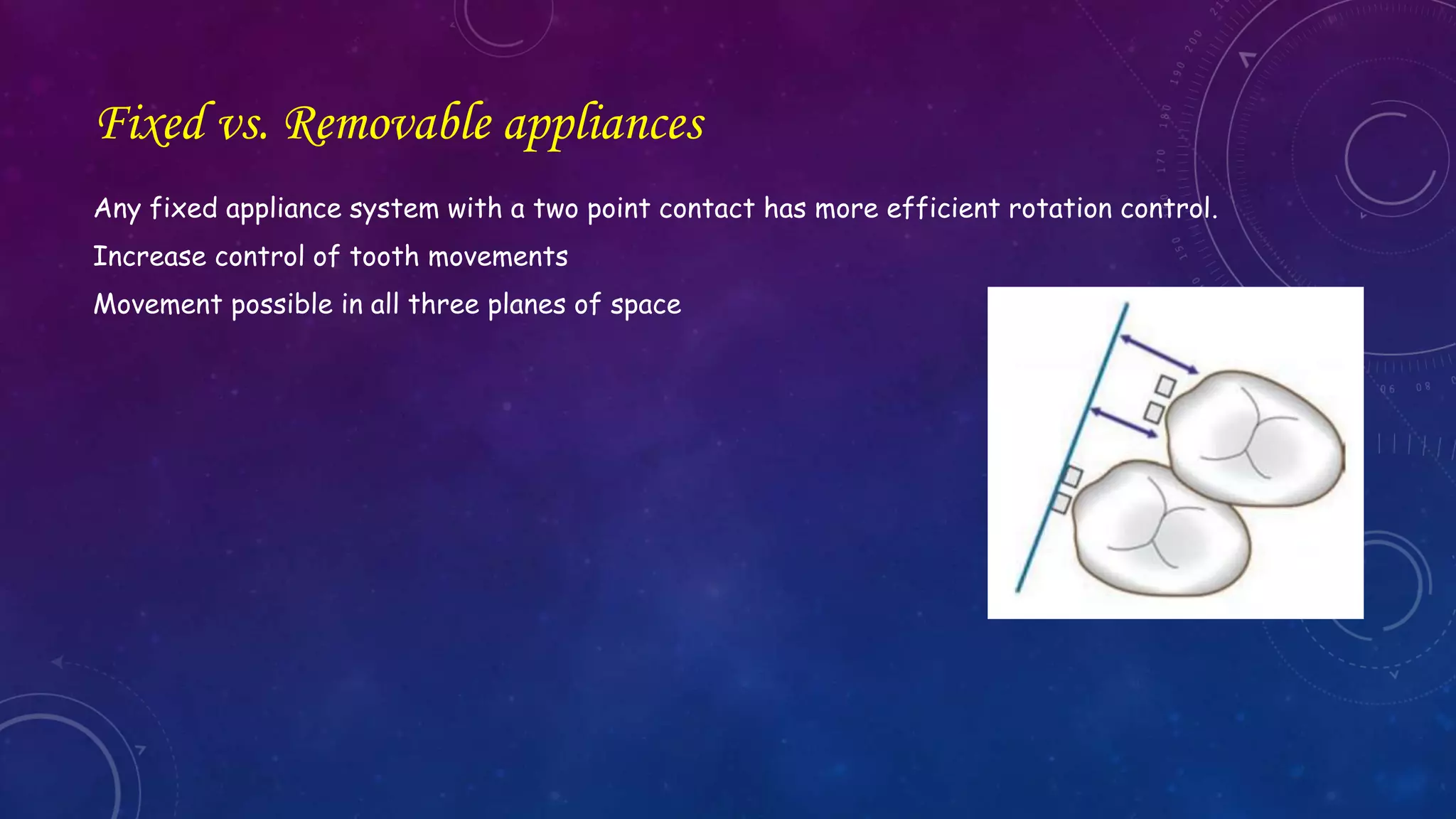

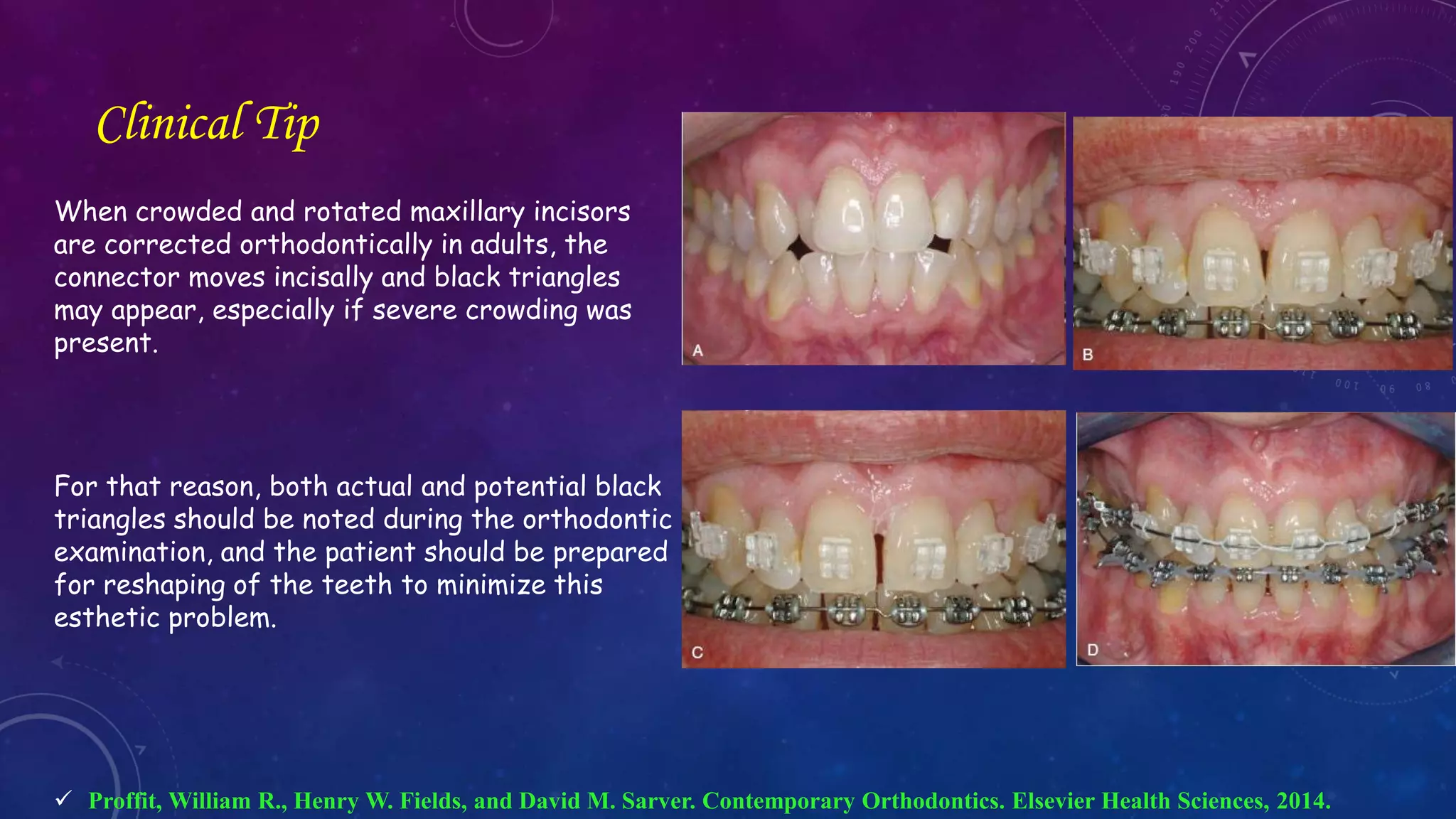




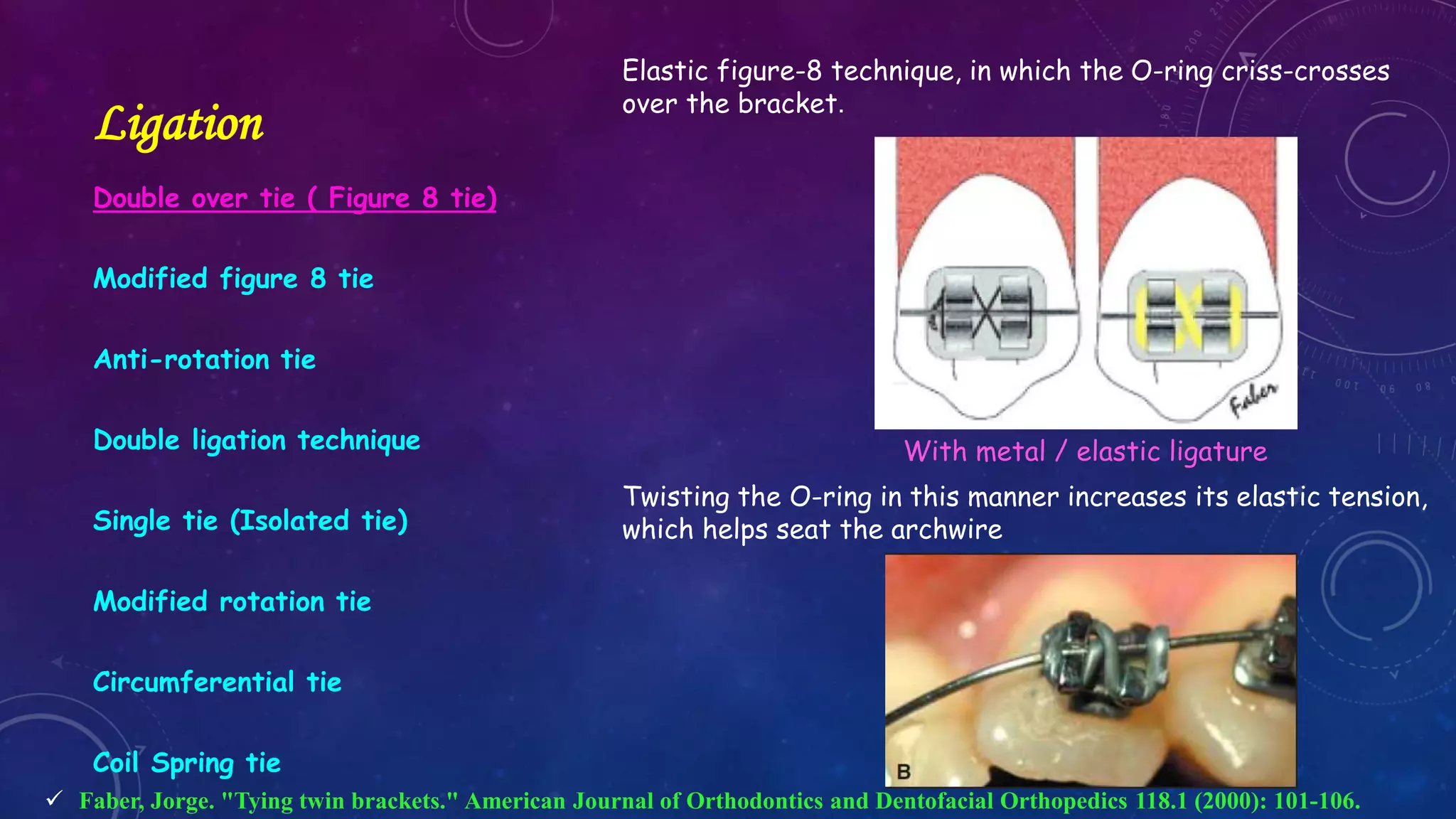


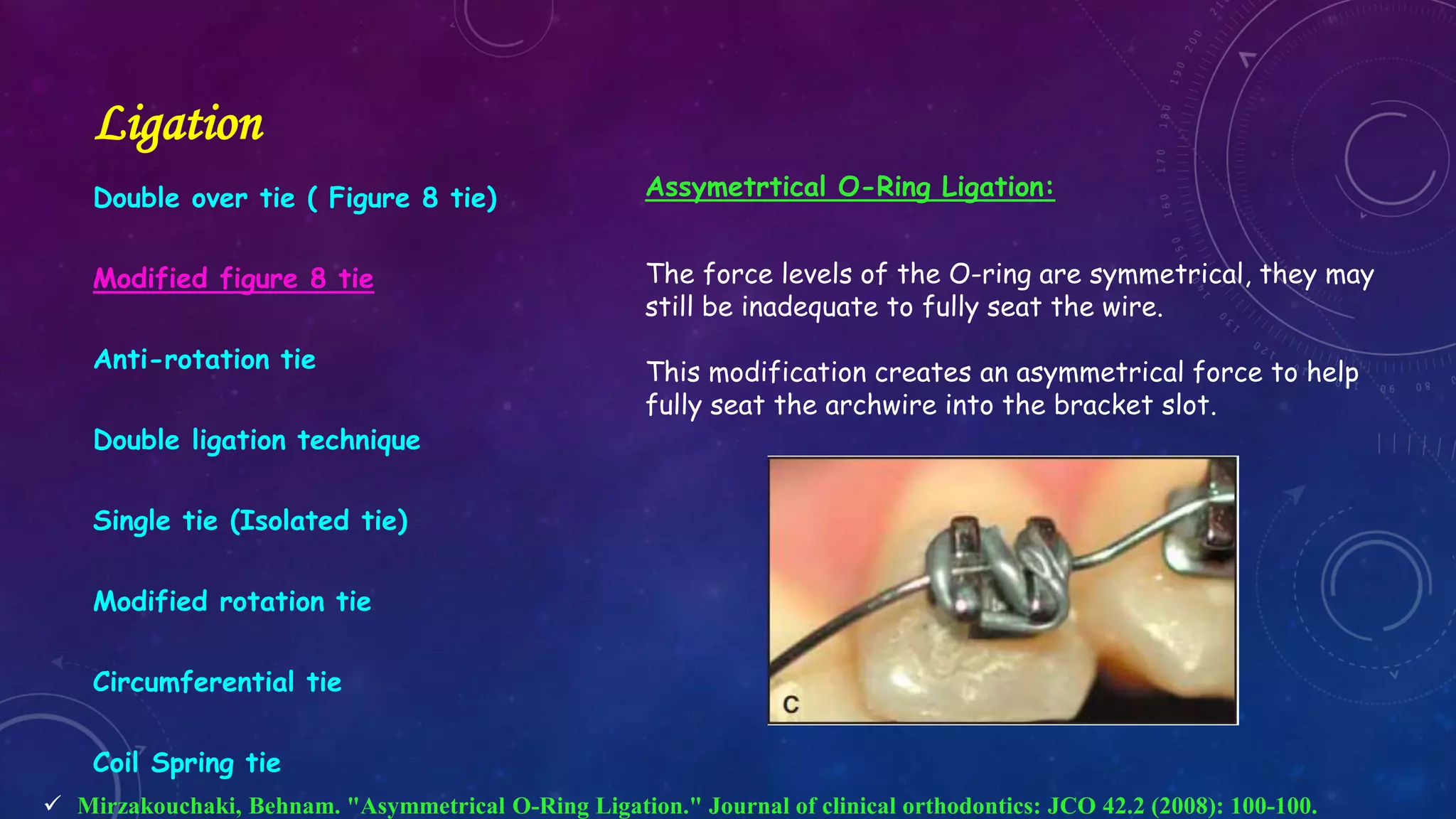
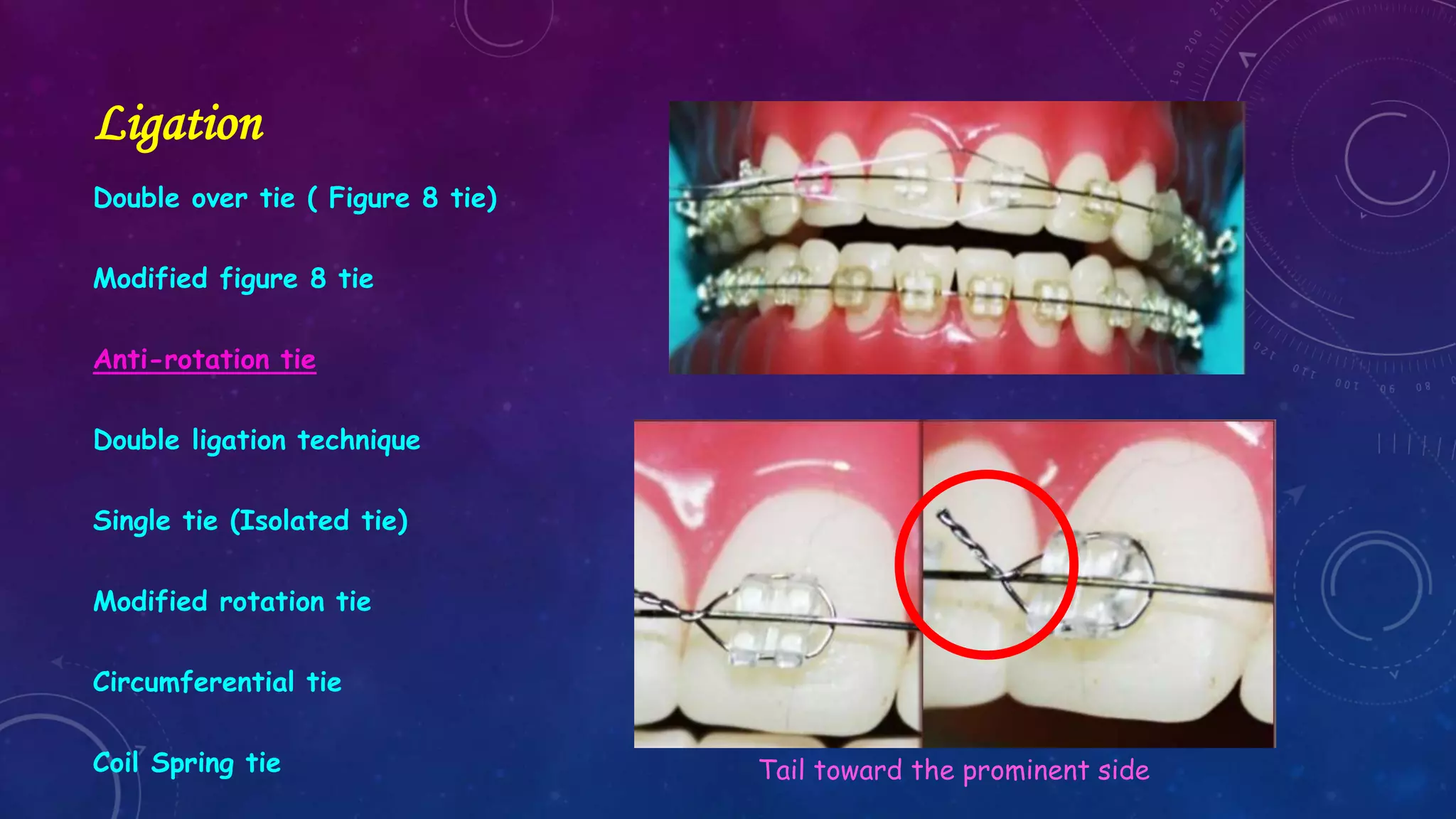
