
Recommended
More Related Content
What's hot
What's hot (19)
Viewers also liked
Viewers also liked (20)
Similar to Special Report- TFQCDM-UPDATED-8
Similar to Special Report- TFQCDM-UPDATED-8 (20)
Special Report- TFQCDM-UPDATED-8
- 1. 1 SPECIAL REPORT Challenges in the Conduct of Health Disaster Response Studies: Consensus Statement by the Task Force for Quality Control of Disaster Management (TFQCDM) Knut Ole Sundnes, MD Chair, Head of Anaesthesia, Norwegian Armed Forces Joint Medical Services; Co-Chairs: Dag Hjelle, MD, Brigadier General and Director Norwegian Armed Forces Joint Medical Services; Ernesto A. Pretto, JR. MD, MPH, Professor of Clinical Anesthesiology, University of Miami Miller School of Medicine; Edmund M. Ricci, PhD Professor, Graduate School of Public Health, University of Pittsburgh; Jeffrey Arnold, MD, Chief Medical Officer Santa Clara Valley Health and Hospital System, Santa Clara County, California, US; Yasufumi Asai, MD Emeritus Professor, Sapporo Medical University, Japan Special advisor of Japan Disaster Relief (JICA) and Editor in Chief of Journal of Japan Association of Disaster; Robert Balazs, MD Lt. Col Technical Officer (Medical) NATO Operational Logistics Planning and Support Programme Office; Per Morten Boelstad Lt Col. Safety inspector (Infantry) Norwegian Armed Forces joint medical services/risk, safety, preparedness and vulnerability; Felipe Cruz Vega, MD, Mexican Institute of Social Security, Special Health Projects Division; Siddarth David Senior Research Officer, School of Habitat Studies, Tata Institute of Social Sciences (TISS), Mumbai; Michel DeBacker MD, Prof. Dr. Director, Disaster Medicine Unit Research Group on Emergency and Disaster Medicine, Faculty of Medicine and Pharmacy Vrije Universiteit Brussel Laarbeeklaan, Belgium; Hon. Emmanuel de Guzman, Philippine Climate Change Commissioner, Philippine climate Change Commission, San Miguel, Manila, 1005 Philippines; S.William A. Gunn, MD Former Director Emergency Humanitarian Operations, WHO, Geneva and member Academic Council of the United Nations System; Christian Haggenmiller, MD; Omar Juma Khatib, MD; Leo Klein, MD Assoc. Prof. Brigadier General MD., PhD, Former Surgeon General of the Czech Armed Forces, Dept. of Military Surgery, Faculty of Military Health Sciences, University of Defence, Charles University Teaching Hospital, Czech Republic; Istvan Kopcso Brigadier General, Dr, PhD Medical Advisor Supreme Headquarters Allied Powers Europe Belgium; Isidore K. Kouadio, MD, PhD, FETP, DMHA Regional Polio Certification Officer Global Polio Eradication Initiative, WHO Regional Office for Africa, Brazzaville, Republic of Congo; Håkon Lund, MD, Lt Col ,Seniorrådgiver and Senior Staff Officer, Norwegian Armed Forces Medical Services; Ove Njå PhD Prof. University of Stavanger; Nobhojit Roy, MB, Prof & Head of Surgical Services and Scientist 'G' BARC Hospital (Govt. of India), HBNI University, Mumbai; Sidika Tekeli, MD Asst. Prof. Dr. Head of Department Hacettepe University Institute of Public Health Department of Health Management in Disasters, Turkey; Andreas Ziegler, MD MSc EMDM MBA, Vienna Municipal Ambulance Service. Please address correspondence to: Knut Ole Sundnes MD, (kosundnes@gmail.com) and Ernesto A Pretto, Jr. MD, MPH (eapretto@med.miami.edu)
- 2. 2 ABSTRACT Background: A goal of disaster medicine is the conduct of studies to enable evidence-based learning that will translate into prevention or reduction of the adverse effects of a disaster on human health and the health system infrastructure. However, there is no consensus on priorities or best practice methodology for disaster studies. In this report an international panel of public health experts and disaster medicine practitioners identifies priorities and proposes solutions concerning the design and conduct of such studies. Methods: Interdisciplinary members of the Task Force for Quality Control of Disaster Management conducted field studies after numerous large-scale disasters. We convened a series of workshops with public health researchers and disaster medicine practitioners to analyze the literature and deconstruct the health and medical aspects of disaster response to achieve consensus on priorities and methodology for disaster response research. Findings: We have identified research priorities and proposed guidelines for a consensus on the adoption of a ‘mixed methods’ approach to broaden the scope and improve the quality of evidence- based research in disaster medicine. Interpretation: A universal consensus on study priorities and mixed-methods approach to disaster medicine research will improve data collection and facilitate the uniform reporting of data for creation of data banks and registries for comparison of all hazard disaster types. This will improve the scientific rigor of disaster research to better enable the translation of evidence-based knowledge into cost-effective programs for the prevention and mitigation of human suffering