Download as PDF, PPTX
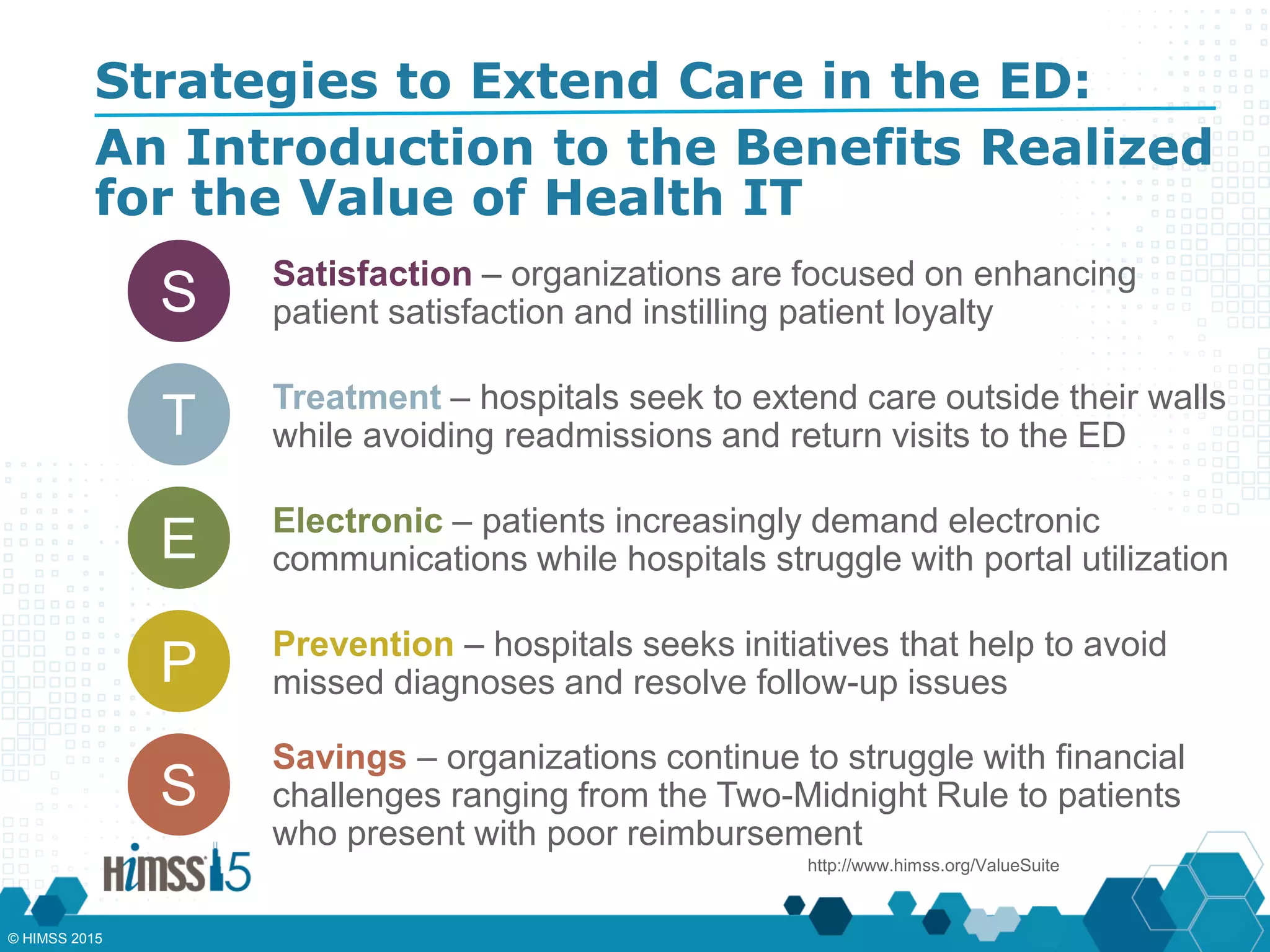
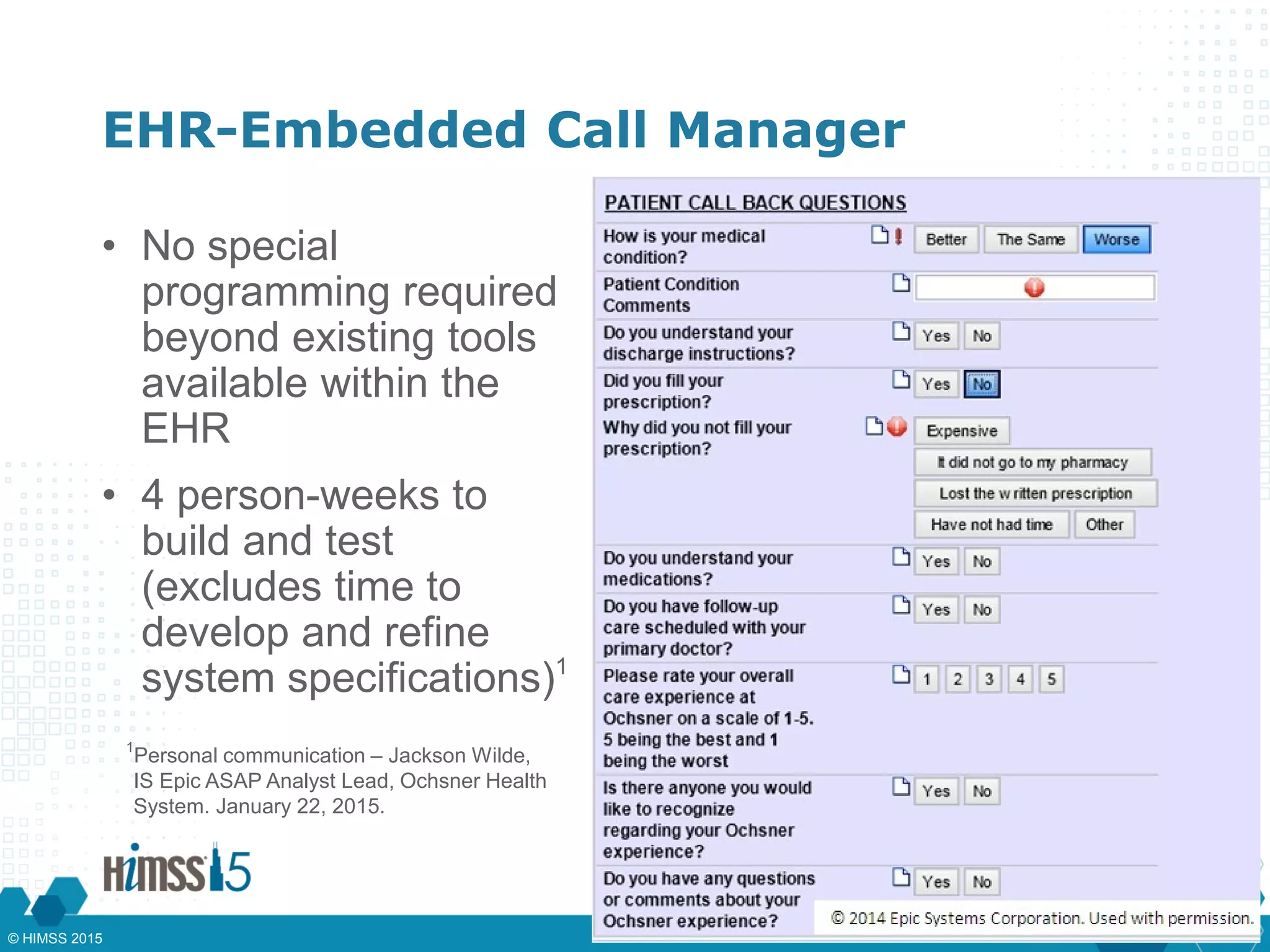
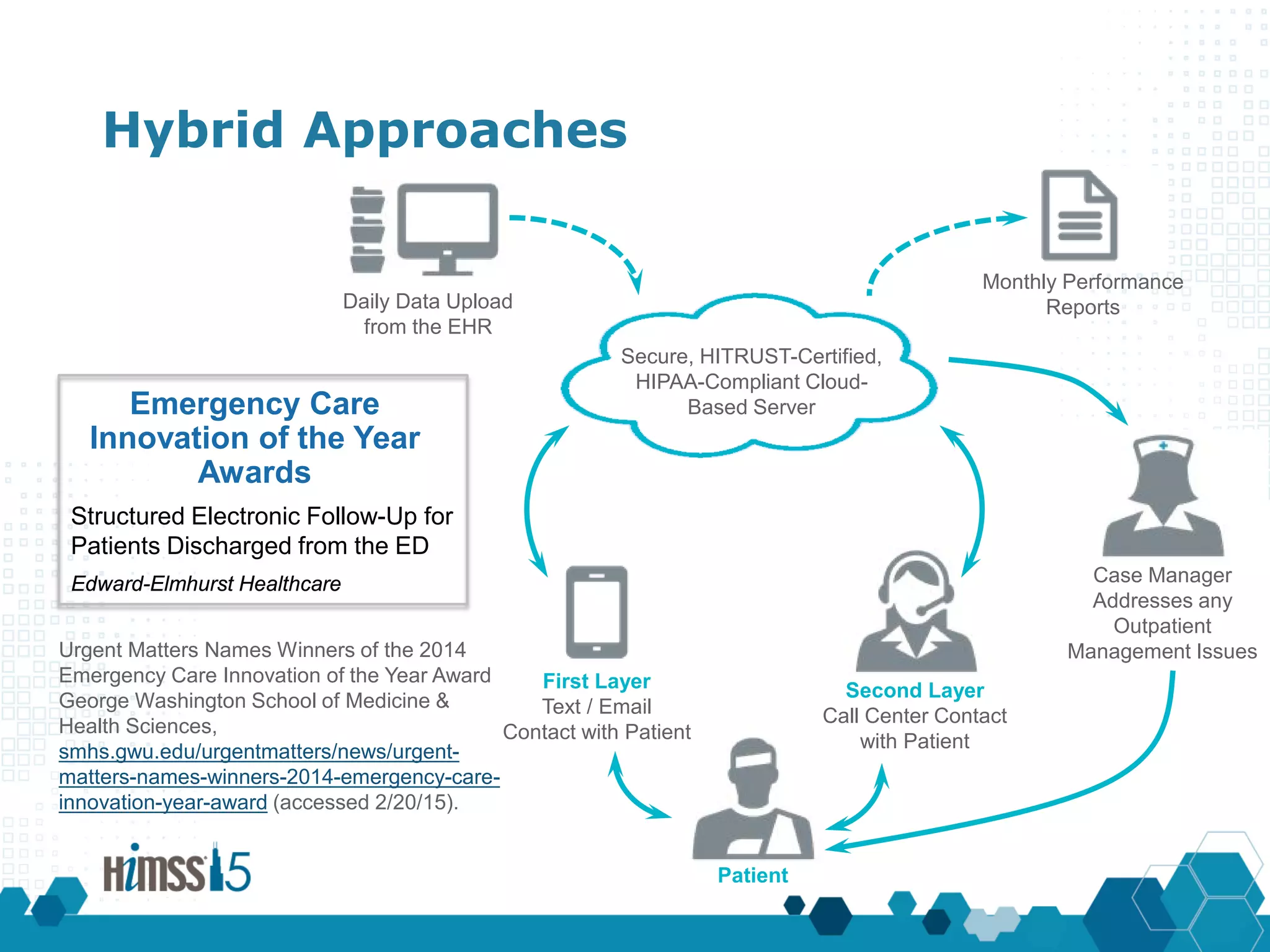