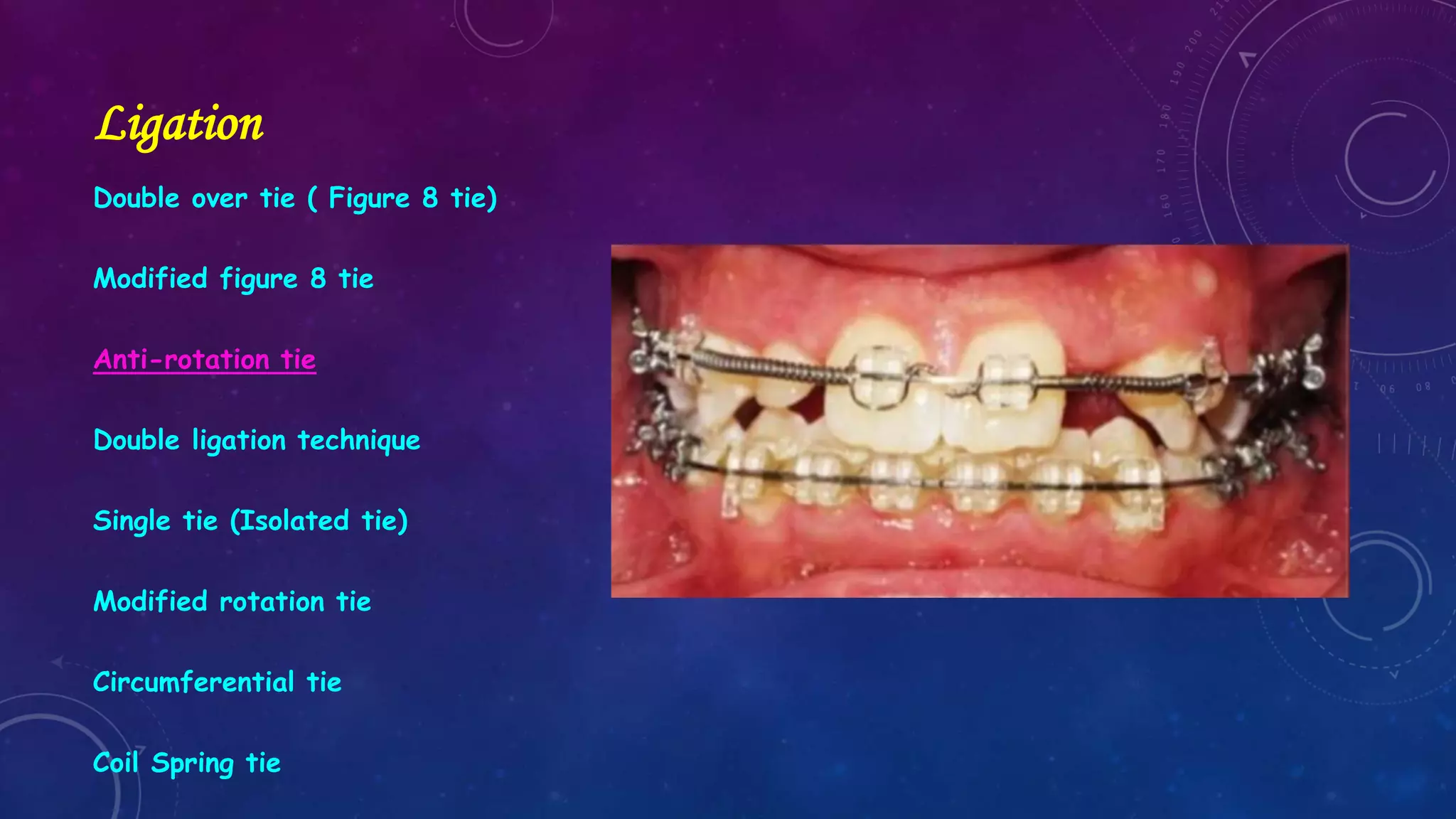



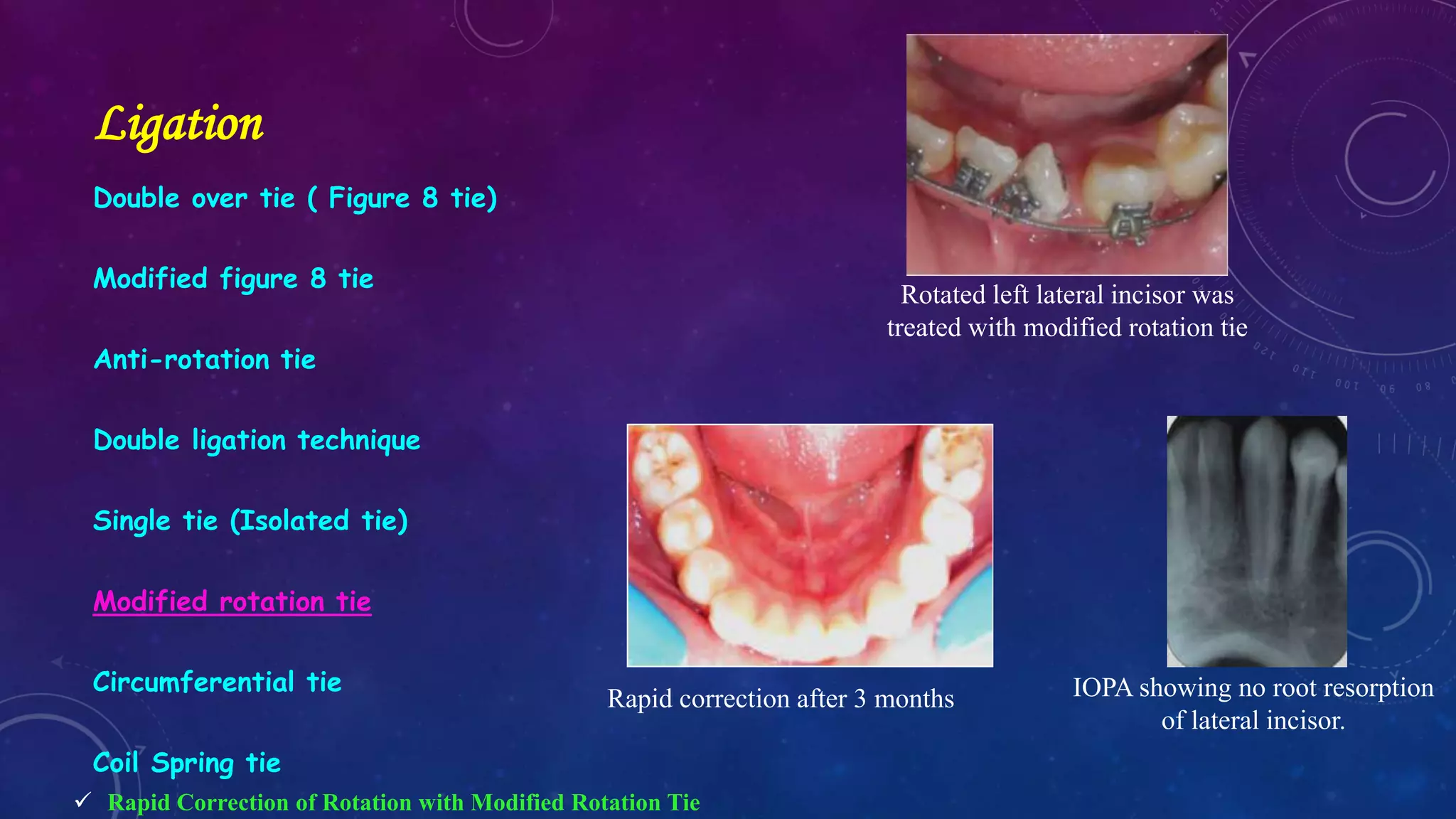
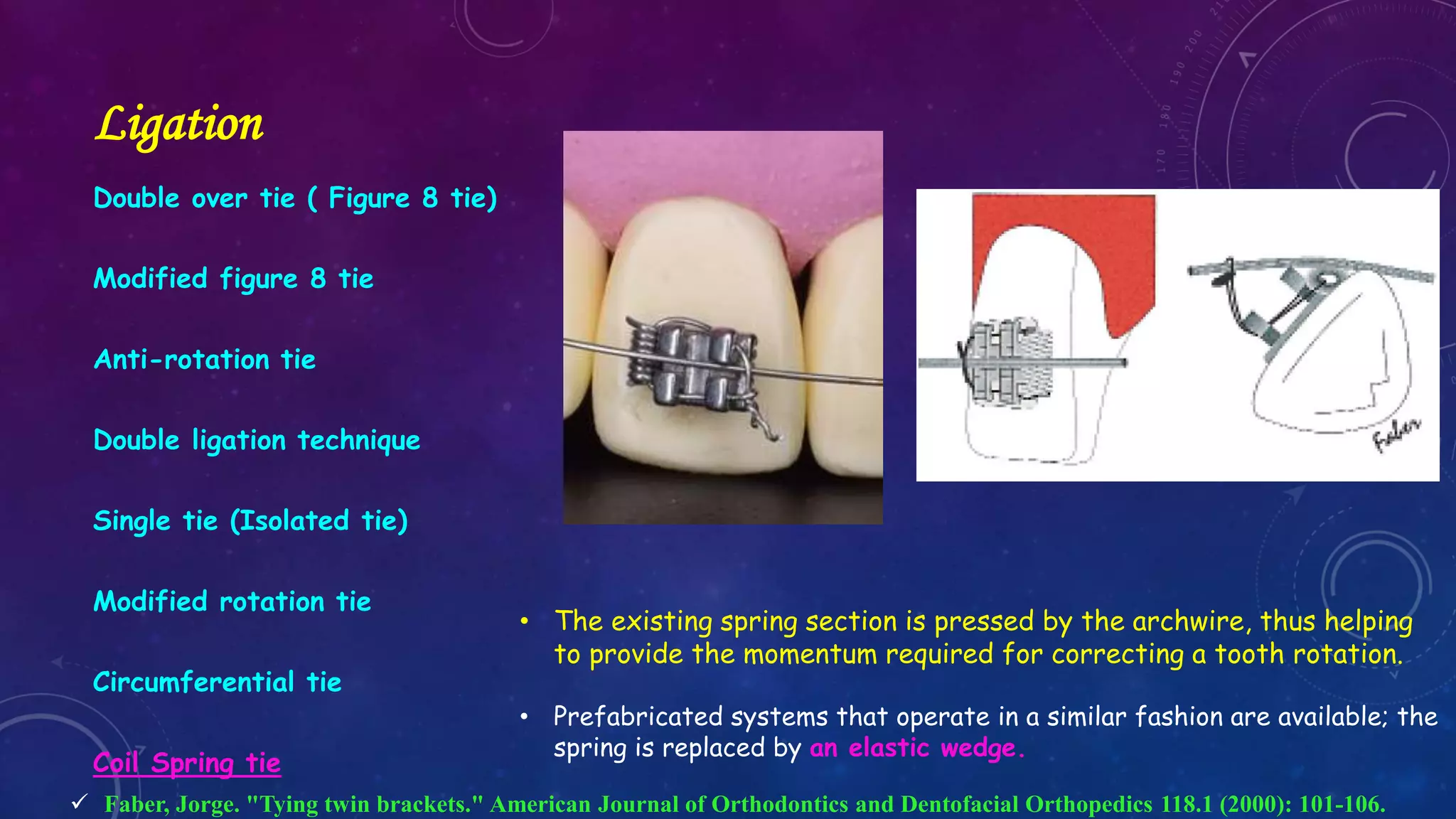
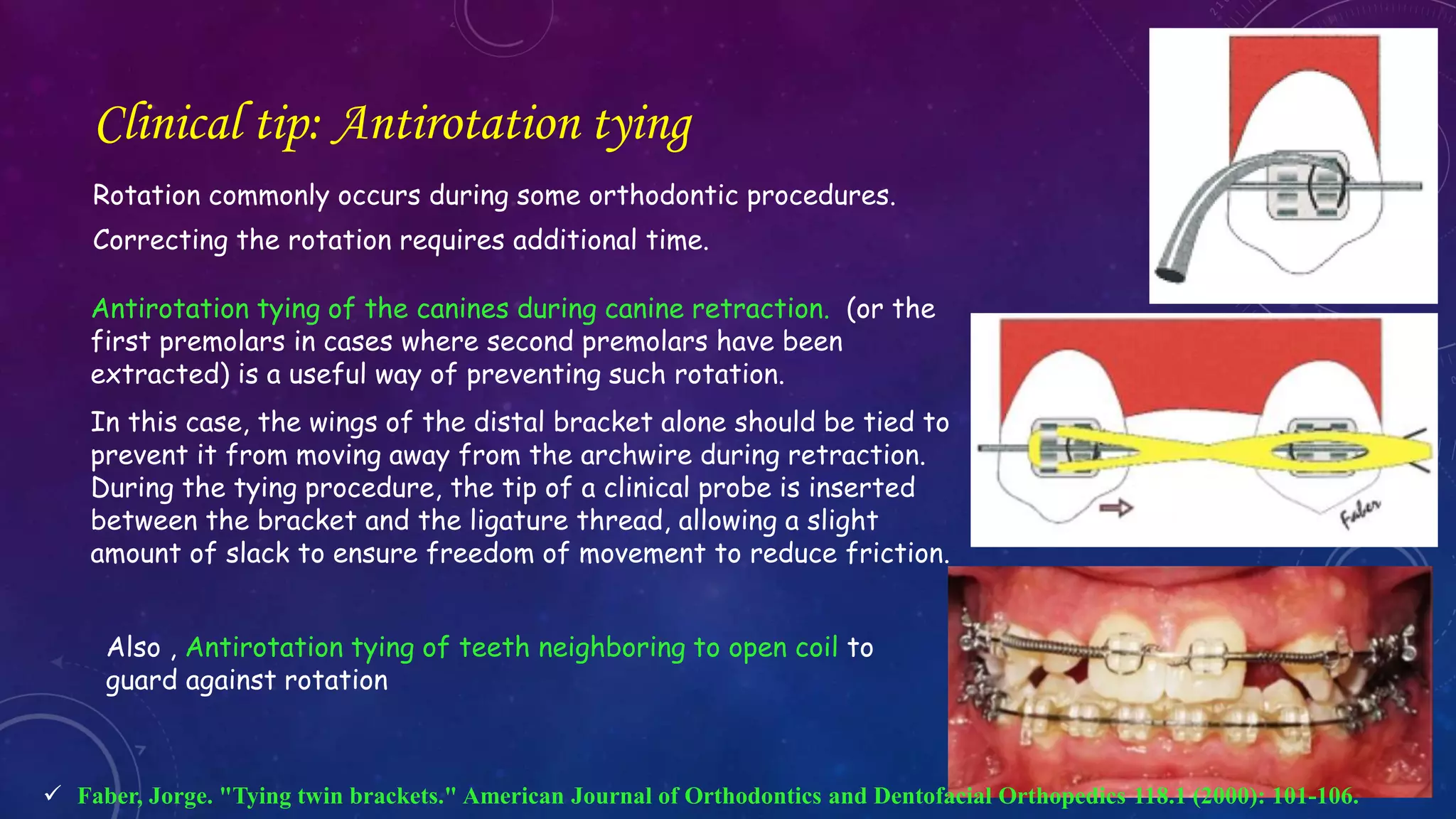



