Worldwide prevalence
approximately16.4 million adults are affected by
RVO:
13.9 million by BRVO
and 2.5 million by CRVO
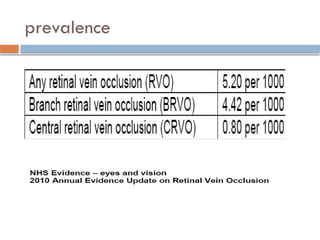
Rogers S, McIntosh RL, Cheung N, et al; International Disease Consortium. The prevalence of retinal vein occlusion: pooled data
from population studies in the United States, Europe, Asia, and Australia. Ophthalmology 2010; 117(2):313-319 e1
5.
Natural course
50-60%patients: recovery of visual acuity to
20/40, or better, without therapy.
91% within 1st
year
Pre-treatment VA
Depends on site and degree of occlusion
collateral circulation
Poor prognosis
Chronic macular edema (14% VA>6/12)
Vit h’ge due to neovascularization
6.
Management of BRVO
GENERAL PRINCIPALS
Maximise Recovery and Vision
Prevent re-occlusion
Detect any associated systemic disease
Detect / Prevent Glaucoma
Protect other eye
Exclusion / control of
Diabetes
HTN
hyperlipidaemia
hyperviscosity/coagulation states
antiphospholipid syndrome
7.
Blood investigations
Thrombophilicconditions, such as the following, may also be
involved:
Homocysteine levels
Protein S deficiency
Protein C deficiency
Resistance to activated protein C (factor V Leiden)
Antithrombin III deficiency
Antiphospholipid antibody
BVOS (1984)
Purpose
Todetermine
whether scatter argon laser photocoagulation can prevent
the development of neovascularization.
whether peripheral scatter argon laser photocoagulation
can prevent vitreous hemorrhage.
whether macular argon laser photocoagulation can
improve visual acuity in eyes with macular oedema
reducing vision to 20/40 or worse.
TREATMENT GROUPS:Photocoagulation vs.
Observation
RESULTS:
IMPACT: Established macular laser photocoagulation as the
clinical standard therapy for macular edema due to BRVO
13.
Recommendations (BVOS)
Observationfor 3months to allow for resolution of macular edema
and haemorrhages
If VA ≤ 20/40 and persistent macular edema FFA to
determine the extent of ischemia
In the absence of macular ischemia , laser grid photocoagulation to
the area of leakage
14.
Treatment of Neovasularizationin BVOS
If peripheral scatter laser photocoagulation is applied in eyes with
large areas of nonperfusion, the incidence of neovascularization can be
reduced from about 40% to 20%.
In prophylactic treatment , many eyes (60%) that would never develop
neovascularization would receive peripheral scatter laser.
Only CNP, follow up at 4 monthly intervals (no laser)
In confirmed neovascularization by FFA, PROMPT peripheral scatter
laser can reduce the likelihood of vitreous hemorrhage from 60% to
30%.
15.
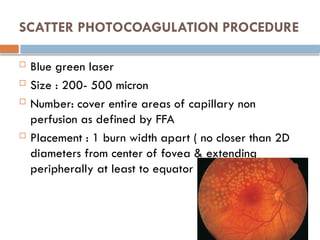
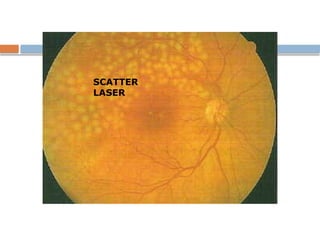
SCATTER PHOTOCOAGULATION PROCEDURE
Blue green laser
Size : 200- 500 micron
Number: cover entire areas of capillary non
perfusion as defined by FFA
Placement : 1 burn width apart ( no closer than 2D
diameters from center of fovea & extending
peripherally at least to equator
GRID PHOTOCOAGULATION PROCEDURE
Size: 50 to 100 μm
Exposure: 0.05 to 0.1 seconds
Intensity: mild
Number: areas of diffuse retinal thickening and focal
leaks (if any)
Placement: 1 to 2 burn-widths apart (500-3000 μm from
center of fovea)
Wavelength: green to yellow
18.
Mechanism of GridLaser in macular edema
activates RPE pump to reduce edema.
produces thinning of outer retina & reduces oxygen
consumption and increases choroidal delivery of
oxygen to the inner retina, producing a consequent
autoregulatory constriction of the retinal vasculature in
the leaking area & decreasing the edema.
