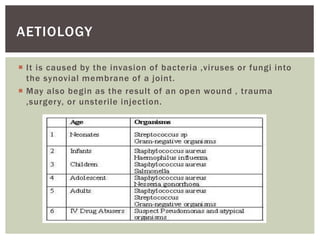
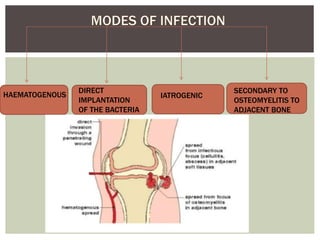
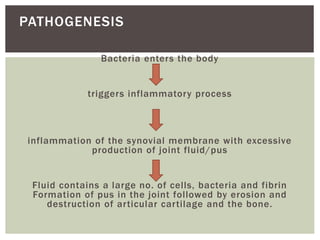
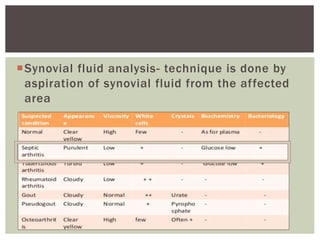
Septic arthritis is an infection-induced inflammation of the synovial membrane, primarily caused by bacteria such as Staphylococcus aureus, affecting patients of all ages and commonly impacting the hip and knee joints. Key clinical features include fever, joint swelling, pain, and restricted movement, with a diagnosis involving radiographic and laboratory tests to assess joint fluid and infection indicators. Treatment includes antibiotics, supportive care, possible surgical intervention, and physiotherapy to manage symptoms and restore joint function.