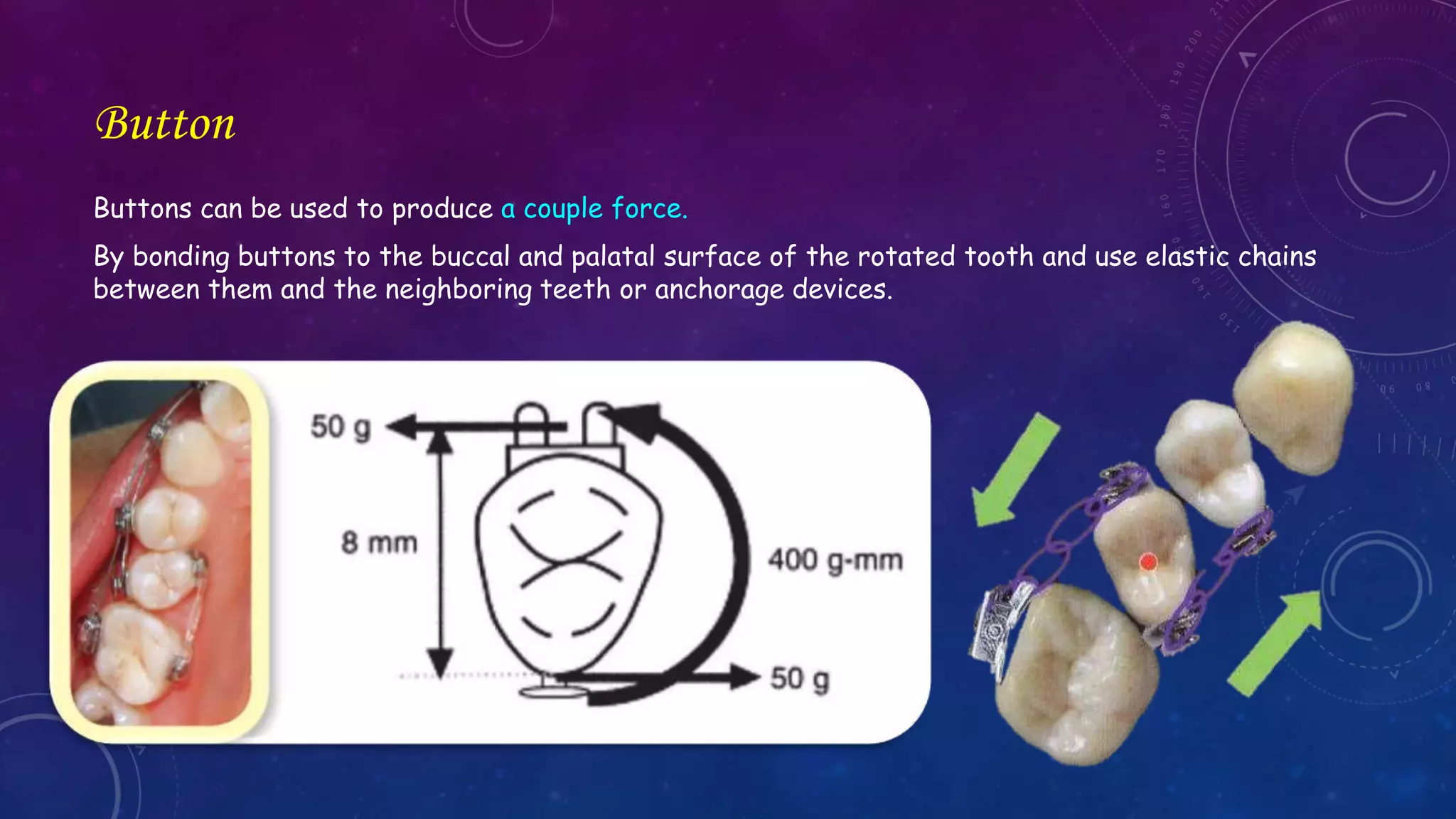
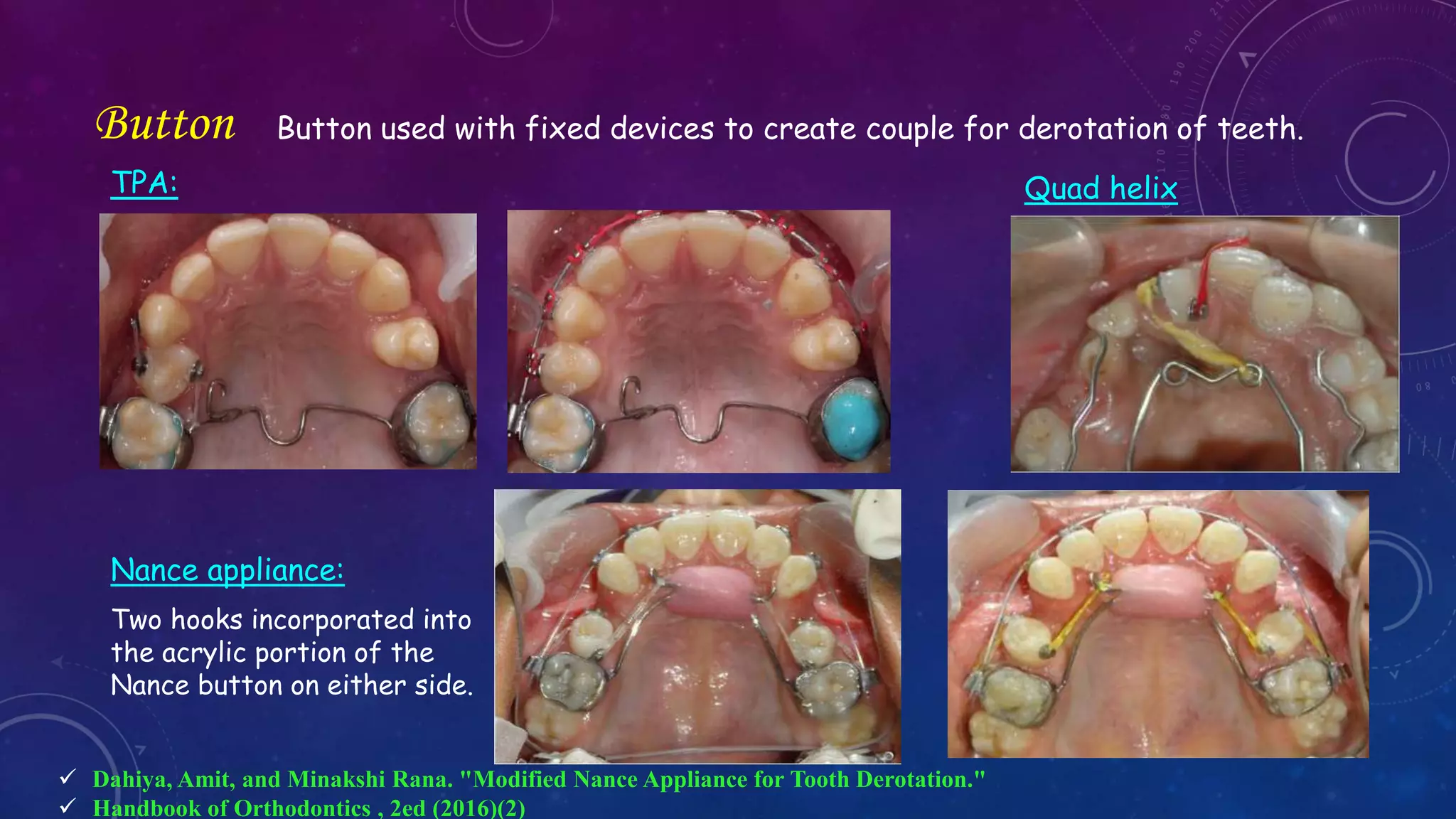


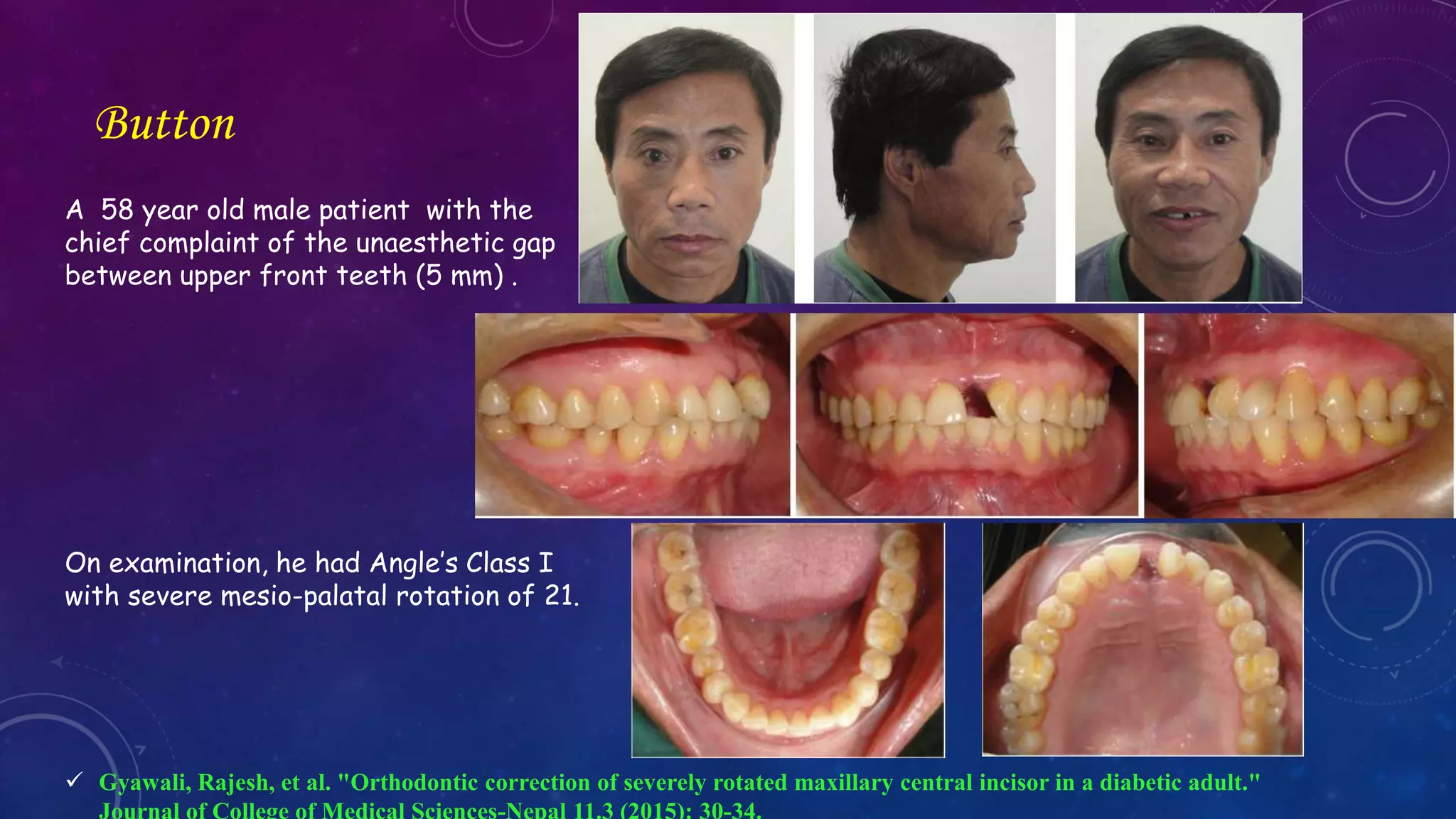

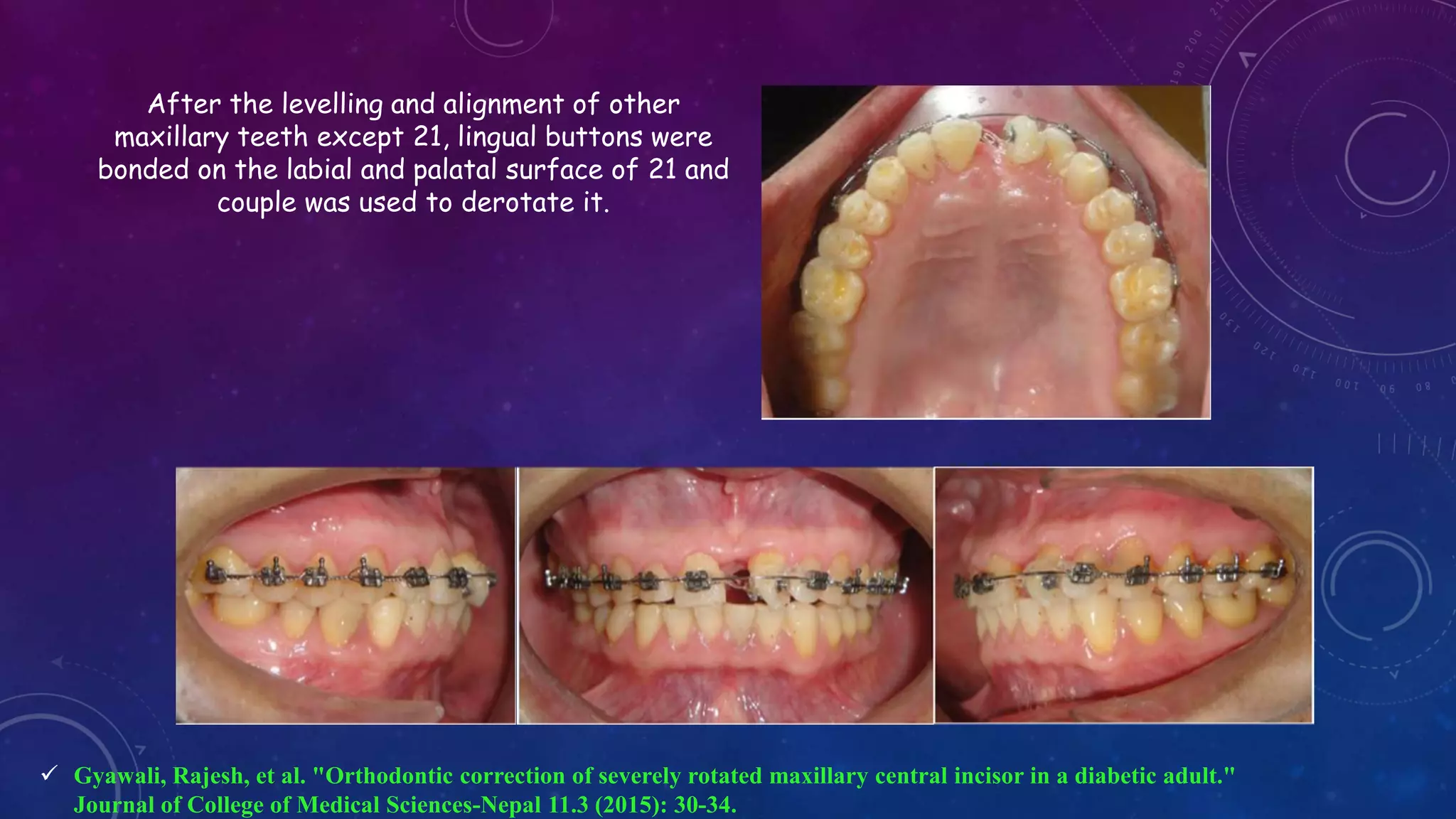



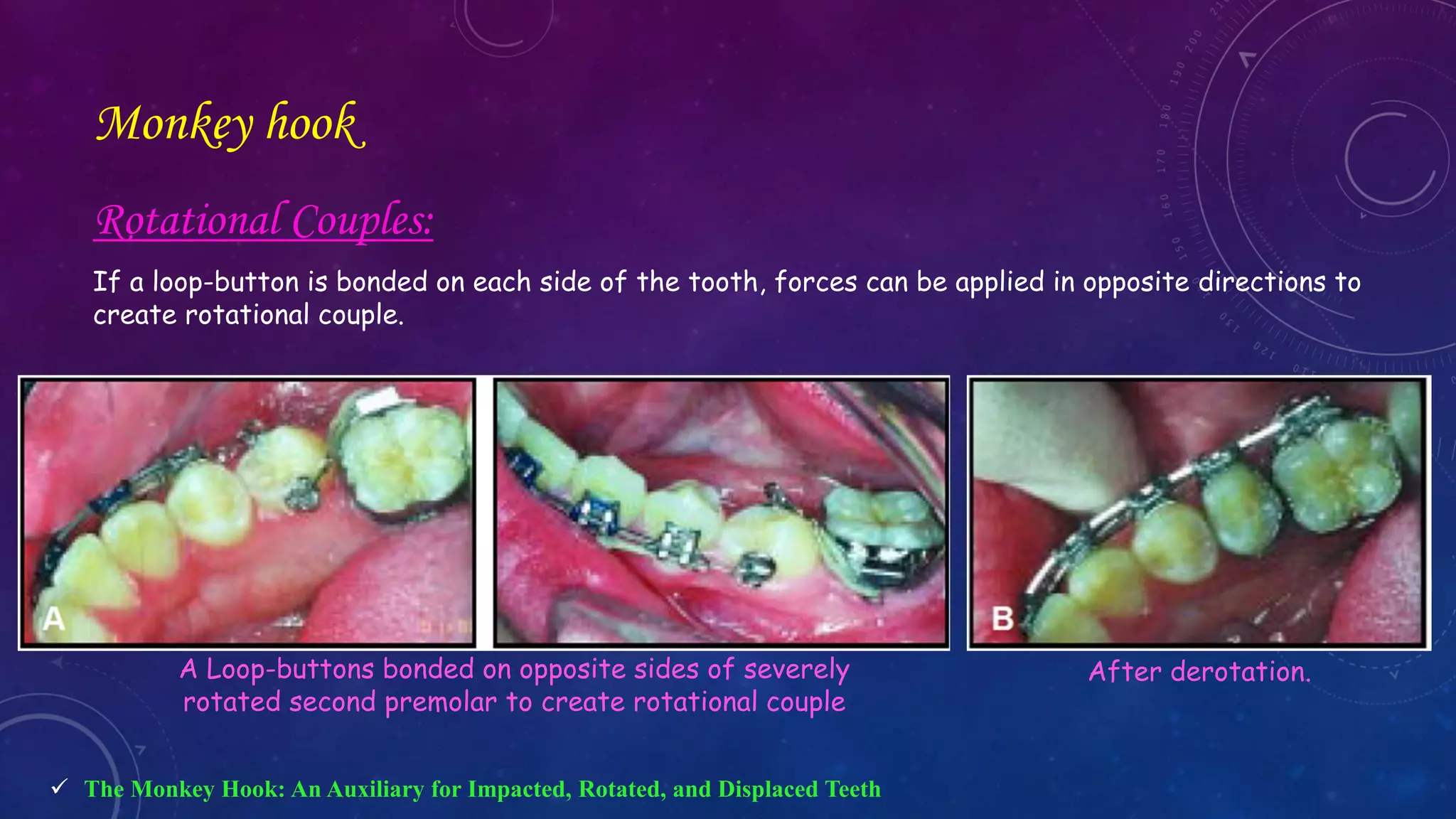