19.
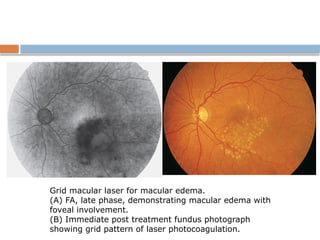
Grid macular laserfor macular edema.
(A) FA, late phase, demonstrating macular edema with
foveal involvement.
(B) Immediate post treatment fundus photograph
showing grid pattern of laser photocoagulation.
20.
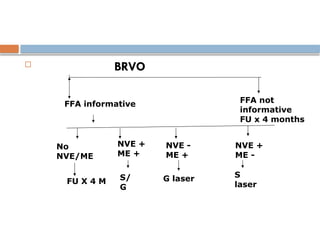
BRVO
FFA informativeFFA not
informative
FU x 4 months
No
NVE/ME
NVE +
ME +
NVE -
ME +
NVE +
ME -
FU X 4 M S/
G
G laser S
laser
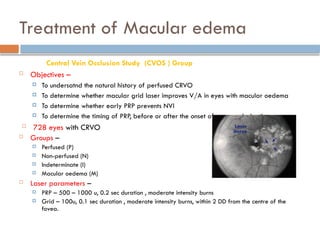
Treatment of Macularedema
Central Vein Occlusion Study (CVOS ) Group
Objectives –
To undersatnd the natural history of perfused CRVO
To determine whether macular grid laser improves V/A in eyes with macular oedema
To determine whether early PRP prevents NVI
To determine the timing of PRP, before or after the onset of neovascularization.
728 eyes with CRVO
Groups –
Perfused (P)
Non-perfused (N)
Indeterminate (I)
Macular oedema (M)
Laser parameters –
PRP – 500 – 1000 u, 0.2 sec duration , moderate intensity burns
Grid – 100u, 0.1 sec duration , moderate intensity burns, within 2 DD from the centre of the
fovea.
23.
Conclusions –
1/3rd
of perfused CRVO convert to non-perfused within 3 yrs
Grid laser is not recommended for macular oedema, its use in patients
> 65yrs is yet to be determined
Majority of (I) are non-perfused
Prophylactic PRP is not recommended
Prompt PRP at the first sign of NVI diminishes the development of NVG
No effective treatment for ischaemic CRVO.
PRP –
Treatment of choice in ischaemic CRVO to prevent and cause regression of
neovascularization
CRVO Treatment Study
24.
Follow - up
Perfused –
Every 2-3 months for 6 months, then yrly for 3 yrs
Non-perfused –
Every month for first 6 months, then yrly
Macular oedema -
Every month for first 6 months, then yrly
25.
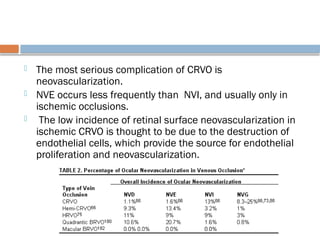
Treatment of Neovascularization
The most serious complication of CRVO is
neovascularization.
NVE occurs less frequently than NVI, and usually only in
ischemic occlusions.
The low incidence of retinal surface neovascularization in
ischemic CRVO is thought to be due to the destruction of
endothelial cells, which provide the source for endothelial
proliferation and neovascularization.
26.
RECOMMENDATIONS OF CVOS
PRP be delivered promptly after the development
of NVI/NVA but not prophylactically in eyes with
nonperfused CRVO .
Persons presenting with NVD/NVE without NVI/NVA
should be treated with PRP,
The Standard Careversus COrticosteroid
for REtinal Vein Occlusion Study
(The SCORE Study)
31.
OBJECTIVE:
To compare theefficacy and safety of 1-mg and
4-mg doses of preservative-free intravitreal
triamcinolone (IVTA) with standard care (grid
photocoagulation) for eyes with vision loss
associated with macular edema secondary to
BRVO.
preservative-free, sterile, single use, nondispersive formulation of triamcinolone
was used, brand name TRIVARIS; Allergan, Inc, Irvine, California ) in 1-mg and
4-mg doses. administered in a volume of 0.05 mL.
