Downloaded 26 times



































































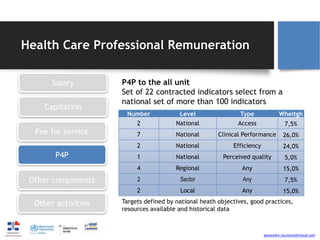










The document discusses the need for reforms in physician compensation systems to improve primary care, highlighting the challenges of current payment methods that often lead to inefficiencies and unsustainable healthcare costs. It emphasizes the importance of aligning incentives with patient outcomes rather than service volume, calling for blended payment methods and value-based care models that prioritize quality and coordination. The text also highlights successful practices from models in other countries, advocating for a patient-centered approach in healthcare delivery.























































































