It isunpleasant state of tension, apprehension
or uneasiness a fear seem to arising from
unknown source.
Symptoms are tachycardia, sweating trembling
and palpitation.
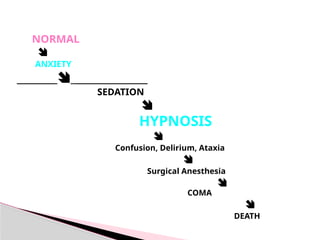
Since many anti anxiolytic drugs cause sedation
so same drug is clinically used as both
anxiolytic and hypnotic (sleep inducing ) drug.
Anxiety
An effectivesedative (anxiolytic) agent should
reduce anxiety and exert a calming effect.
The degree of central nervous system
depression caused by a sedative should be the
minimum consistent with therapeutic efficacy.
Sedative-Hypnotics
5.
A hypnoticdrug should produce drowsiness
and encourage the onset and maintenance of a
state of sleep.
Hypnotic effects involve more pronounced
depression of the central nervous system than
sedation, and this can be achieved with most
drugs in this class simply by increasing the
dose.
Sedative-Hypnotics
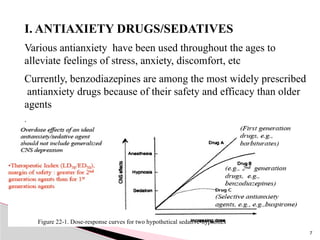
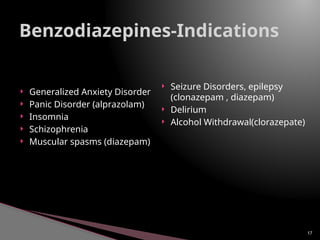
I. ANTIAXIETY DRUGS/SEDATIVES
Variousantianxiety have been used throughout the ages to
alleviate feelings of stress, anxiety, discomfort, etc
Currently, benzodiazepines are among the most widely prescribed
antianxiety drugs because of their safety and efficacy than older
agents
.
Figure 22-1. Dose-response curves for two hypothetical sedative-hypnotics
7
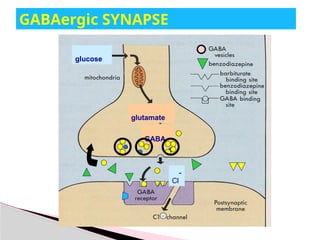
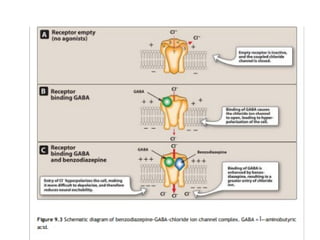
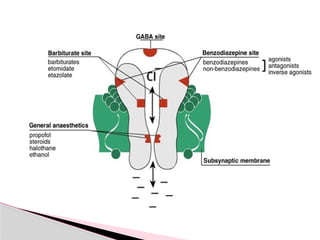
GABA isthe major inhibitory neurotransmitter
in the CNS.
The target of BZD is GABA receptor.
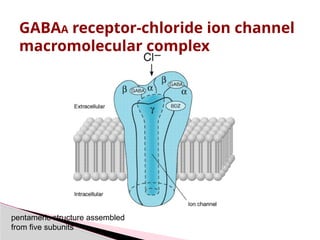
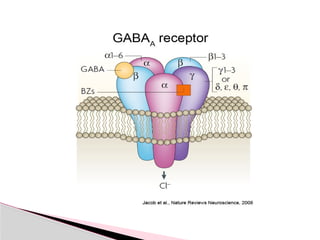
These receptors are composed of ἀ,ᵝ and ᵞ
subunit families.
BZD binds to the “benzodiazepine receptors”
on GABA neuron located at the interface of
alpha and gemma 2 subunit.
Benzodiazepines relieve anxiety through
enhancement of the inhibitory activity of GABA
No antipsychotic, No analgesic, Not affect ANS
10
Benzodiazepines
Mechanism of Action
Binding ofBZD results in the increase
frequency of the chloride channel opening
produced by GABA.
The influx of chloride ions cause a
hyperpolarization resulting in inhibition of the
formation of the action potential.