in all-hazard events. INTRODUCTION Disaster medicine is a newly emerging and interdisciplinary medical specialty. It is comprised of two major domains within health care, emergency public health (EPH) and emergency medical services (EMS). Each domain is characterized by a series of health and medical services delivered to a disaster- impacted population. In many countries these activities are conducted according to a pre-conceived plan and well-elaborated disaster response framework, which includes a concept of operations and detailed descriptions of emergency support functions 1. A disaster response evaluation study is defined as a scientific endeavor to gather evidence to elucidate the causes, circumstances, risk factors and extent of
- 3. 3 human and health system damage during the life cycle of a disaster (Fig 1). A major goal of such studies is the conduct of assessments of the quality of life-saving and life-supporting actions implemented during and after a disaster in order to improve response to future disasters. However, this task has not been carried out in an optimal manner to date due to the complexities of performing research during or after a disaster 2. In this monograph an international panel of experts recognized as the ‘Task Force for Quality Control of Disaster Management (TFQCDM)’ describe guidelines for the study of disaster. These guidelines comprise consensus on priorities and on a combined retrospective methodological approach we consider to best facilitate evidence-based data collection within the complex interdisciplinary framework of emergency public health and disaster response. We have concluded that a combination of evaluative and epidemiological methods blended into a ‘mixed methodology’ is the ideal study design for disaster research. A mixed methods approach can be defined as: “…focus on collecting, analyzing, and mixing both quantitative and qualitative data in a single study or series of studies. Its central premise is that the use of quantitative and qualitative approaches in combination provides a better understanding of research problems than either approach alone.” 3,4 The challenge is to know which tools to apply, when, and for what priorities of study so as to ensure ‘lessons learned’. The guidelines we have developed are based on experiences gained during field survey studies of large-scale disasters during the period 1989-2005 5-19. After each study the scope and the methodology were expanded to incorporate elements of both evaluation and epidemiological research in order to increase the generalizability, applicability and scientific rigor of the methods. To complement experiences gained in these early studies a series of workshops were convened with public health researchers and practitioners to systematically deconstruct health and medical activities commonly performed in the response to disasters and to identify research priorities and the most
- 4. 4 appropriate methodology to achieve study objectives. A critical analysis of previous disaster studies was crucial to the process of establishing priorities and selecting a standard methodology. The result of these efforts is a set of guidelines for evaluation and research of disaster response in the ‘Utstein Style’. The Utstein Style guidelines format was selected because it provides a structured framework consisting of templates (standardized forms) and registries (databases) for the uniform reporting of data to compare disaster responses 20. A first volume of 3 planned volumes of these guidelines has been published previously describing consensus on terminology and concepts: ‘Conceptual framework of disasters’ 21. A second published volume describes consensus on the concept of operations: ‘Structural Framework, Operational Framework and Preparedness,’ 22. The 3rd volume in this consensus project will focus on ‘Methodology’. An abbreviated description of that methodology is presented herein for review and feedback. STUDY PRIORITIES Pre-Event Phase: A scientific assessment of the severity of impact of a disaster on a community cannot be fully realized unless we can collect baseline data on community-wide all-hazard risk planning and preparedness prior to the event under study, as follows: The level of awareness about known hazards by the population at risk. An assessment of the degree of socio-economic development of the community and especially of the health system, its infrastructure and the types and extent of access to health care services available to members of the community on an everyday basis. [The assessment of pre-event status is facilitated by the use of selected World Health Organization (WHO) standard population health indicators (Table 1)]
- 5. 5 An assessment of the structure, organization, adequacy and investments in disaster planning and preparedness programs, and the extent to which these were implemented or tested and achieved stated objectives during actual and/or simulated events.
