Downloaded 11 times

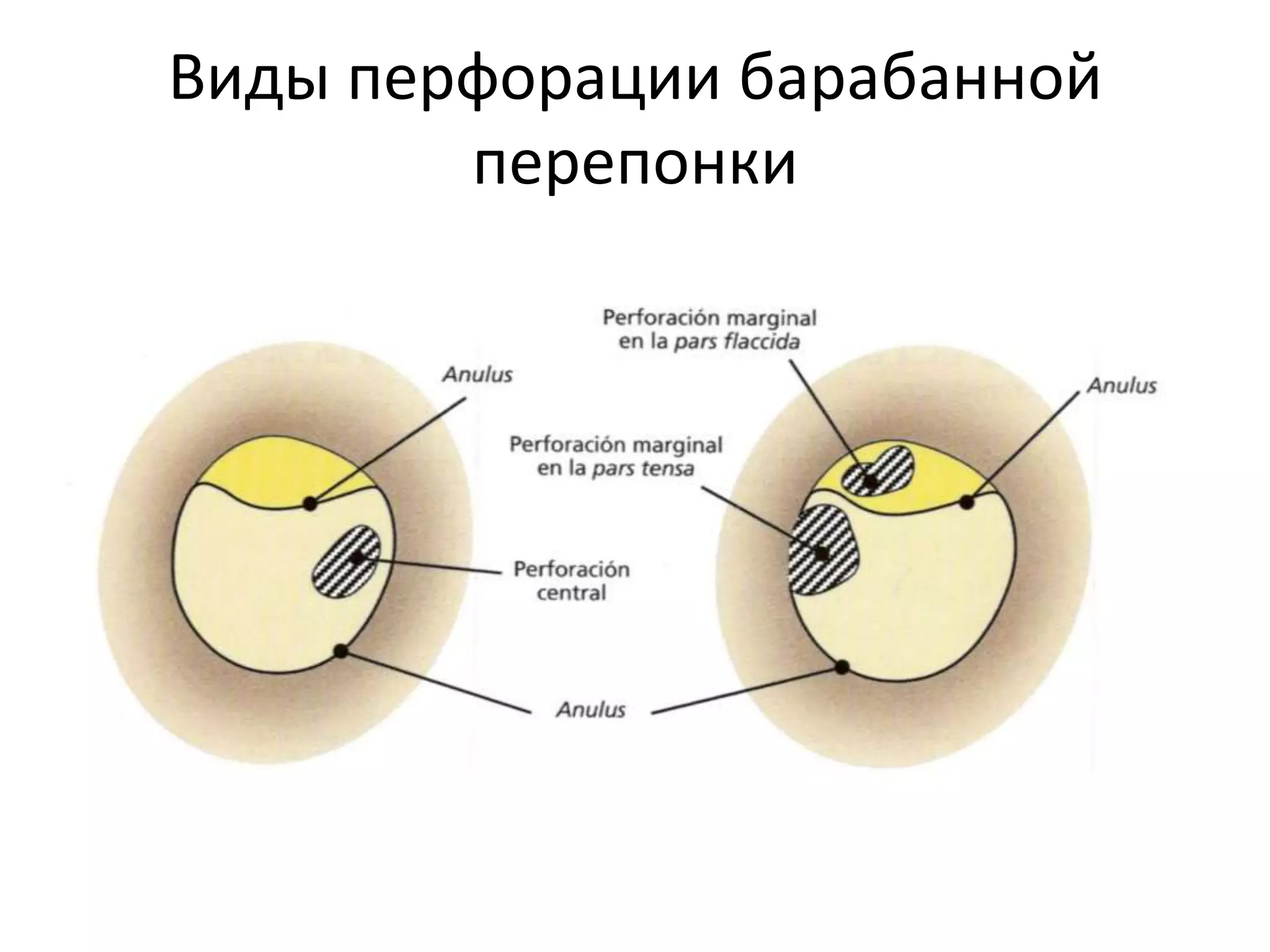
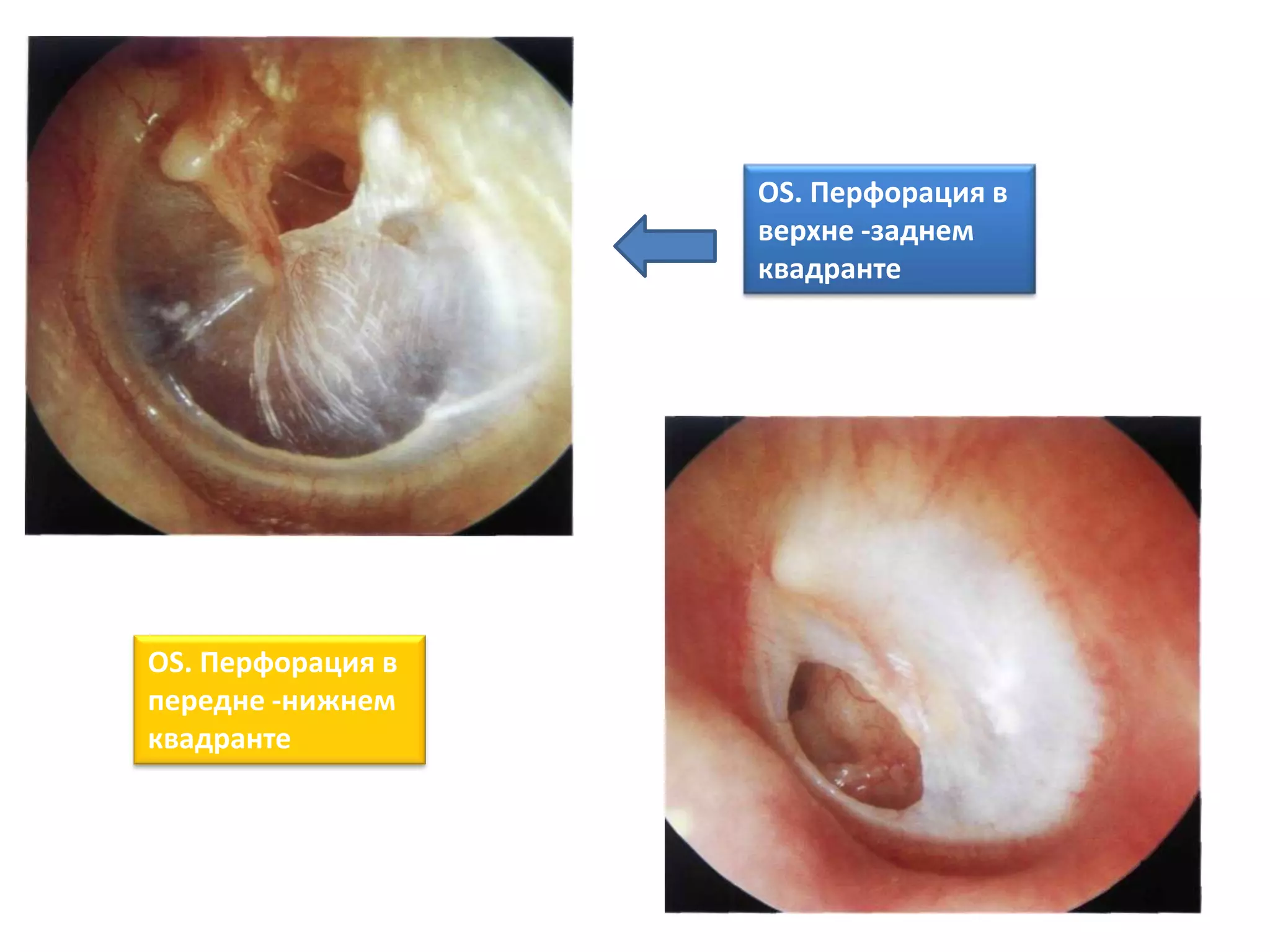
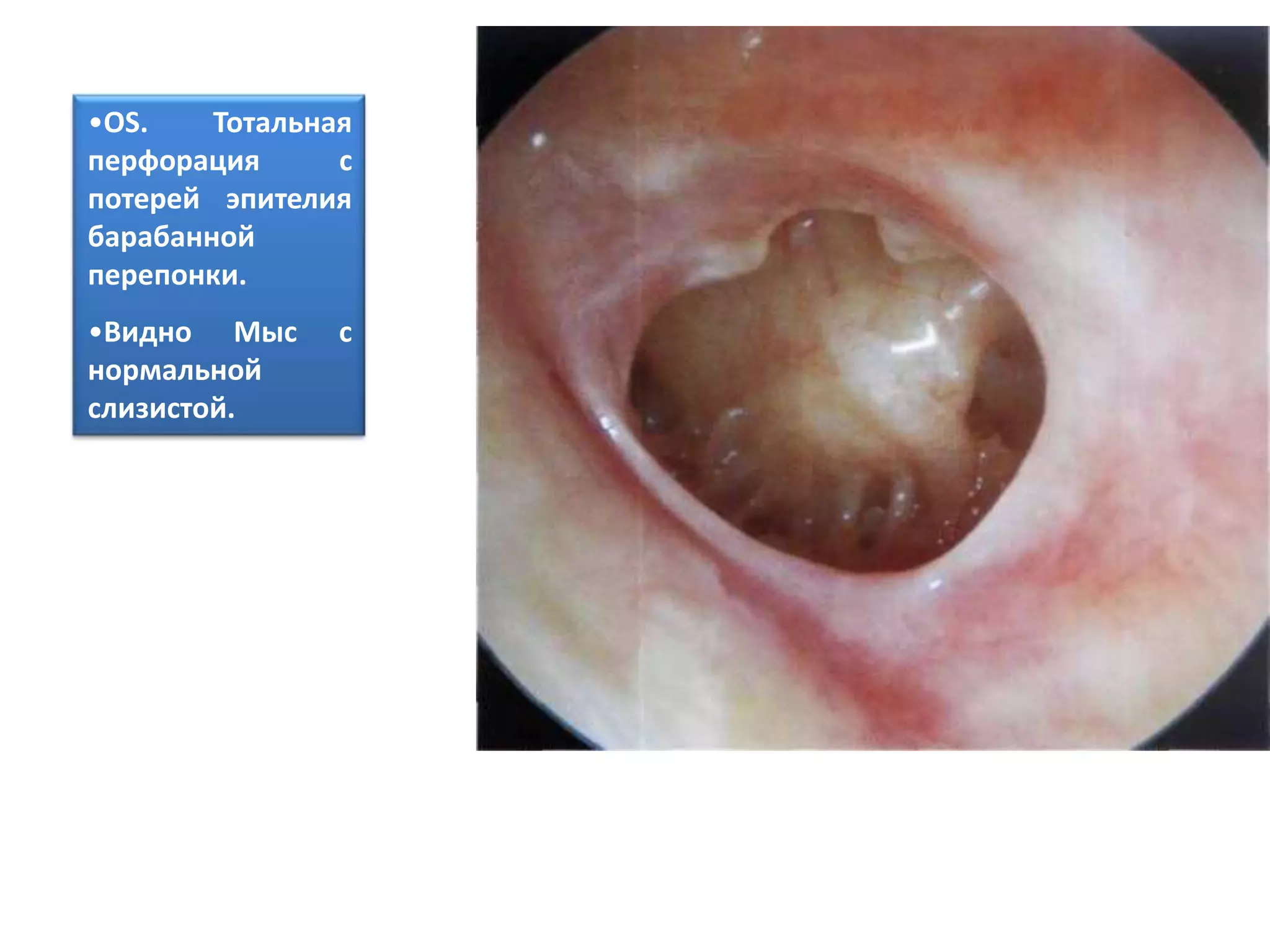
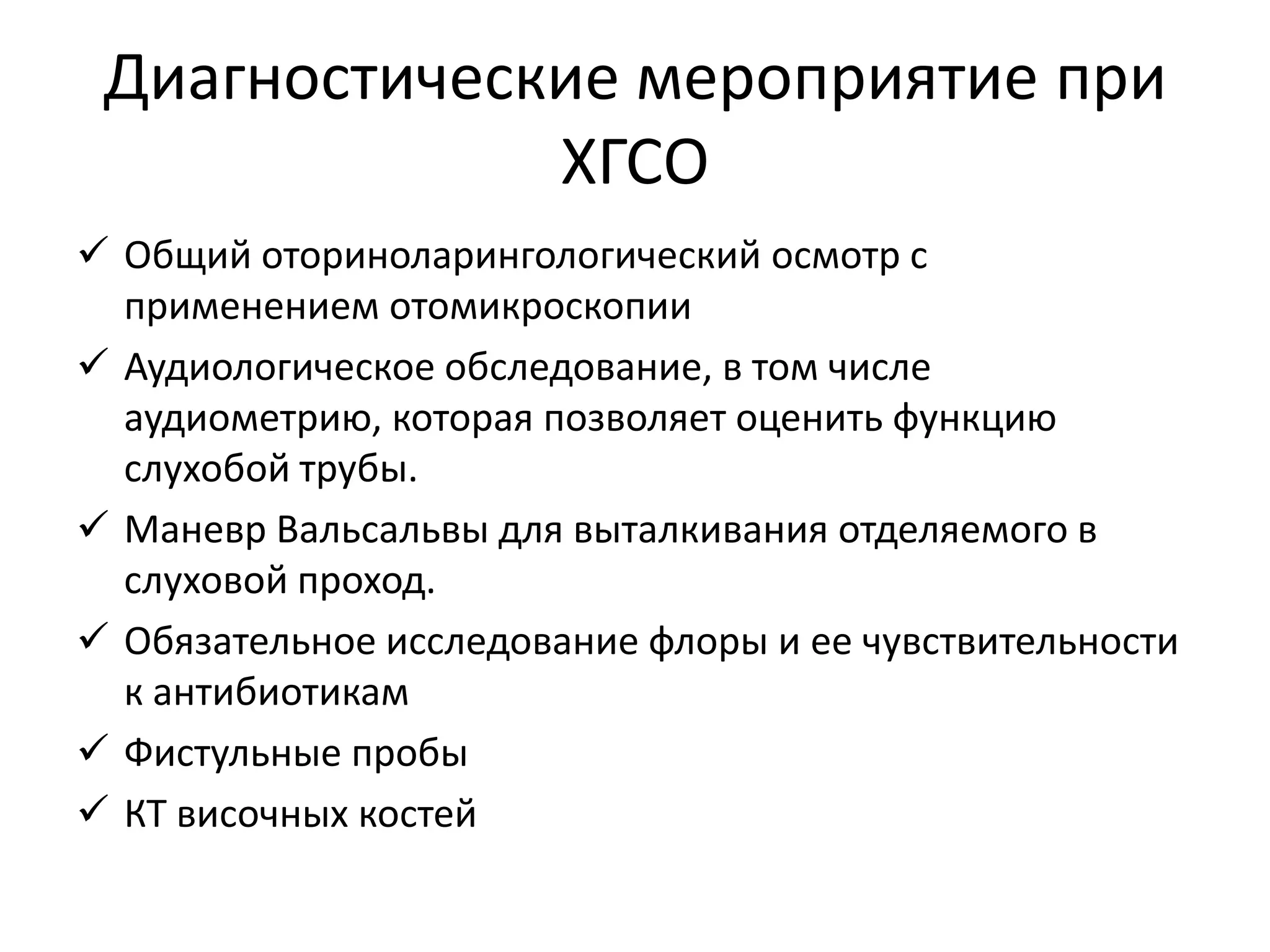