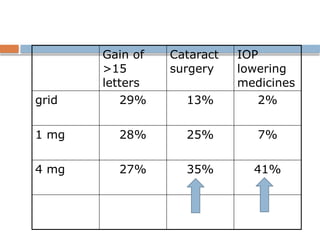
SCORE BRVO Conclusion
Consensus : Grid laser (standard care) : the
treatment for macular edema secondary to BRVO
Similar efficacy in all 3 groups up to month 12
Improved efficacy for laser beyond month 12
Superior safety profile of laser over 1-mg and 4-
mg Triamcinolone
34.
SCORE CRVO
Tocompare the Efficacy and Safety of Intravitreal
Triamcinolone With Observation to Treat Vision
Loss Associated With Macular Edema Secondary to
Central Retinal Vein Occlusion
35.
Objective
To comparethe efficacy and safety of 1-mg and 4-
mg doses of preservative-free intravitreal
triamcinolone with observation for eyes with vision
loss associated with macular edema secondary to
perfused central retinal vein occlusion (CRVO).
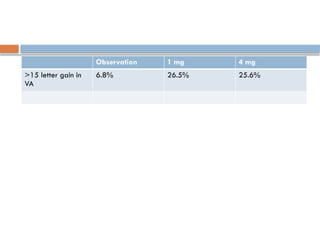
Comments
Natural historyof untreated CRVO is poor, with
only 7% showing a gain in visual acuity of >15
letters as compared to IVTA group (26%).
Although OCT showed decrease in all the groups,
maximum visual acuity gain was found in IVTA
group.
This could be due to anti- VEGF , antiinflammatory
and possible neuroprotective effect of coriticosteroids .
38.
Both 1mg and 4 mg groups had comparable results
in terms of visual efficacy
The adverse event profile is dose dependent
39.
SCORE CRVO Conclusion
Intravitreal triamcinolone effective in improving
visual acuity
1 mg triamcinolone preferred for better safety
profile
OZURDEX™
(dexamethasone intravitreal implant)
•Injectable, biodegradable intravitreal implant contains 0.7 mg (700
μg) dexamethasone in the NOVADUR™
solid polymer drug
delivery system (preservative-free).
• Poly (D,L-lactide-co-glycolide) PLGA biodegradable polymer matrix, which slowly
degrades to lactic acid and glycolic acid as dexamethasone is gradually released.
42.
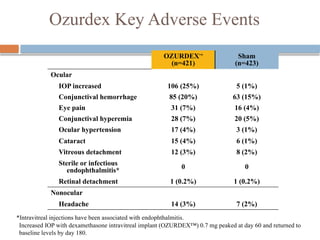
Ozurdex Key AdverseEvents
*Intravitreal injections have been associated with endophthalmitis.
OZURDEX™
(n=421)
Sham
(n=423)
Ocular
IOP increased 106 (25%) 5 (1%)
Conjunctival hemorrhage 85 (20%) 63 (15%)
Eye pain 31 (7%) 16 (4%)
Conjunctival hyperemia 28 (7%) 20 (5%)
Ocular hypertension 17 (4%) 3 (1%)
Cataract 15 (4%) 6 (1%)
Vitreous detachment 12 (3%) 8 (2%)
Sterile or infectious
endophthalmitis* 0 0
Retinal detachment 1 (0.2%) 1 (0.2%)
Nonocular
Headache 14 (3%) 7 (2%)
Increased IOP with dexamethasone intravitreal implant (OZURDEX™) 0.7 mg peaked at day 60 and returned to
baseline levels by day 180.
43.
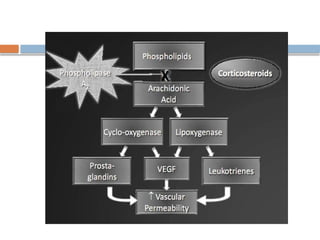
Anti-VEGFs
Vitrectomy
Chorioretinal anastomosis
Arteriovenous sheathotomy
Newer Treatments
Anti-VEGFs are most widely used
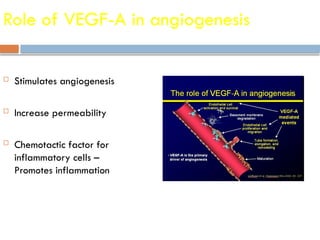
Role of VEGF-Ain angiogenesis
Stimulates angiogenesis
Increase permeability
Chemotactic factor for
inflammatory cells –
Promotes inflammation
46.