- 6. 6 Table 1. Template for Assessment of Pre-Event Status Basedon SelectedIndicators of Pre Event Socio-Economic Development and the Post DisasterSeverity Score (DSS). ____________________________________________________________________________________ Checklist: Indicator of Socio-economic Development *Range GDP/per capita income (current U.S.$) Low Middle High Real GDP Growth (%) Low Middle High Proportion of population rural/urban Low Middle High Under 5 Infant mortality rate Low Middle High Maternal mortality rate Low Middle High Life expectancy Low Middle High Literacy rate Low Middle High Proportion of population cell phones/1000 Low Middle High Proportion of homeless population Low Middle High Number of residential structures Low Middle High Number of office buildings Low Middle High Number of hospitals Low Middle High Number of vehicles in use/1000 Low Middle High Annual energy consumption (eq. Kg of oil/capita) Low Middle High ____________________________________________________________________________________ Pre-Event Development Score: * The range of the score prior to the event is based on the total sum for each category: Middle (average among nations): Low = 5 points(poorly developed);Middle = 10 points (Average development);High = 15 points (highly developed) .The change in score before vs after the disasterprovides an estimate of the severity of the disaster on the socio-economic development of the affected community.. Event Phase: Once the event has impacted a population we can attempt a study to determine the degree of damage to the health and health system within the affected community (Table 2). The disaster study should aim to assess human damage and the extent of disruption or destruction of the health system infrastructure. The ideal timing for such studies is immediately after the end of relief and response activities. Evaluative study tools are essential to collect administrative, medical record and interview data from survivors and responders on the quality of overall life-saving activities implemented during the event. For each activity the following categories of information must be collected:
- 7. 7 The structure, process, adequacy, timeliness, outcomes and costs of the damage and of the needs assessments performed on the disaster-impacted community or society; and the process, and cost-efficiency of supplying those needs from within the affected community (local response) or from without (external response). The identification, prioritization and process of implementation of the emergency relief function The structure, process, adequacy, timeliness, outcomes and costs (and possible opportunity costs) of the delivery and management of the health and medical response The outcomes of specific public health and medical interventions to prevent or reduce morbidity, mortality and disability among disaster impacted victims as determined by pre-established standard-of-care end points, as well as the ability or inability of the impacted health system to provide health services to survivors during the event (triage, application of first aid, emergency transport, definitive care, potable water, epidemiological surveillance, etc.) Table 2. Template for Assessment of Pre- and Post-Event Health Status/Health Disaster Severity Score (HDSS) ____________________________________________________________________________________ Checklist: Indicator of Health System Development *Range (Before/After) _____________________________________________________________________________________ Human Impact: Affected Population: # # # Crude Mortality Rate/10,000 # # # Crude Injury Rate/10,000 # # # Health System infrastructure: Number and type of hospitals/capita* Low Middle High Number of beds/capita Low Middle High Number of health care workers/capita* Low Middle High Number of Critical Care beds Low Middle High Average ICU bed occupancy rates (Past 6 months) Low Middle High Number of Ambulances/EMS systems Low Middle High Percent population with access to potable water Low Middle High _____________________________________________________________________________________