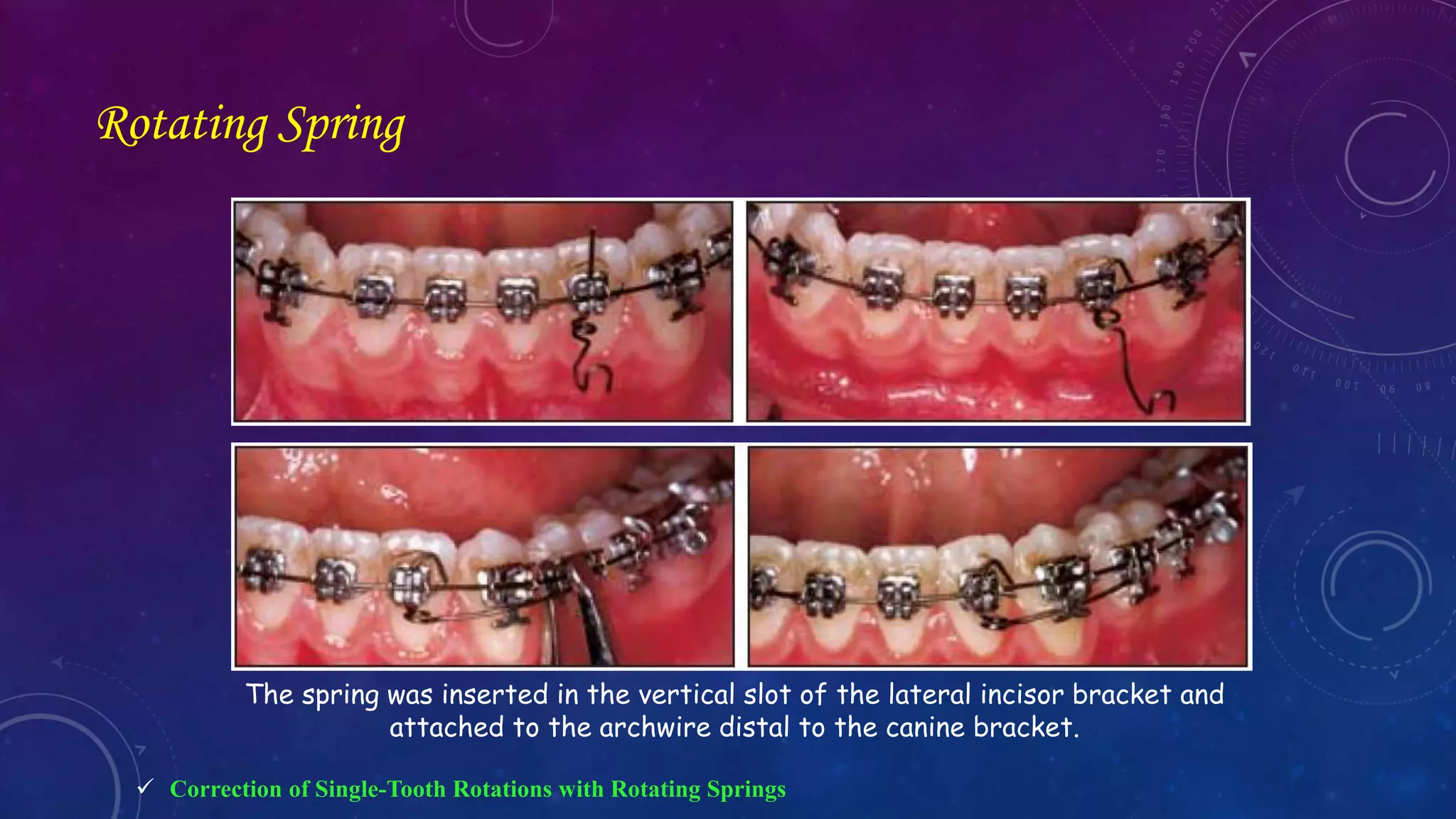


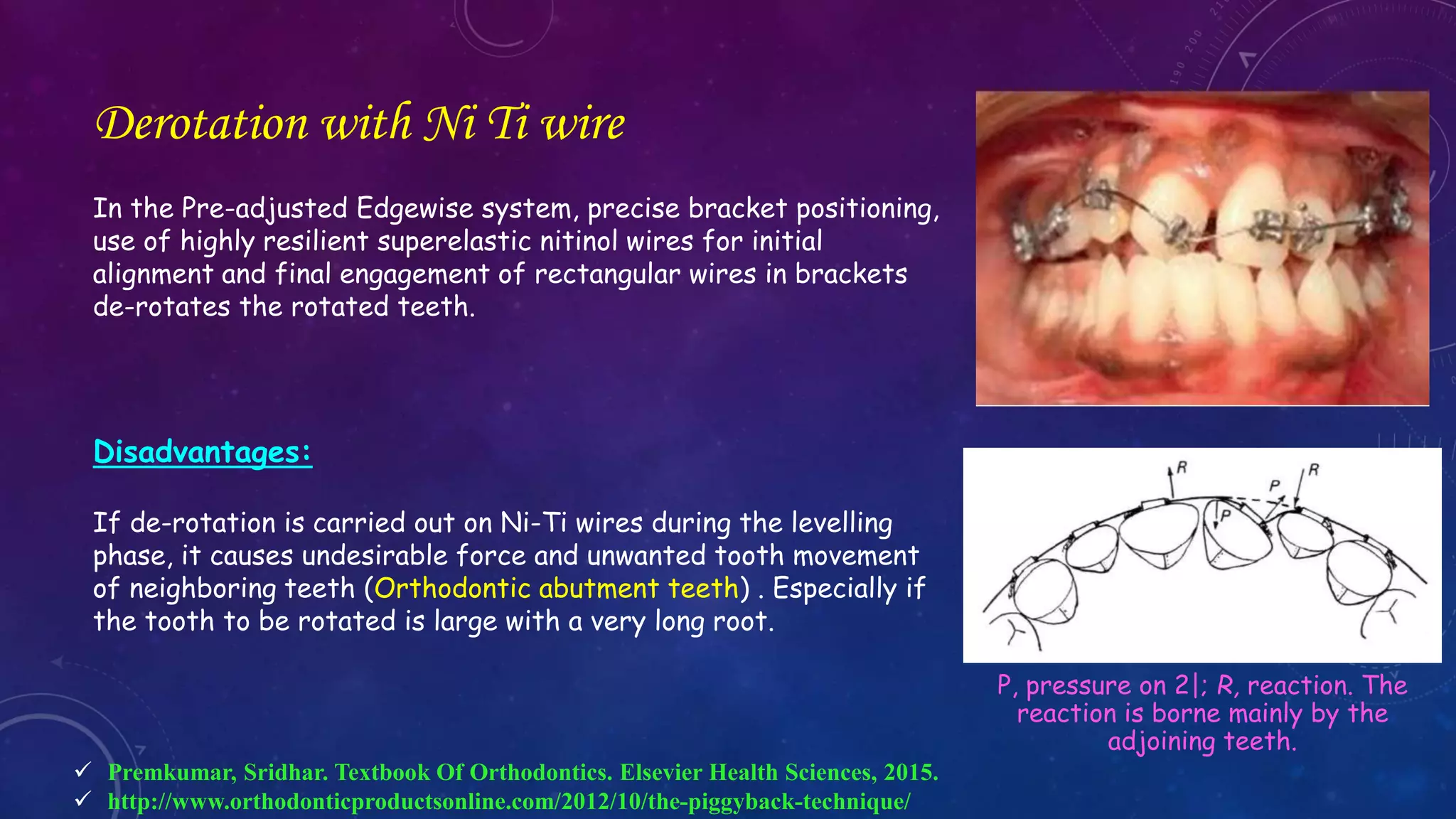

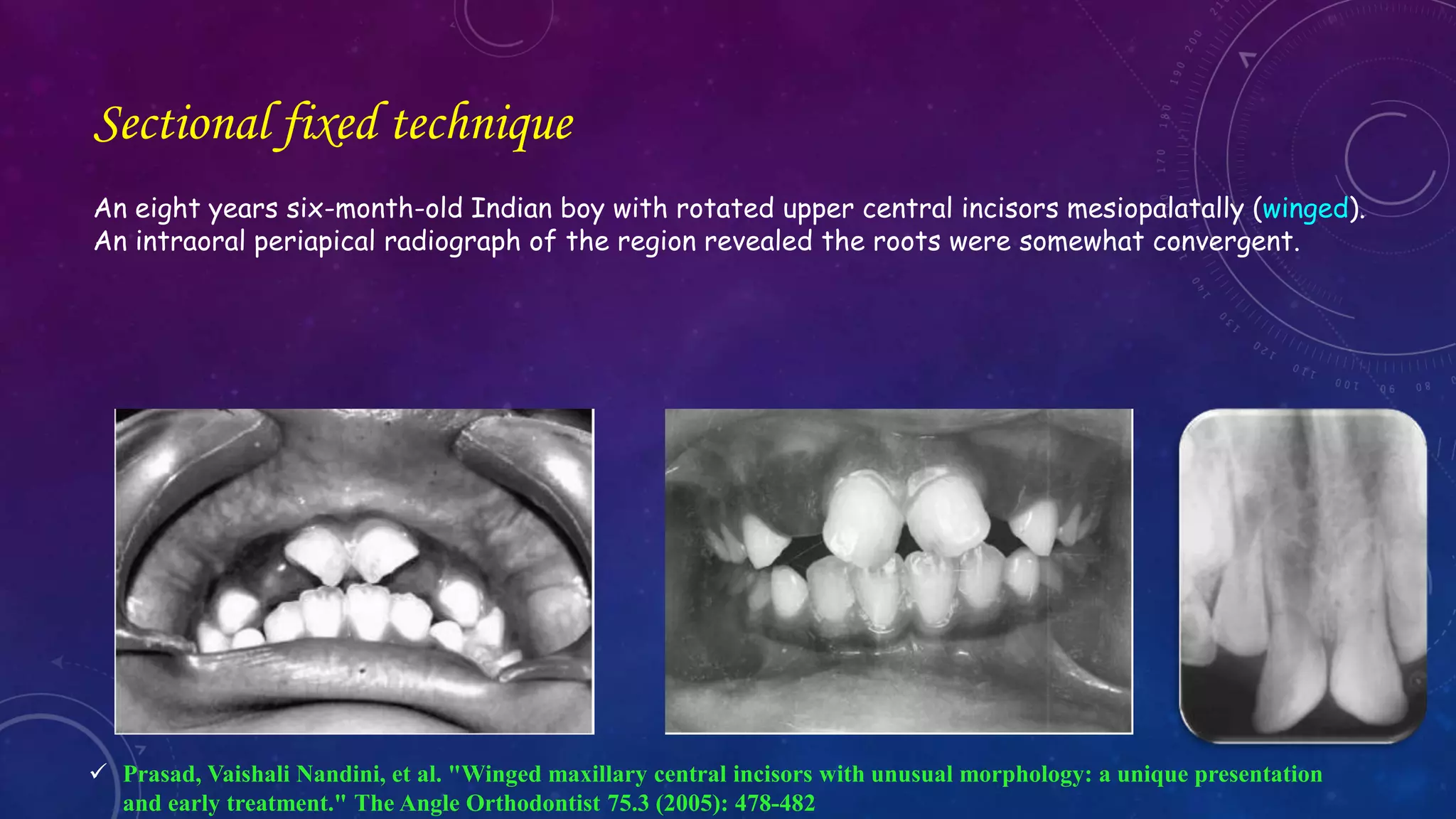

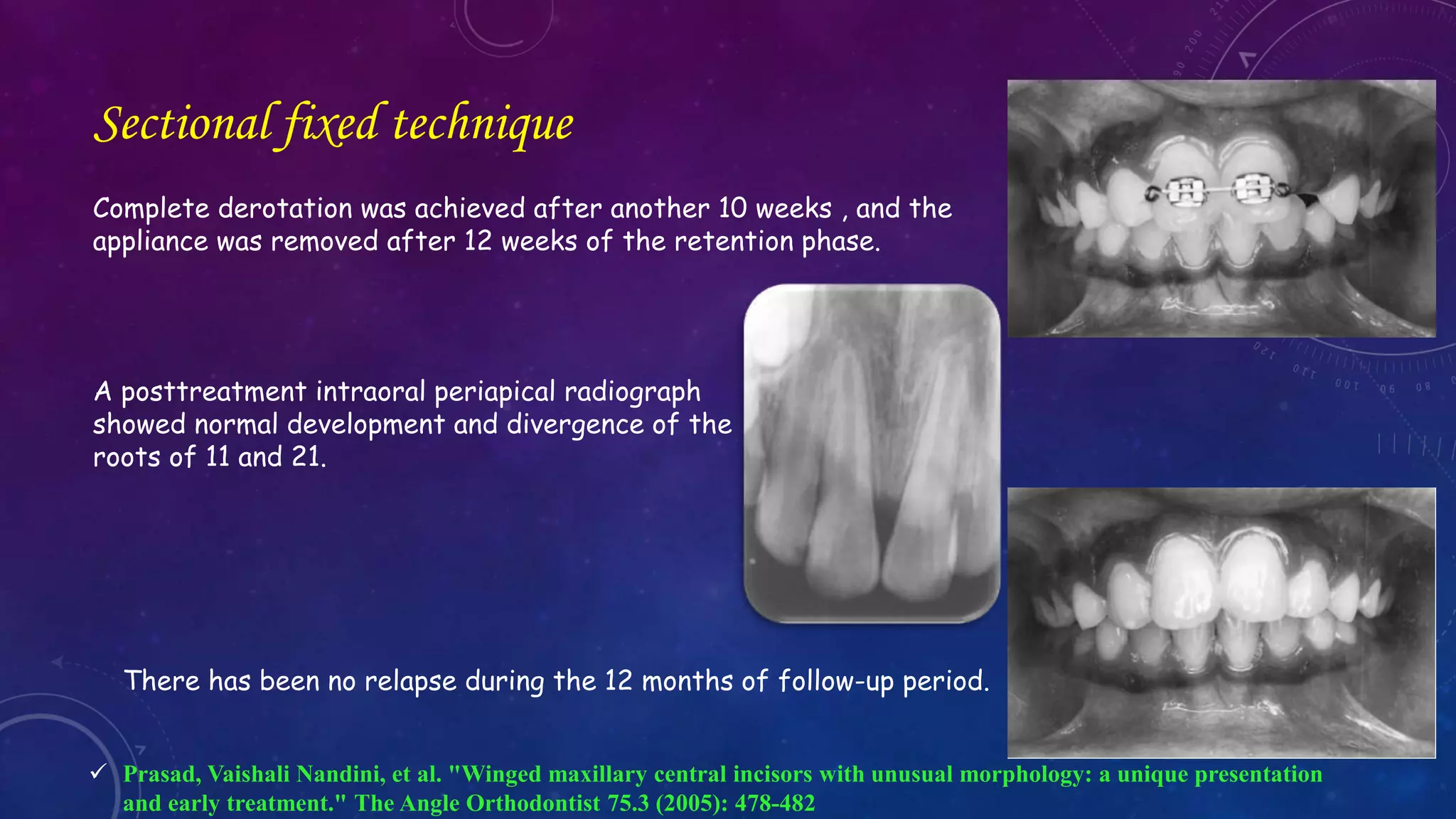