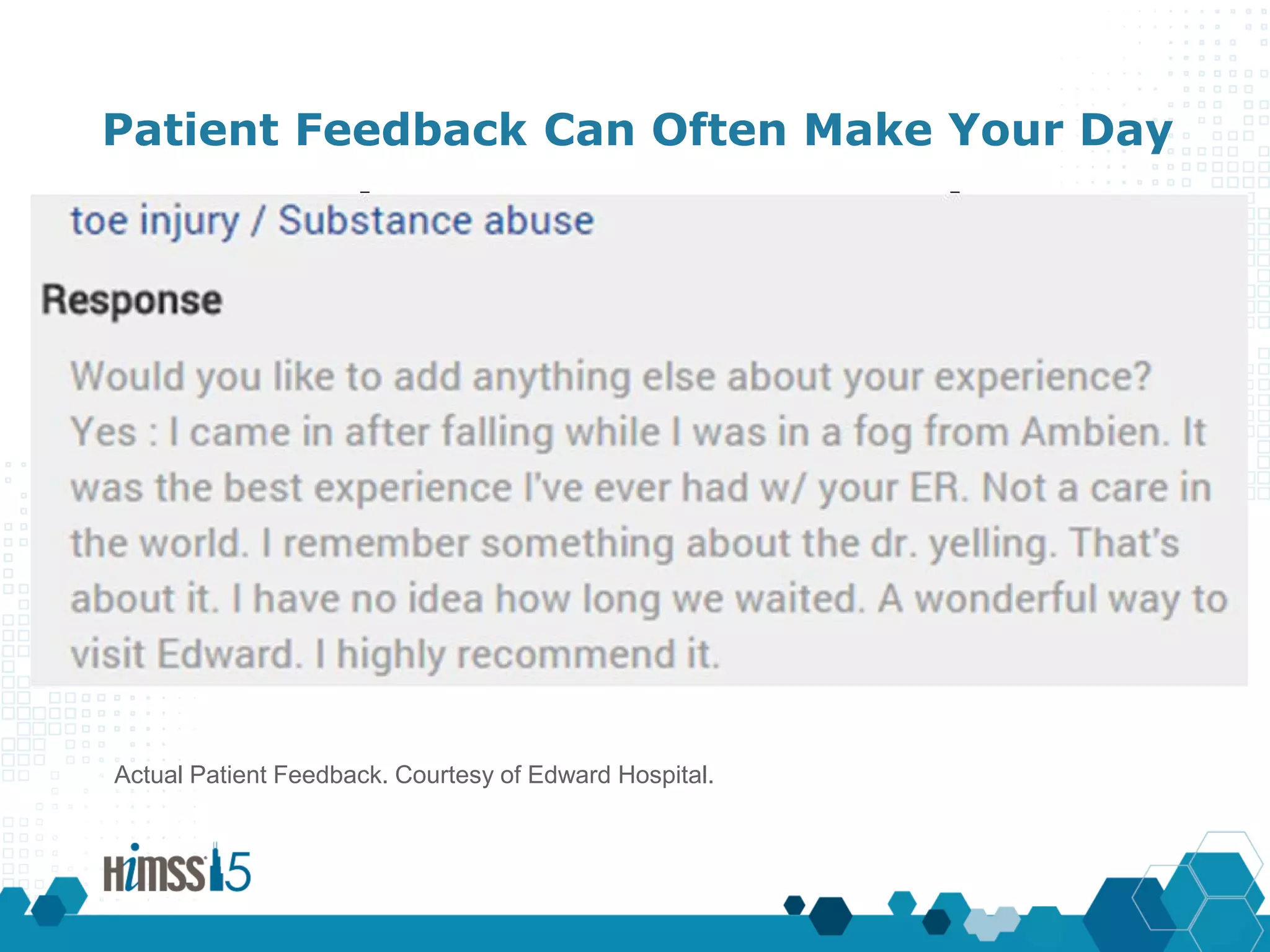
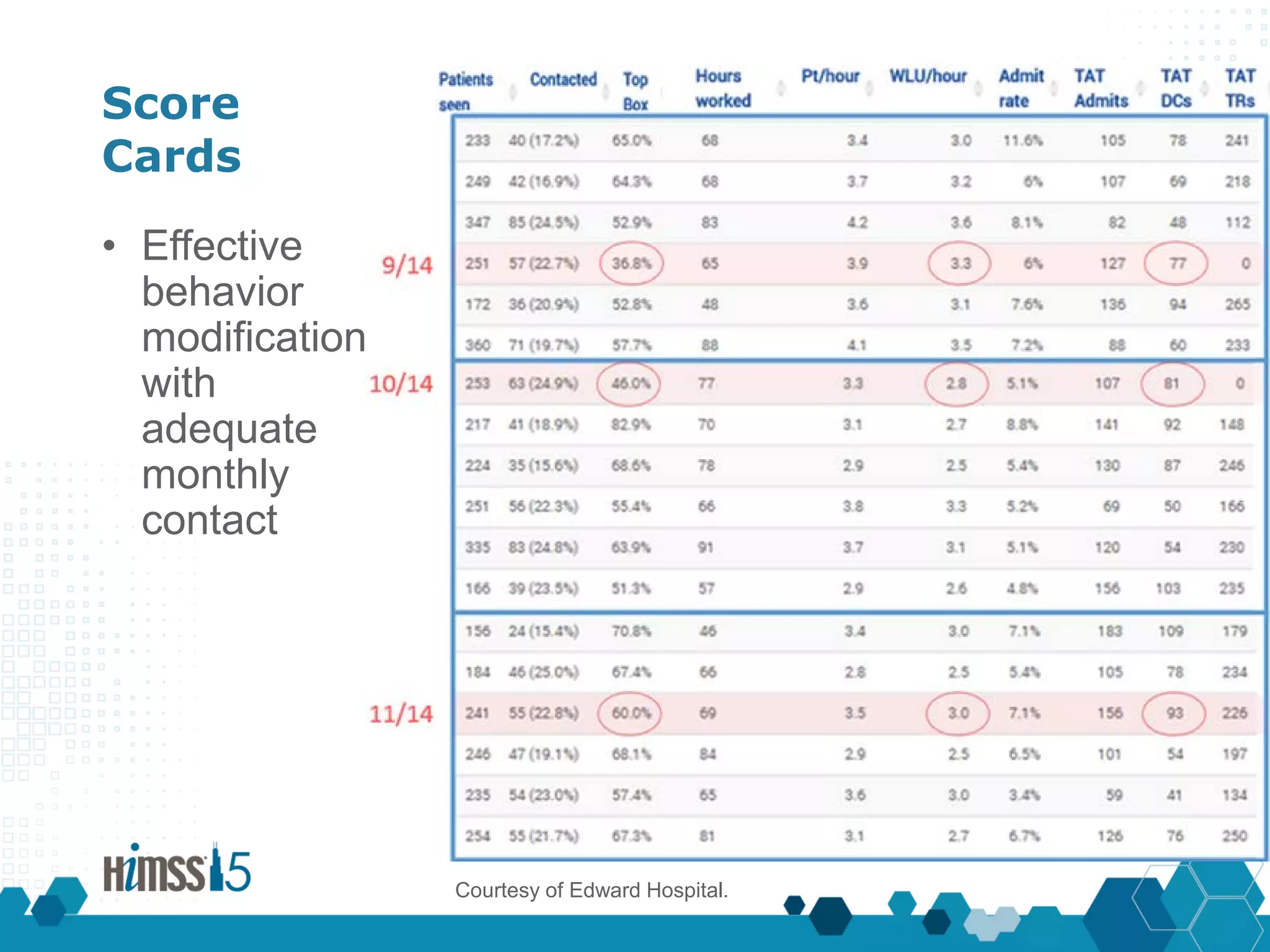
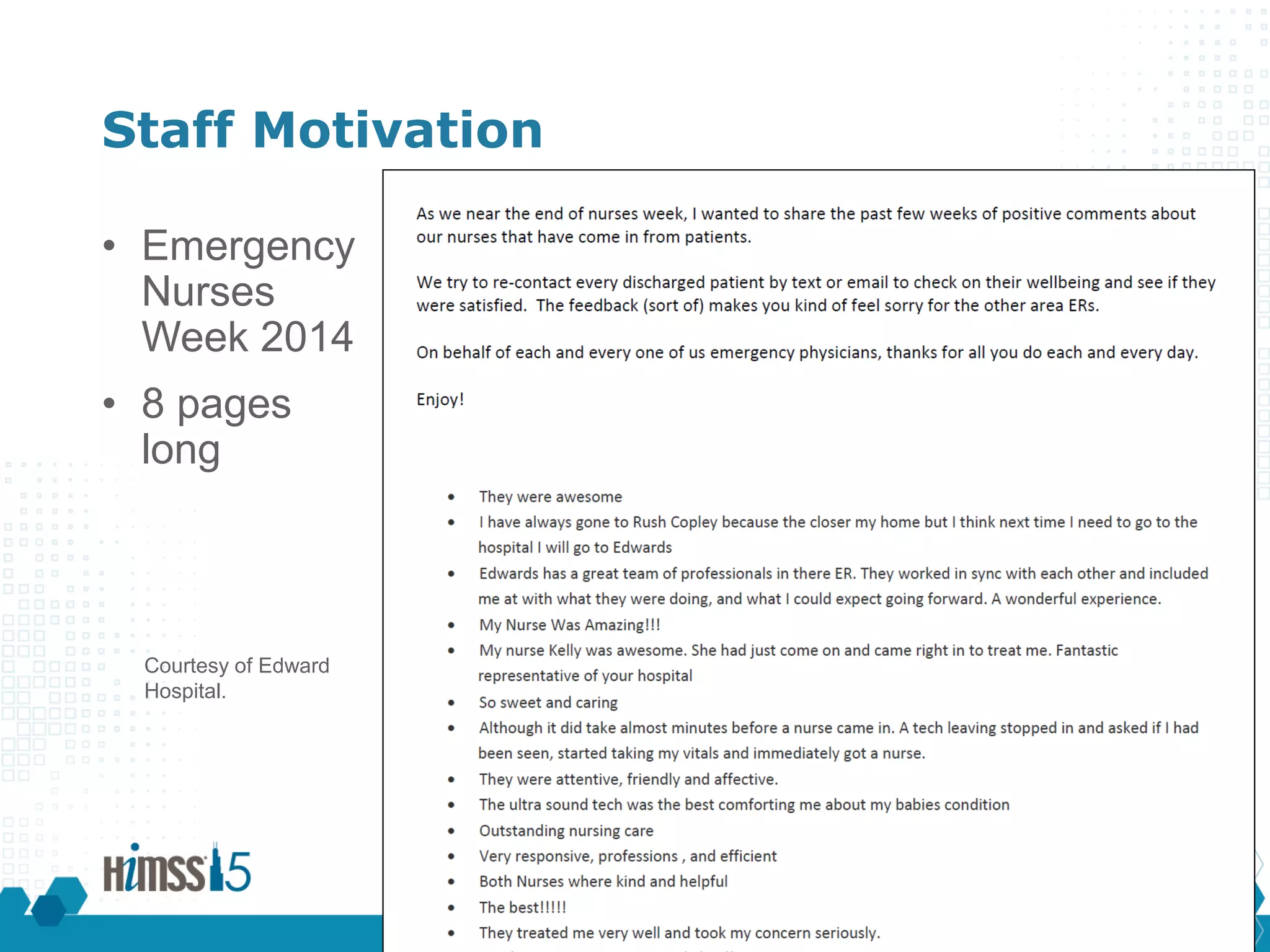
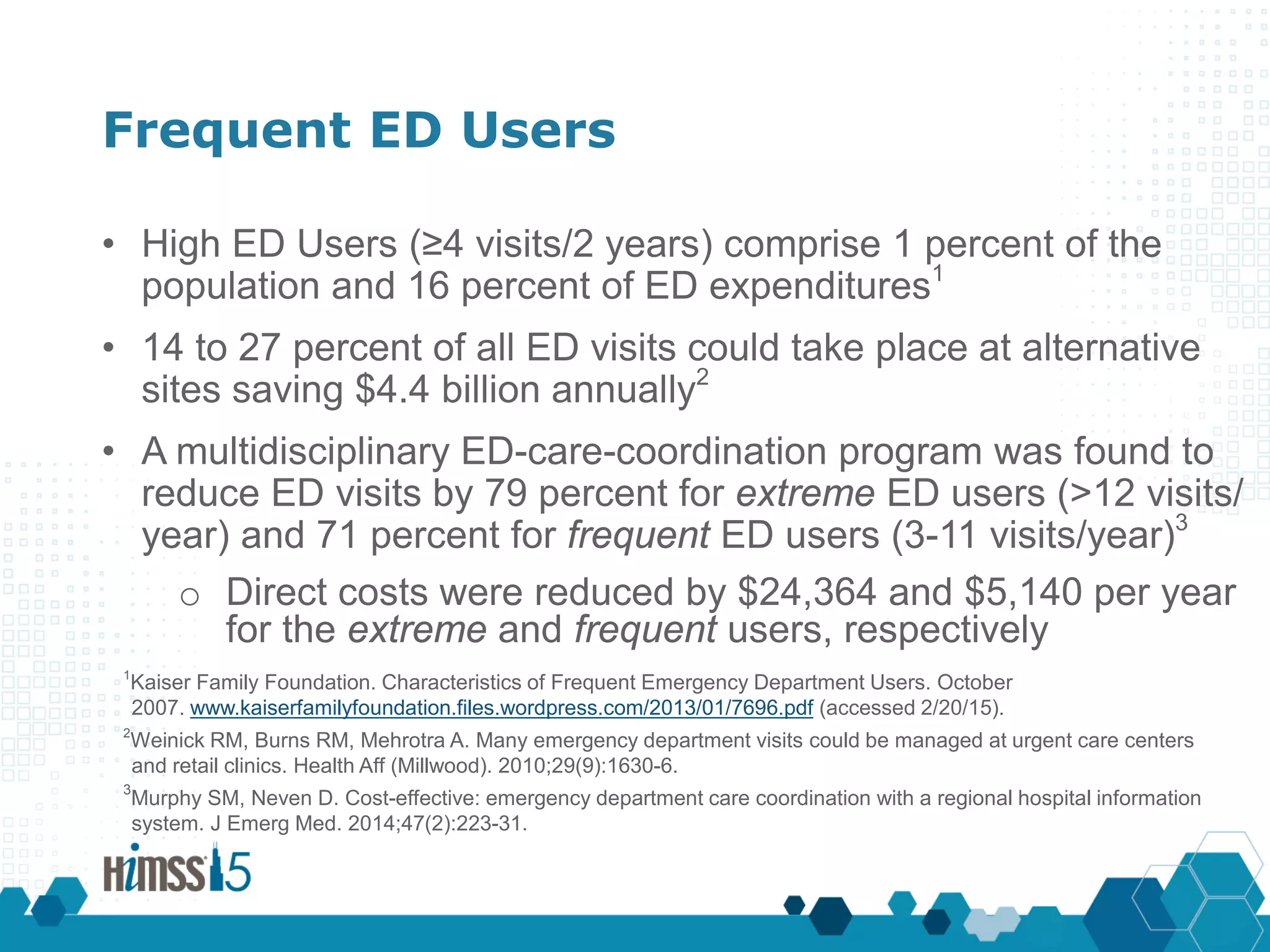
