Download as PDF, PPTX


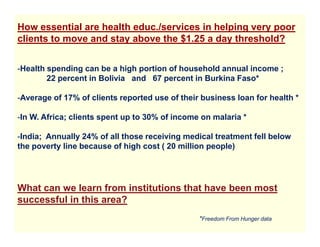

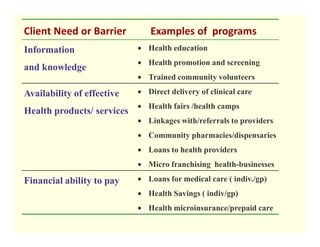

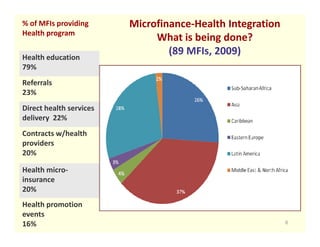

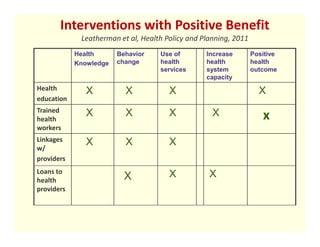
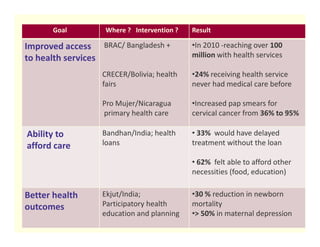

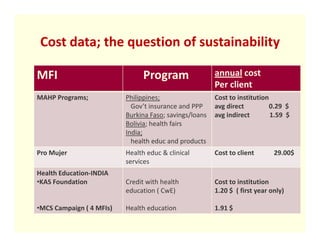
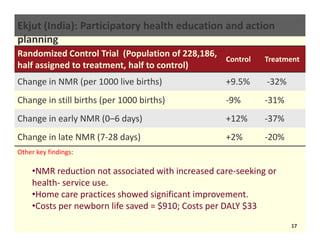

This document discusses integrating microfinance and health programs to improve access to healthcare for poor clients. It notes that illness is a major barrier to escaping poverty, and that microfinance institutions reach hundreds of millions globally. Integrating basic health education, services, and products can help address clients' health needs while leveraging the vast network of microfinance institutions. The evidence shows that combining health education with microfinance can positively impact reproductive health, child health, nutrition, disease prevention and more. Programs providing health education, loans for healthcare, or linking clients to providers have demonstrated improved access, behaviors, and health outcomes. Moving forward, barriers to integration like costs must be addressed to realize the potential of joining microfinance and health.











































