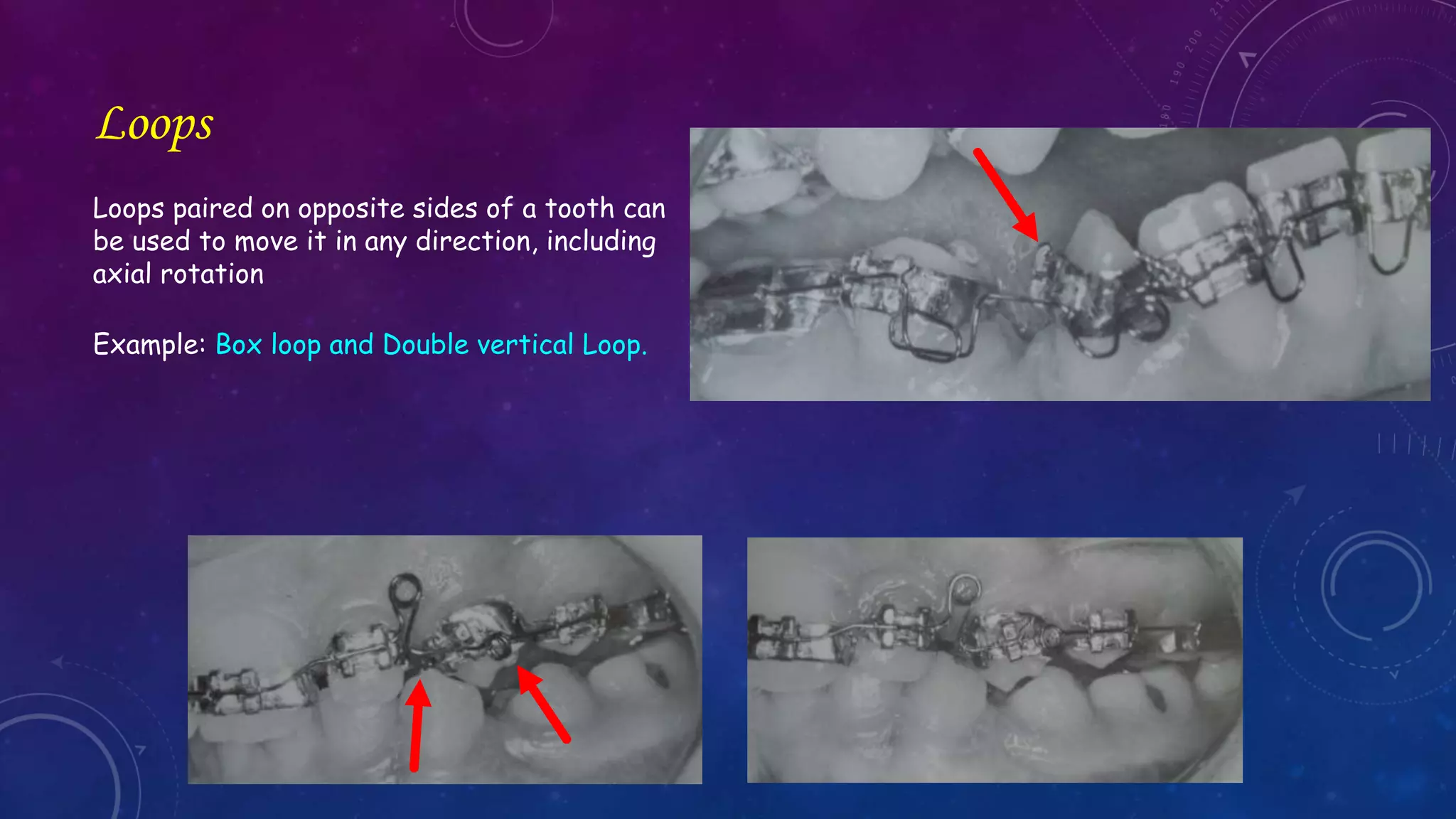

















































































Rotated teeth can be corrected using fixed or removable appliances. With fixed appliances, various ligation techniques can be used to apply rotational forces, including double ligation which ties one bracket loosely and the other firmly. NiTi wires or loops can also be used to derotate teeth around their long axis. Removable appliances are generally not suitable for correcting severe rotations of teeth with rounded crowns like premolars and canines due to the inability to apply proper rotational forces. Early correction of rotations is preferable before root completion to aid retention.



































