MOA
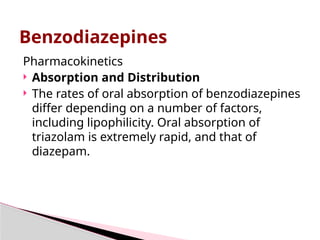
Pharmacokinetics
Absorption andDistribution
The rates of oral absorption of benzodiazepines
differ depending on a number of factors,
including lipophilicity. Oral absorption of
triazolam is extremely rapid, and that of
diazepam.
Benzodiazepines
19.
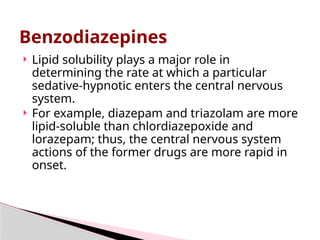
Lipid solubilityplays a major role in
determining the rate at which a particular
sedative-hypnotic enters the central nervous
system.
For example, diazepam and triazolam are more
lipid-soluble than chlordiazepoxide and
lorazepam; thus, the central nervous system
actions of the former drugs are more rapid in
onset.
Benzodiazepines
20.
Biotransformation
Metabolic transformationto more water-
soluble metabolites is necessary for clearance
of sedative-hypnotics from the body. The
microsomal drug-metabolizing enzyme
systems of the liver are most important
Benzodiazepines
21.
Excretion
The water-solublemetabolites of
benzodiazepines and other sedative-hypnotics
are excreted mainly via the kidney.
The Benzodiazepines & Barbiturates
23.
Drowsiness andconfusion: These effects are
the two most common side effects of the
benzodiazepines.
Ataxia occurs at high doses and precludes
activities that require fine motor coordination,
such as driving an automobile.
Cognitive impairment (decreased long-term
recall and retention of new knowledge) can
occur with use of benzodiazepines.
Adverse effects of benzodiazepines
24.
Triazolam, oneof the most potent oral
benzodiazepines with the most rapid
elimination, often shows a rapid development
of tolerance, early morning insomnia, and
daytime anxiety, along with amnesia and
confusion.
Adverse effects of benzodiazepines
25.
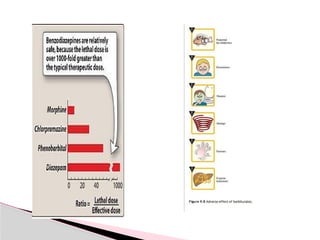
Alcohol andother CNS depressants enhance
the sedative-hypnotic effects of the
benzodiazepines. Benzodiazepines are,
however, considerably less dangerous
than the older anxiolytic and hypnotic drugs.
As a result, a drug overdose is seldom lethal
unless other central depressants, such as
alcohol, are taken concurrently.
Precautions
26.
a selectivecompetitive antagonist of BZD
receptors (Bz1).
Blocks action of benzodiazepines and
reverse the its effects
Rapid but short acting
Half life 1hr
IV available
FLUMAZENIL
27.
Long acting(1-2days)
Phenobarbital
Shortacting (3-8hrs)
Pentobarbital
Secobarbital
Amobarbital
Ultra short acting(20min)
thiopental
2. Barbiturates
28.
Barbiturates
are secondchoice as sedative – hypnotic.
Mechanism of Action:
Facilitation of GABA action on the brain.
increase the duration of the GABA gated
channel opening but in large dose, they can
directly activating chloride channels. (not
through BZD receptors).
30.
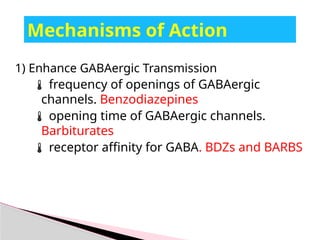
Mechanisms of Action
1)Enhance GABAergic Transmission
frequency of openings of GABAergic
channels. Benzodiazepines
opening time of GABAergic channels.
Barbiturates
receptor affinity for GABA. BDZs and BARBS
31.
Barbiturates -Actions
Barbituratesare less selective in their actions than
benzodiazepines
1. Cns depression: since they also depress the actions of
excitatory neurotransmitters (eg, glutamic acid) in
parallel with their effects on GABA neurotransmission.
2. This multiplicity of sites of action of barbiturates may
be the basis for their ability to induce full surgical
anesthesia and for their more pronounced central
depressant effects (which result in their low margin of
safety) compared to benzodiazepines.
3. Respiratory depression
4. Its also induce the CYP p450microsomal enzyme of
the liver.
Advantages of BZDover barbiturates
1. Selective: minimal respiratory and
cardiovascular depression.