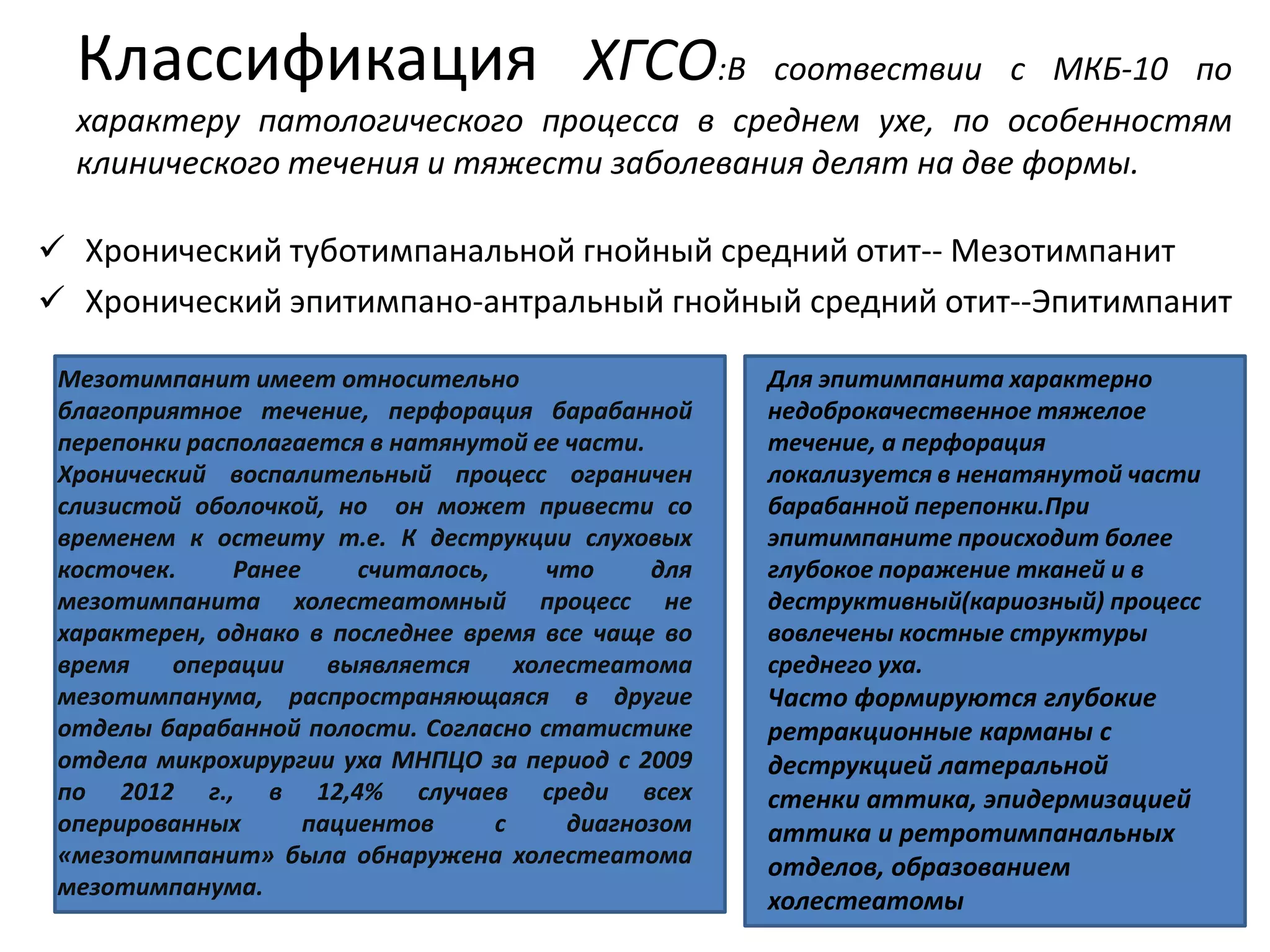

Хронический гнойный средний отит (ХГСО) характеризуется стойкой перфорацией барабанной перепонки, постоянными или повторяющимися гноетечениями и снижением слуха, затрагивая до 46% населения в разных странах. Основными причинами являются нелеченный острый средний отит и различные инфекции, включая стафилококки и псевдомонады, что усугубляется предрасполагающими факторами, такими как аллергии и анатомические особенности уха. Лечение включает оперативные вмешательства, такие как мастоидэктомия и тимпанопластика, для удаления инфекции и восстановления слуха.




































