The document discusses a rare case of simultaneous amoebic colonic perforation and ruptured liver abscess in a 70-year-old male presenting with severe abdominal pain and fever. Key features include the use of imaging techniques for diagnosis and surgical intervention, which involved right hemicolectomy and drainage of the liver abscess. The discussion highlights the prevalence and risks associated with invasive amoebiasis, surgical management options, and the importance of early detection to reduce mortality rates.








![DISCUSSION
Amoebic liver abscess is the most common manifestation
of extra intestinal amoebiasis. The causative agent is a
protozoan, Entameba histolytica.
10% of the world population harbours
E.histolytica in their colon, 10% of them may develop
invasive amoebiasis and 1-10% of these patients develop
amoebic liver abscess.
Amoebic liver abscess is common in tropical countries
and prevalent in low socioeconomic class living in
unhygienic conditions
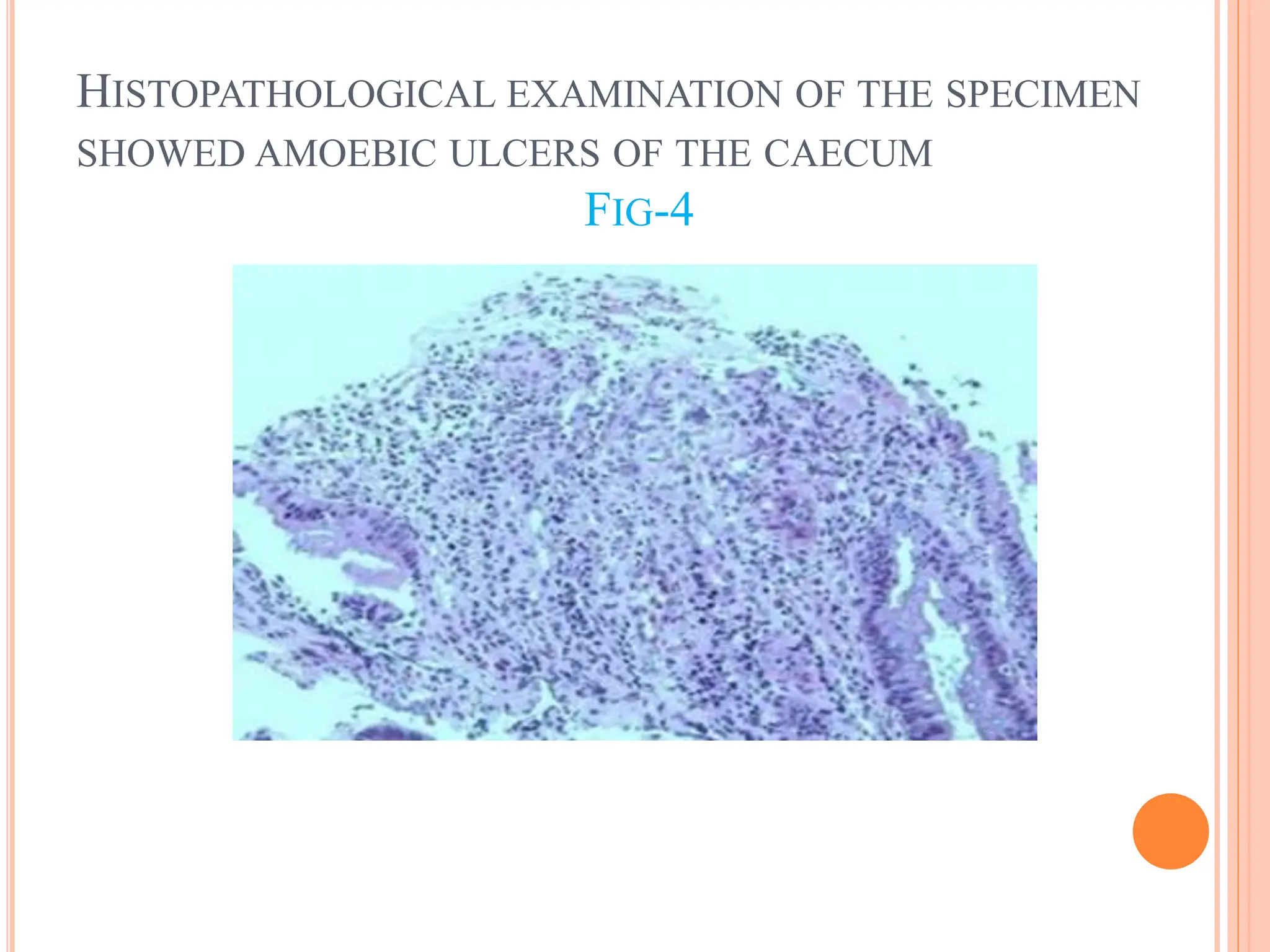
Trophozoites of Entameba histolytica usually invade
mucosa and submucosa of colon [4].](https://image.slidesharecdn.com/simultaneousamoebiccaecalperforationwithrupturedliverabscess-240507120637-e2d0cc5f/75/Simultaneous-Amoebic-Caecal-Perforation-with-Ruptured-Liver-Abscess-pptx-14-2048.jpg)
![ Invasion may reach up to musclar layer and serosa causing
silent perforation often involving caecum [1,2].
Bowel perforation occurs between 1%-6% of the patients
with amoebiasis [5].
The surgical approach is most efficient to treat a large liver
amoebic abscess(>5cm) and intraperitoneal collection and
colonic perforation [1,3,4].
Fecal peritonitis with concomitant ruptured liver abscess
usually leads to severe septicemia. If not detected at an early
stage ,mortality ranges from 6% to as high as 50% [4,5].](https://image.slidesharecdn.com/simultaneousamoebiccaecalperforationwithrupturedliverabscess-240507120637-e2d0cc5f/75/Simultaneous-Amoebic-Caecal-Perforation-with-Ruptured-Liver-Abscess-pptx-15-2048.jpg)