- 8. 8 Health Disaster Severity Score: each indicator is given an arbitrary point score – Low (5) - Middle (10) – High (15).The change in the score (before vs. after) is an estimate of the severity of damage sustained by the health system infrastructure (Health Disaster Severity Score). Post-Event Phase: A major priority of the study is the assessment of how the affected community recovered from the event. The priorities during the rehabilitation/recovery phase include the following: Identification, prioritization, timing of initiation and implementation of relief and recovery projects, and whose aim is the resumption of the normal activities of daily living [lifelines (electricity, water, gas, shelter, food distribution, transportation, communication)], as well as the resumption of normal health services, school, work and leisure activities Assessment of the health and medical care costs to restore health care services and for the long term rehabilitative care of the mentally and physically disabled caused by the disaster itself Assessment of the organization, coordination, sources of funding, costs and adequacy of plans to reconstruct societal infrastructure (hospitals, roads, bridges, housing, schools, entertainment facilities, parks, etc.) Study Designand Methods We propose consensus on the adoption of a mixed method design for evidence-based research on health and medical response efforts in a disaster. The study tools employed whether evaluative or epidemiological are based on the questions asked and the character of the information to be obtained (qualitative vs. quantitative) and the objectives and specific aims of the study according to the following considerations: 1) Evaluative methods gather information to be used to assess the quality of the medical and public health services and interventions deployed using pre-established measures of effectiveness
- 9. 9 and/or quality indicators and outcome parameters 23-28. 2) Epidemiological research methods are used to collect concurrent or retrospective quantitative data primarily about the fate of casualties. Whenever possible data collection instruments must be designed a priori to facilitate uniform reporting of data for input into data banks and registries that can be used for hypothesis testing (Table 3). Also, the study design must provide a mechanism for concurrent data collection, which will serve a dual role: a) to monitor the quality of delivery of services during the event and; b) for risk factor analysis in retrospective case control studies after the event. With regard to the implementation of the study, the first phase should involve the following thought process: 1) identification of the problem(s) to be studied; 2) formulation of the questions or hypotheses based on the problems identified, and; 3) validation of the research questions through substantial literature and background research. A primary objective of the study must be to uncover risk factors for adverse health effects of hazards, in addition to the utility and effectiveness of interventions employed to prevent or reduce injury or death. As in any investigative process the findings are only as good as the research questions asked and the methods used to collect reliable data to answer them. Evaluative tools (eg. survey methodology) are applicable for the collection of information from key target audiences who participated in the organization or delivery of the relief and response and to define the parameters of the quality of those activities according to standard evaluation categories 23,24. The following are sample questions to be asked of eyewitnesses in health disaster studies: What was the hazard type? What was its intensity (Richter scale, Saffir-Simpson wind scale, etc.)? What was the population at risk?
- 10. 10 What were the demographic features of the affected population (age, gender) or other important characteristics? Were there secondary disasters (fires, dam burst, landslides, etc.) Was there early warning of the hazard or early warning systems employed? How well did early warning systems function? When and how did victims become identified for care? What types of medical care/surgical procedures were provided to each victim? Who provided the care (lay bystanders, search and rescue, paramedics, physicians, etc.)? What was the outcome or the result of the care provided? What factors worsened the outcome with regard to injury, death or disability? Was the care provided in a timely manner and appropriate for the various injury conditions? Were the interventions appropriate for the identified needs? How many people required temporary shelters? In addition disaster research is employed to investigate morbidity and mortality statistics (descriptive), incidence and prevalence of injuries, and exposure response for the determination of risk factors for illness, injury and death 28. The following are a sample of health data for quantitative analysis and hypothesis testing that are usually collected within the context of a mixed methods health disaster study: What were the injury types according to cause and mechanism (crush, drowning, burn, traumatic brain injury, malnutrition, etc.) Injury type according to anatomic region (head, neck, thorax, extremities) Circumstances of injury or death (building collapse, entrapment, flooding, fire, explosion, drought, etc.)