2. High therapeutic index.
3. Less dependence with minimal withdrawal
symptoms
4. Has specific antagonist
35.
Some antihistamine have sedative properties
Diphenhydramine
Hydoxyline
Doxylamine
Effective in treating mild form of insomia
But not for all types
Further more they have numerous undesired
effects(anticholinergic)
3.Antihistamine
Zolpidem
imidazopyridine derivative.
acts on benzodiazepine receptors &
facilitate GABA mediated neuronal inhibition.
Induce hypnotic effect for 5 hrs
rapidly absorbed from GIT and metabolized
to inactive metabolites via liver CYT P450.
Short duration of action ( 2- 4 h).
39.
Zolpidem
has nomuscle relaxant effect.
has no anticonvulsant effect.
Minimal tolerance & dependence.
Minimal rebound insomnia.
Its efficacy is similar to benzodiazepines.
40.
Zolpidem
Minor effecton sleep pattern
Respiratory depression occur at high doses in
combination with other CNS depressant as
ethanol.
Uses
a hypnotic drug for short term treatment of
insomnia
Zaleplon
Binds toBZs receptors and facilitate GABA
action, cause hypnosis.
Rapid absorption
Short onset of action (30min)
Short duration of action (3 hr)
Metabolized by liver microsomal enzymes
metabolism is inhibited by cimetidine
44.
Zaleplon
Little effecton sleep pattern
Potentiates action of other CNS depressants
(alcohol).
Used as hypnotic drug
The ultrashort half-life gives zaleplon a unique
advantage over other hypnotics because of its
lack of next-day residual effects on driving and
other performance-related skills
45.
Anxiolytic
Usedin GAD
Moa action different from BDZ
Bind to the serotonin and dopamine receptors.
Lack anticonvulsant property .
Lack muscle relaxant property
Dependence is unlikey
ADRS
Low frequency of ADR
Increase prolactin and growth hormone.
Cause hypopthermia
Nervousness
Light headedness
Buspirone-sedative
46.
Cns depressant
Ethanol potentiates GABA-receptor actions via
a mechanism independent of benzodiazepine-
receptor
Sedation ultimately hypnosis
Readily absorbed
Large vol. of distribution
Metabolised in liver
Excreted by kidney
Ethanol – sedative
48.
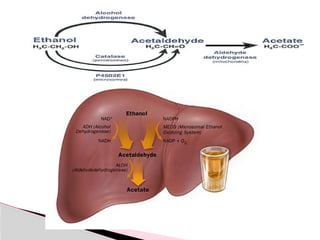
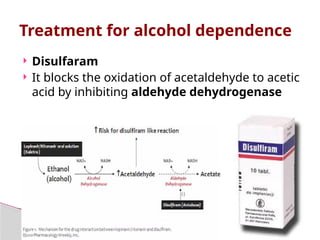
Disulfaram
Itblocks the oxidation of acetaldehyde to acetic
acid by inhibiting aldehyde dehydrogenase
Treatment for alcohol dependence
49.
This resultsin the accumulation of the
acetaldehyde resulting in
Tachycardia
Flushing
Hyperventilation
Nausea
These response induce patient to avoid alco.hol
#6 Delirium :A state of uncontrolled excitement or emotion:
Ataxia: Loss of the ability to coordinate muscular movement
Ataxia is a lack of muscle coordination which may affect speech, eye movements, the ability to swallow, walking, picking up objects and other voluntary movements. A person with persistent ataxia may have damage in the part of the brain that controls muscle coordination - the cerebellum.
Dyskinesia refers to a category of movement disorders that are characterized by involuntary muscle movements, including movements similar to tics or chorea and diminished voluntary movements.
Tardive dyskinesia: A neurological syndrome characterized by repetitive, involuntary, purposeless movements caused by the long-term use of certain drugs ...
akinesiaabsence or loss of the power of voluntary movement. 2. the temporary paralysis of a muscle by the injection of procaine. akinesia al´gera a condition characterized by generalized pain associated with movement of any kind
Dystonia:a state of abnormal muscle tone resulting in muscular spasm and abnormal posture, typically due to neurological disease or a side effect of drug therapy.
#16 Anterograde amnesia is a loss of the ability to create new memories after the event that caused the amnesia, leading to a partial or complete inability to recall the recent past, while long-term memories from before the event remain intact.