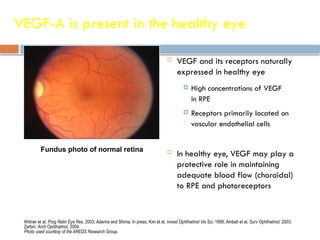
VEGF-A is presentin the healthy eye
VEGF and its receptors naturally
expressed in healthy eye
High concentrations of VEGF
in RPE
Receptors primarily located on
vascular endothelial cells
In healthy eye, VEGF may play a
protective role in maintaining
adequate blood flow (choroidal)
to RPE and photoreceptors
Witmer et al, Prog Retin Eye Res, 2003; Adamis and Shima, In press; Kim et al, Invest Ophthalmol Vis Sci, 1999; Ambati et al, Surv Ophthalmol, 2003;
Zarbin, Arch Ophthalmol, 2004.
Photo used courtesy of the AREDS Research Group.
Fundus photo of normal retina
47.
Pathologic
VEGF-A secreted byRPE
• Hypoxia
• Accumulation of lipid metabolic
byproducts
• Oxidative stress to retina & RPE
• Alterations in Bruch’s membrane
• Drusen (Reduction in the
choriocapillaries blood flow and block
diffusion of oxygen and nutrients to RPE
and photoreceptors)
Initiating stimuli for VEGF release
Witmer et al, Prog Retin Eye Res, 2003; Ferrara et al, Nat Med, 2003. 47
50.
RanibizumaB for theTreatment of Macular
Edema following BRAnch Retinal Vein
Occlusion (BRAVO) Study
51.
BRAVO Study
Six-monthphase 3 study with 6 months of follow-up
20/40 to 20/400 (mean 20/ 80)
CST 250 microns (mean 488 µ sham,
552 µ ranibizumab)
Foveal center ME within 12 months
Perfused BRVO
Campochiaro PA et al. Ophthalmology. 2010;117:1102-1112.
52.
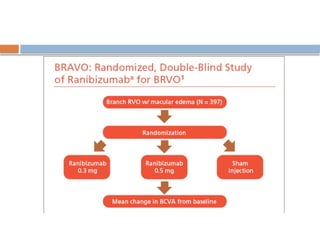
A Study ofthe Efficacy and Safety of Ranibizumab Injection in Patients
With Macular Edema Secondary to Branch Retinal Vein Occlusion
(BRAVO)
397 pt.
3 groups
o 0.3mg ranibizumab
o 0.5mg ranibizumab
o Sham
Monthly injections for 6
months
eligible for laser rescue T/t at 3
mths if
- Macular edema showed little
or no improvement
- VA 20/40 or worse
- CFT ≥ 250 µm
12 months study ; 6 months
data published in June 2010
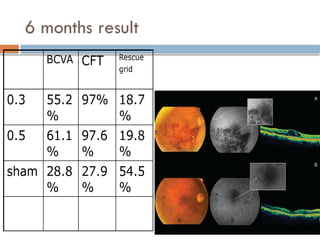
Conclusions
Monthly injectionsof Ranibijumab are effective in
improving VA & reducing macular edema.
Low rates of adverse events
This study prompted FDA approval of ranibizumab
for the treatment of CRVO .
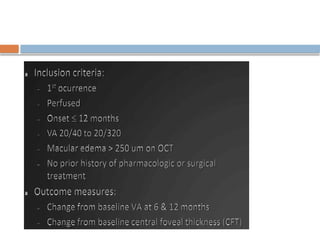
Key inclusion criteria
1. Macular edema secondary to CRVO with CRT ≥
250 μm
2. ETDRS BCVA of 20/40 to 20/320 in the study
eye
67.
Key exclusion criteria
1. Previous use of intraocular or periocular
corticosteroids in the study eye
2. Previous treatment with anti-angiogenic drugs in
the study eye
3. Prior panretinal laser photocoagulation or
macular laser photocoagulation in the study eye
4. CRVO disease duration > 9 months
68.
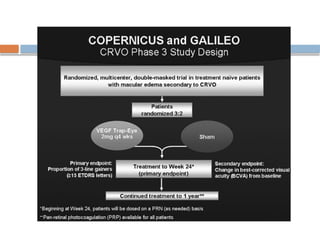
Treatment groups and
randomization
Patients were randomized 3:2 to 2-mg VEGF Trap-
Eye or sham injections every 4 weeks upto week 24.