- 11. 11 Mechanism and pattern of dying (asphyxiation, exsanguination, hemorrhagic shock, ventricular fibrillation cardiac arrest, hypothermia, starvation, etc.) What was the severity of injuries (Injury severity scores)? Timing of death (instant, delayed, protracted) Location of injury or death (inside or outside of a building, out-of-hospital, during transport, in- hospital, etc.) Types and quantity of medical/surgical interventions employed (extrication, fluid resuscitation, basic or advanced trauma life support, resuscitative surgery, amputations, etc.), if possible by ICDM-10 codes. Types of disabilities? Epidemiological methods can be combined with evaluation methods to assess the influence of first aid training on relief efforts using inferential statistical analyses 9. Case-control methodology has been used since the 1970s to identify risk factors based on differences in circumstances between populations of injured and uninjured at the time of disaster impact 29-38. Prospective randomized clinical trials have not been reported in disaster situations due to the unpredictable nature of disasters. Table 4. Template for Concurrent Data Collection on DisasterCasualties ____________________________________________________________________________________ Name Age (if known) Date of birth (if known) Gender Numeric identifier/bar code Date of injury Date and time the victim was identified Location of the victim when injured Distance to treatment facility Mode of transportation to the treatment facility Distance to food sources
- 12. 12 Distance to potable water/water source Preliminary diagnosis or cause of injury/illness Type of treatment(s) provided at the scene of injury, during transport, and in-hospital Triage status of the victim on arrival to the treatment facility (EG. walking wounded, urgent, critical, dead on arrival) ________________________________________________________________________________________ Discussion We propose a consensus for the study of disaster response based on previous experiences in disaster studies and on a systematic analysis by public health experts and practitioners on the priorities for study and best methodology for disaster response research 3,4. There are many benefits that should accrue with the prioritization of the objectives and the systematic application of standardized research methods for the study of disaster 39. These guidelines provide purpose and structure and a detailed road map for the formulation of questions and hypotheses, identification of sources of data, and data collection templates in disaster situations. It also provides guidance on when and how to apply a mixed methodological approach. In addition, the structure and processes of the methods are generic enough to have applications in other domains within the broader disaster field. Its proper application by trained teams should result in increasing validity of the findings and enhanced reproducibility and generalizability applicable to all-hazards disaster research. The practical application of these consensus guidelines should result in evidence-based findings, and conclusions and recommendations to enhance the cost-effectiveness of the medical responses to disasters and their outcomes. Ongoing use of the processes outlined and the uniform reporting of data using standardized checklists and templates should facilitate the creation of data banks and registries to inform disaster planners as they review and revise existing disaster preparedness programs and interventions in anticipation of future disasters.
- 13. 13 Further development of the guidelines will include a consensus on a set of key indicators or best practices for each activity. Once the indicators have evolved, a set of measurements and potentially critical pathways should develop for each of the indicators. Ultimately, appropriate benchmarks will evolve and be tested using select indicators and methods for measurement. Once this is achieved, real quality monitoring capabilities will be in place. Numerous examples of tools for use in rapid needs assessment serve as models. There are several limitations to the methodology presented. A primary limitation of retrospective data collection is that much of the needed information is not documented or may be inconsistent. Also, information collected from individuals is subject to recall bias and is perishable. Perishable data change with the passage of time and consequently their value also decreases with the passage of time. In fact, much of the interview data obtained in or following disaster situations is subject to change by many confounding factors such as the influence of media reports, and the sharing of information between victims, between responders, and between others involved in the care delivered to the victims. Thus, for certain data, the time selected for data collection is crucial. Despite these limitations an attempt is made to reconstruct the events from data collected from individuals within the affected population namely, uninjured survivors, injured survivors and data on non-survivors. Another source of information is the group of individuals who were involved in the relief effort. These subgroups are primary sources of data collection. In conclusion, this consensus paper is meant to raise awareness among the general medical and humanitarian relief communities about an approach that will lead to an increased scope and systematic evidence-based study of disaster. We hope that the publication of this paper will lead to a debate within academic circles that will lead to a better understanding of the challenges of this particular area of research.