#23 Ataxia:Loss of the ability to coordinate muscular movement.
Precludes: prevent
#46 Alcohol is a multiple-action depressor of the Central Nervous System, and the depression caused by it is dose-dependent. Although alcohol is mainly used because of its stimulating action, this action is only apparent and happens only with moderate doses. It results from the depression of inhibitory controlling mechanisms. Under the effect of alcohol the cortex is freed from its integrative role, thus resulting confuse and disorganized thinking, as well as disruption of adequate motor control.
Ethanol diffuses through lipids, modifying proteins fluidity and functions. High concentrations of ethanol can decrease the eletron-transporting functions of the Na+K+/ATPase pump, thus impairing electrical conduction in the nerve cells.
Neuropharmacology of Alcohol
Only recently was it possible to understand the neurobiological mechanisms responsible for many clinical manifestations of alcoholism. Ethanol affects different cerebral neurotransmitters. One of them is the inhibitory neurotransmitter gamma-aminobutyric acid (GABA).
The interaction between ethanol and the GABA receptor is evident in studies showing decrease in the symptoms of alcoholic-withdrawal syndrome by the use of substances that increase GABA activity, like GABA-reuptake blockers and benzodiazepines, thus demonstrating the possible influence of the GABAergic system on the physiopathology of human alcoholism.
Ethanol potentiates GABA-receptor actions via a mechanism independent of benzodiazepine-receptor.
See the animation
GABAergic pathways play an important inhibitory action on the other neuronal pathways. GABA-receptor is associated with the chloride channel and the benzodiazepine receptor, making up a functional complex. When GABA binds to its receptor, it promotes an increase in the opening frequency of chloride channels, thus allowing a greater flow of this ion to the intracellular medium, making it more negative, and thus promoting neuronal hyperpolarization.
Low alcohol concentrations could promote facilitation of GABAergic inhibition on the cerebral cortex and spinal cord.
Some phenomena observed in alcoholism, such as tolerance and dependence, could be explained by the effects consequent to chronic ethanol exposure.
The quick tolerance to the increased chloride influx mediated by GABA begins already in the first hours and becomes established during chronic alcohol use.
Alcohol selectively modifies the cerebral synaptic action of glutamate. The glutamatergic system, whose neurons use glutamate as neurotransmitter, and is one of the main excitatory pathways in the central nervous system, also seems to play a relevant role in the nervous alterations induced by ethanol. Glutamate is the major neuroexcitatory neurotransmitter in the brain, accounting for 40% of all synapses.
Post-synaptic actions of glutamate in the central nervous system are mediated through two types of receptor: One of them is the inotropic receptor, related to ionic channels causing neuronal depolarization. The second type of receptor is the metabotropic (since its answers need cellular signalization metabolic steps); its intracellular actions are mediated by G-protein.
One of the inotropic glutamate receptors has two families diferentially identified by their pharmacological, biophysical, and molecular characteristics. In the first family we find the NMDA (n-metil-D-aspartate receptor), voltage-dependent, that sustains the currents, and is associated with ion channels permeable to calcium, sodium and potassium. In the second family of glutamate receptors we find the AMPA/Ka, whose preferental agonist is a-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid.
Glutamate participates in synaptic plasticity and in long term potentiation (LTP), and it seems to play a critical role in memory and cognition.
The prevailing eletrophysiological effect of ethanol is the reduction of excitatory glutamatergic neurotransmission. It has been observed that low concentrations of ethanol can inhibit the stimulating actions mediated by NMDA upon hippocampal cells in culture.
In concentrations associated to "in vivo" intoxication, ethanol inhibits NMDA receptor current.
These findings could also explaim part of the genesis of physical dependence to alcohol, through a process that is the opposite to that of GABA. That means that when ethanol is interrupted, glutamatergic pathways induce overexcitement of the central nervous system, causing convulsions, anxiety, and delirium.
Calcium influx into the cells has an important function in the release of neurotransmitters in the synaptic cleft, as well as in the activity of cellular second messengers. Ethanol, in concentrations of 25mM, seems to inhibit calcium flow through ionic channels, thus decreasing neurotransmitters release. This could also be one of the mechanisms responsible for dependence and tolerance, because when alcohol-intake is stopped these ionic channels would increase calcium influx and, consequently, neurotransmission, giving rise to signs and symptoms of withdrawal syndrome.