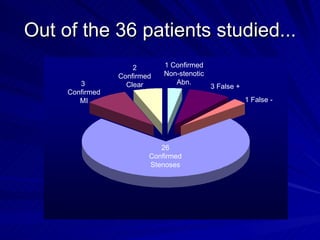
This study compared the results of 82Rb PET/CT myocardial perfusion imaging (MPI) to cardiac catheterization for 36 obese patients at St. Joseph's Hospital in Wisconsin. 32 of the 36 MPI scans matched the catheterization results, confirming the diagnostic quality of 82Rb PET/CT MPI. The higher gamma energy of 82Rb allows for higher quality images in obese patients compared to conventional MPI methods. 82Rb PET/CT MPI takes less time than other protocols, improving patient experience and clinic throughput.