- 14. 14 References 1. http://www.fema.gov/national-response-framework 2. Yeskey K, Miller A. Science Unpreparedness. Disaster Medicine and Public health Preparedness. 2015 9(4): pp 444-445. 3. Creswell, J. W. (1999). Mixed-method research: Introduction and application. In G.Cizek (Ed.), Handbook of educational policy. San Diego, CA: Academic Press 4. Creswell, J. W., Goodchild, L., & Turner, P. (1996). Integrated qualitative and quantitative research: Epistemology, history, and designs. In J. Smart (Ed.), Higher education: Handbook of theory and research (Vol. 11, pp. 90–136). New York: Agathon Press. Understanding Mixed Methods Research 5. Klain M, Ricci E, Safar P, Semenov V, Pretto E, Tisherman S, Abrams J, Comfort L: Disaster Reanimatology Potentials: a structured interview study in Armenia I. Methodology and Preliminary results. Prehospital and Disaster Medicine. 1989; 4:135-152. 6. Ricci E, Pretto E, Safar P: Disaster Reanimatology Potentials: A structured interview study in Annenia II. Method for Evaluation of Medical Response to Major Disasters. Prehospital and Disaster Medicine 1991;6(2):159-166. 7. Pretto E, Ricci E, Safar P, et al: Disaster Reanimatology Potentials: A structured interview study in Armenia Ill. Final Results, Conclusions and Recommendations. Prehospital and Disaster Medicine 7(4):327-338, 1992. 8. Pretto E, Angus D, Abrams J, et al: An Analysis of Prehospital Mortality in an Earthquake. Prehospital and Disaster Medicine 9 (2):, 1994. 9. Angus D, Pretto E.A., Abrams J. Epidemiological assessment of mortality, building collapse pattern and medical response after the 1992 Earthquake in Turkey. Prehosp Disaster Medicine 1997; 12(3): 49-58. 10. Pretto E, Begovic M, Begovic M. Emergency Medical Services During the Siege of Sarajevo. Prehospital and Disaster Medicine 9(2):, 1994. 11. Angus D, Pretto EA, Abrams JI, Safar P: Recommendations for Life-Supporting First Aid Training of the Lay Public for Disaster Preparedness. Prehospital and Disaster Medicine 8(2):1993. 12. Abrams JI, Pretto E, Angus D, Safar P: Guidelines for Rescue Training of the Lay Public. Prehospital and Disaster Medicine, 8(2):1993.
- 15. 15 13. Kai T, Ukai E, Ohta M, Pretto E: Hospital Disaster Preparedness in Osaka, Japan. Prehospital and Disaster Medicine, 9(1):1994. 14. Pretto E, Angus D, Abrams JI, et al: An Analysis of Prehospital Mortality in an Earthquake. Pre Hosp and Disaster Med 9(2):1994. 15. Bissell R. Pretto E, Angus D, et al: Post-Preparedness Disaster Response in Costa Rica. Pre Hosp and Disaster Med 9(2):1994. 16. Ricci E, Pretto E: Assessment of Prehospital and Hospital Response in Disaster. Crit. Care Clinics, 7(2):471-484, 1991. 17. Comfort L, Tekin A., Pretto E, Kirimli B, Angus D. Time, Knowledge, and Action: The Effect of Trauma Upon Community Capacity For Action. Int. Journal of Mass Emergencies and Disasters 1998 16(1): 18. Pretto E, Safar P: National Medical Response to Mass Disasters in the United States. Are We Prepared? JAMA 266(9):1259-1266, 1990. 