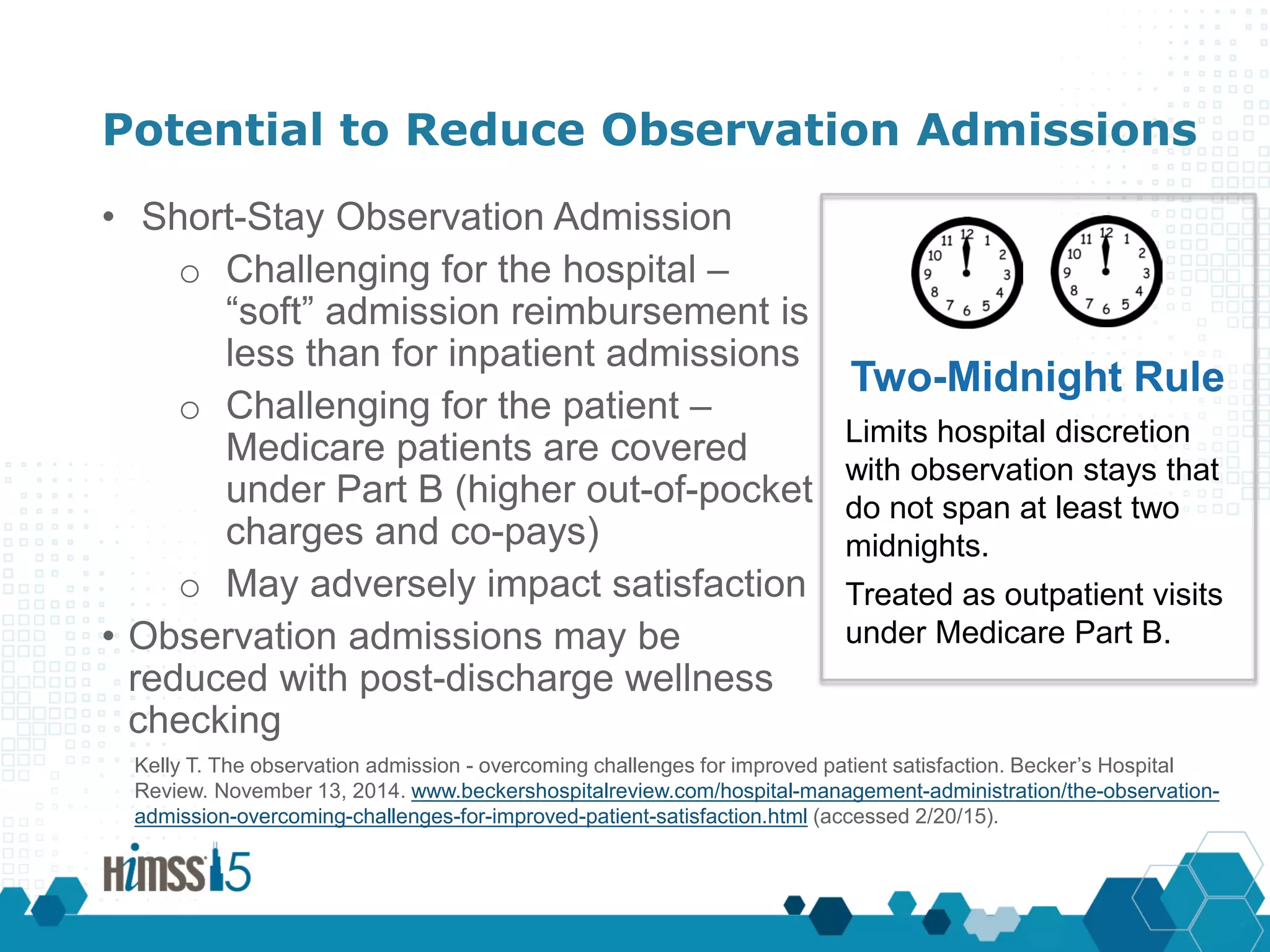
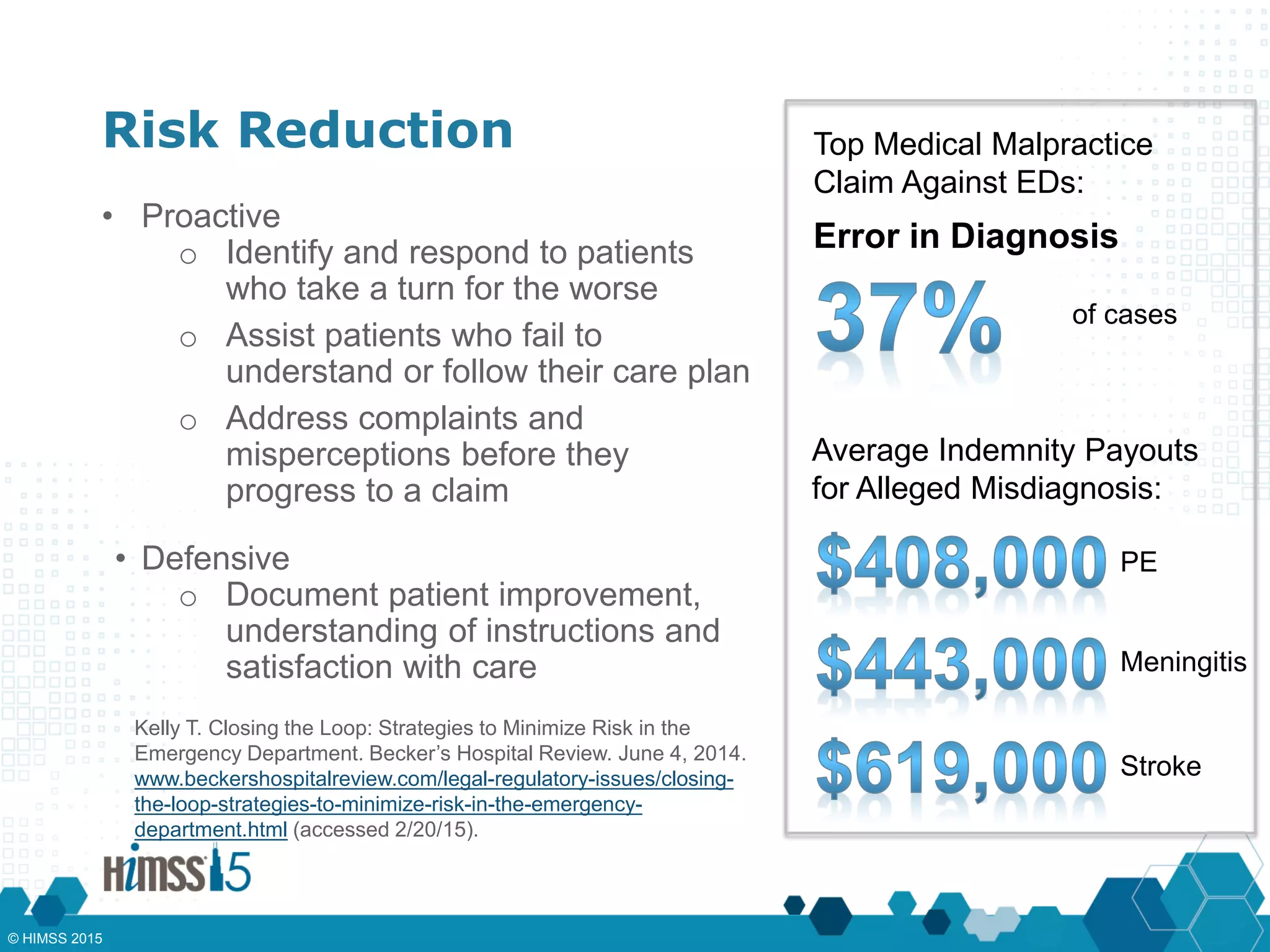
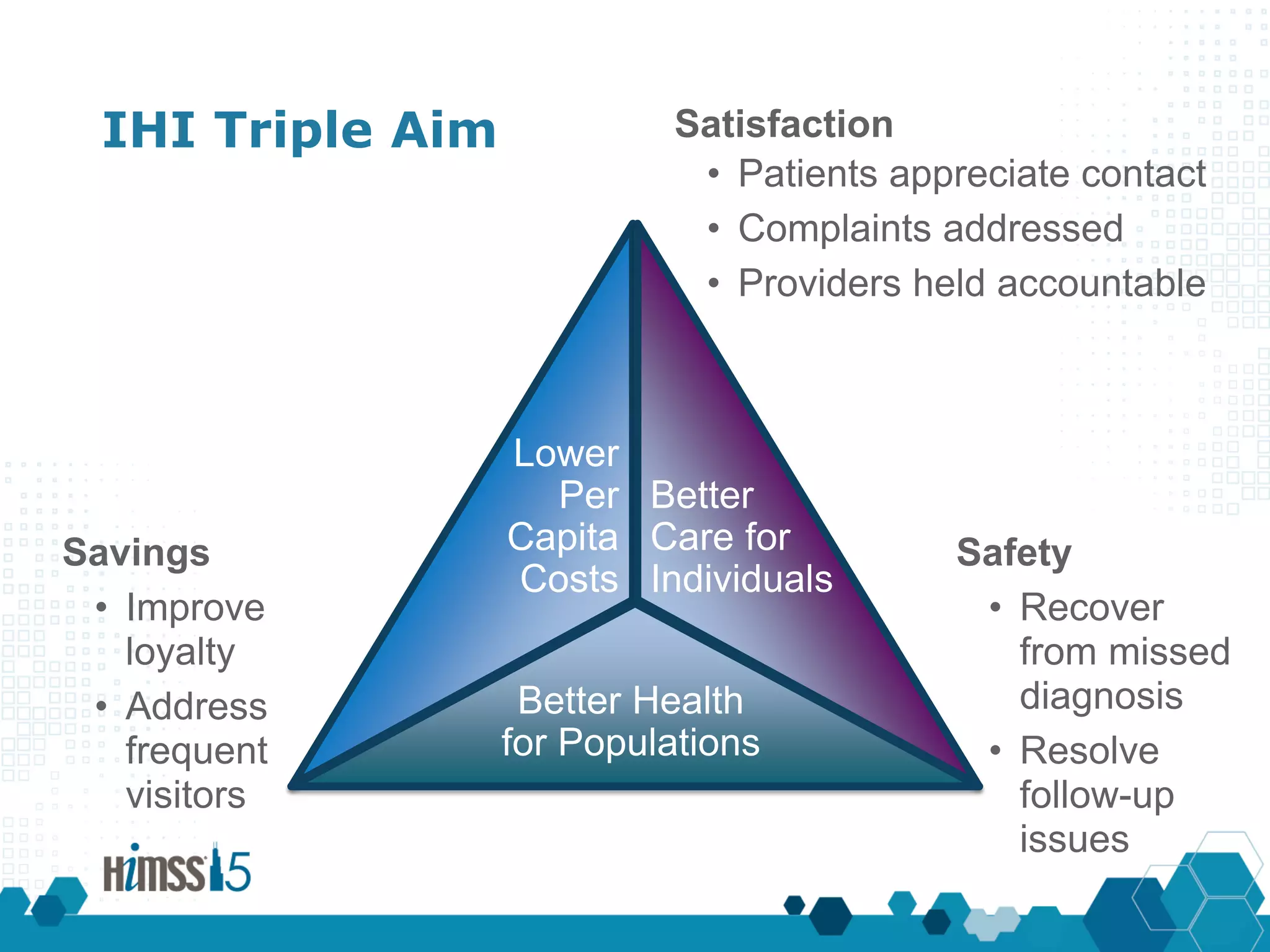