19. WHO. Indonesia earthquake tsunami 20. Perkins GD, Jacobs IG, Nadkarni VM. et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A Statement for Healthcare Professionals From a Task Force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. 2015 Nov;96:328-40. 21. Health disaster management: guidelines for evaluation and research in the Utstein Style. Volume I. Conceptual framework of disasters. Task Force on Quality Control of Disaster Management. Prehospital and Disaster Medicine 2003 17; suppl 3:1-177. 22. Health disaster management: guidelines for evaluation and research in the Utstein Style. Volume II. Structure framework, operational framework, and preparedness. Sundnes K.O. (guest editor). Task Force on Quality Control of Disaster Management. Scand J Public Health 2014; 42 (14 suppl): 1-195. 23. Silverman, M, Ricci, E, Gunter, M: Strategies for Improving the Rigorof Qualitative Methods in Evaluation of Health Care Programs. Evaluation Review, Vol 14, No 1, 1990, p 57-74 24. Suchman, E: Evaluative Research. Russell SageFoundation, New York, NY, 1967
- 16. 16 25. Gibson, G: Guidelines for Research and Evaluation of Emergency Medical Services. Health Services Reports, p 89-99, 1974. 26. Donabedian, A: The Definition of Quality and Approaches to Its Assessment. Health Administration Press, AnnArbor, MI, 1980 27. Eisenberg, M and Bergner, J: Paramedic Programs and Cardiac Mortality: Description of a Controlled Experiment. Public Health Reports, Vol 94(1), p 80-84, 1979 28. Noji, EK: Evaluation of the Efficacy of Disaster Response. UNDRO News, July/August, 1987, p 11-13 29. Domenici F., Levy J.I., Louis T.A. Methodological Challenges and Contributions in Disaster Epidemiology. Epidemiol Review 2005; 27:9-12. 30. DeVille de Goyet C, Del Cid E, Romero E, e t a1: Earthquake in Guatemala: Epidemiologic evaluation of the relief effort. Pan Am Hlth Org Bull., 95-109, 1976. 31. Glass RI, Um1tia JJ, Sibornys S, et al: Earthquake injuries related to housing in a Guatemalan village. Science 197:638643, 1977. 32. Lechat MF: Disasters and Public Health. Bull. WHO 57:11-17, 1979 33. Seaman J, Leivesley C, Hogg C (eds): Epidemiology of natural disasters. Basel: New York, Karger, 1984. 34. DeBruyker M, Greco D, Annino I, et al: The 1980 earthquake in southern Italy: Morbidity and Mortality. Int J Epidemiol 14:113-117, 1985. 35. Binder S, Sanderson LM: The role of the epidemiologist in natural disasters. Ann Emerg Med 16:1081-1084, 1987. 36. Deville de Goyet C, Zeballos JL: Communicable diseases and epidemiological surveillance after sudden natural disasters. In Baskett P, Weller R (eds): Medicine for Disasters. London, Wright, 1988, pp 252-269. 37. Gregg MB (ed): The Public Health Consequences of Disaster. Atlanta, Centers for Disease Control, 1989. 38. Pollander GS, Rund DA: Analysis of medical needs in disasters caused by earthquake: The need for a uniform reporting scheme. Disasters 13:365-369, 1989.
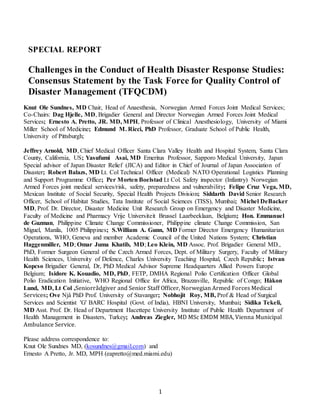
- 17. 17 Fig. 1. LIFE CYCLE OF A DISASTER FROM A HEALTH PERSPECTIVE Pre-event Health Status Event Damage 4. Disturbances in Health Status 5. Identification of Needs 6. Responses 7. Changes in Health Status NO 8. RestoredHealth Status? YES End
- 18. 18