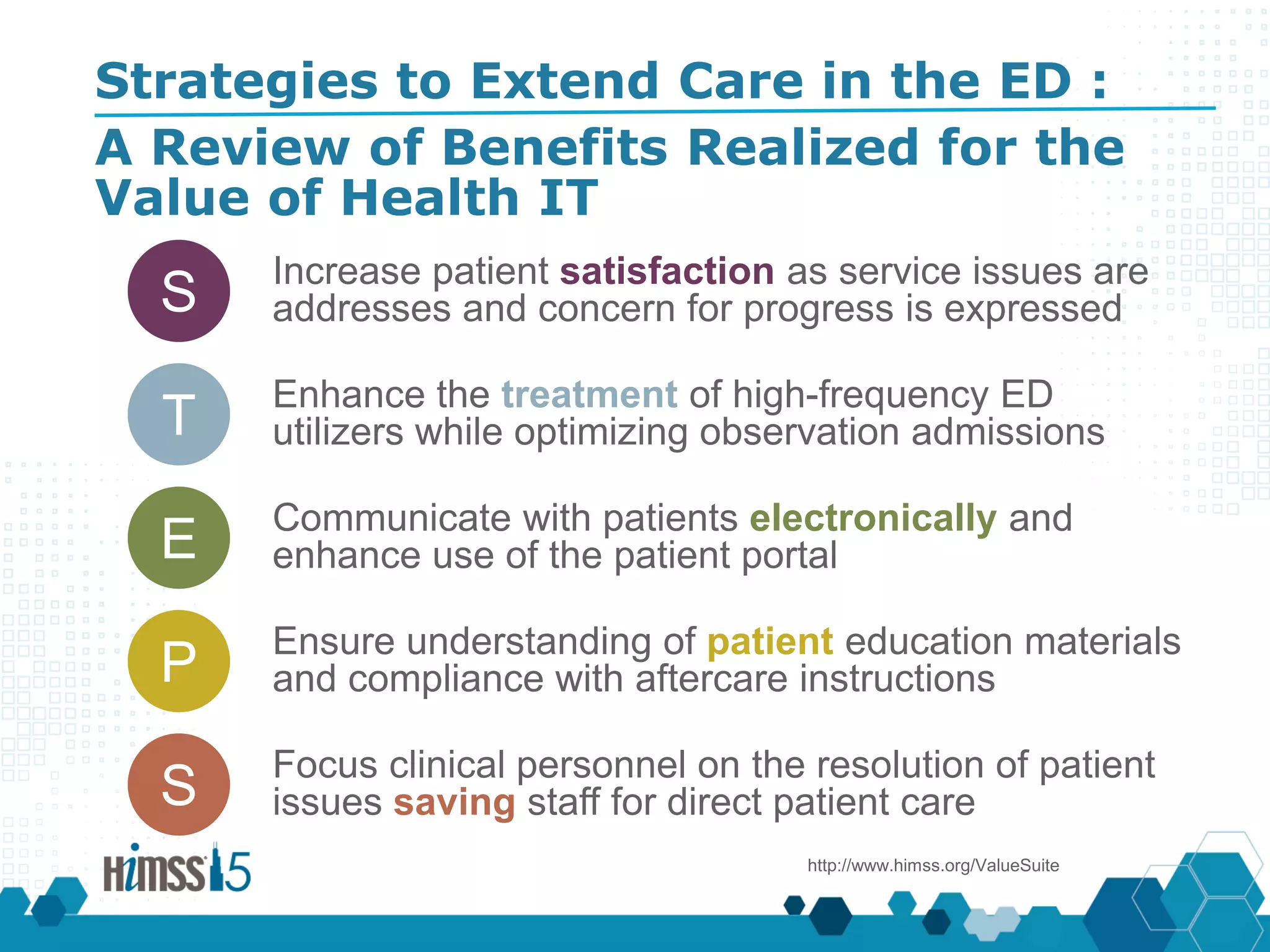


The presentation discusses strategies to enhance patient care post-discharge from emergency departments (EDs) by implementing contact systems that improve patient satisfaction, treatment continuity, and understanding of care instructions. It outlines the unique challenges faced by EDs and the potential benefits of electronic health record (EHR)-integrated follow-up systems, which can identify gaps in care and document patient experiences. Recommendations include incorporating patient feedback through various communication methods to ensure understanding and adherence to post-discharge care plans.











































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)