Week 24 to Week 52, patients received either 2-
mg VEGF Trap-Eye as needed (p.r.n.) or sham
injections based on re-treatment criteria.
69.
Outcomes
Primary endpoint:The proportion of patients who
gained ≥ 15 ETDRS letters from baseline at Week
24
Key secondary endpoint: The change in BCVA from
baseline to Week 24
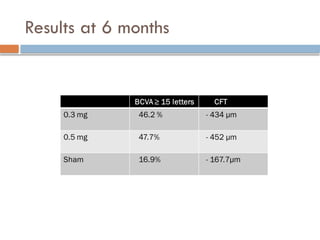
Efficacy
Statistically significantdifferences between patients
receiving VEGF Trap-Eye compared with sham were
seen at Week 24 in both studies
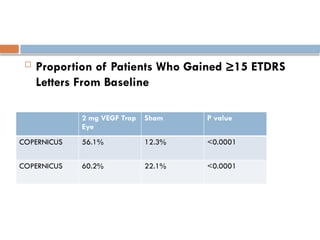
73.
Proportion ofPatients Who Gained ≥15 ETDRS
Letters From Baseline
2 mg VEGF Trap
Eye
Sham P value
COPERNICUS 56.1% 12.3% <0.0001
COPERNICUS 60.2% 22.1% <0.0001
74.
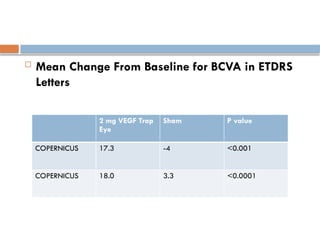
Mean ChangeFrom Baseline for BCVA in ETDRS
Letters
2 mg VEGF Trap
Eye
Sham P value
COPERNICUS 17.3 -4 <0.001
COPERNICUS 18.0 3.3 <0.0001
75.
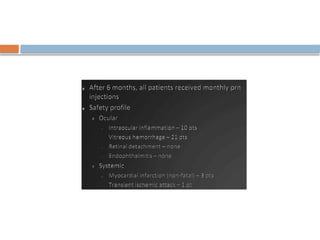
Safety
2-mg VEGFTrap-Eye treatment was generally well
tolerated
COPERNICUS: The most frequently reported
treatment-emergent adverse events (TEAEs) were
conjunctival hemorrhage, visual acuity reduced, and
eye pain
GALILEO: eye pain, conjunctival hemorrhage, and
elevated IOP
76.
BRVO Summary
BRVO:
SCORE: Laser better than IVTA
OZURDEX: Dexamethasone better than sham (no laser
arm)
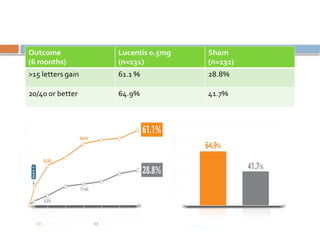
BRAVO: Ranibizumab monthly for 6 months better than
observation in BRAVO. Improved VA: 61% vs 29% eyes
gained 15 or more letters
77.
BRVO Summary
BRVO:
SCORE: Laser better than IVTA
OZURDEX: Dexamethasone better than sham (no laser
arm)
BRAVO: Ranibizumab monthly for 6 months better than
observation in BRAVO. Improved VA: 61% vs 29% eyes
gained 15 or more letters
VEGF TRAP appears beneficial in initial studies
78.
CRVO Summary
CRVOtreatment options
Steroids beneficial in phase 3 studies
SCORE Study: IVTA vs observation
OZURDEX Trials: dexamethasone vs sham
Anti-VEGFs
CRUISE: Ranibizumab monthly for 6 months better than
observation. Improved VA: 48% vs 17% eyes gained 15 or
more letters
VEGF TRAP appears beneficial in initial studies
utilizes monthlyintravitreal Ranibizumab injections
for 9 months to see if total VEGF blockade will
prevent neovascular glaucoma and eliminate the
need for panretinal photocoagulation in patients
with ischemic central retinal vein occlusion.
81.
When to starttreatment ????
no timely treatment photoreceptor
damage/cell death/ permanent cystoid changes
irreversible VA loss
82.
Role of peripheralischemia
Using Wide-field FFA
Eyes with more edema, often have more peripheral
ischemia
Anti – VEGFs decrease both
83.
RELATE STUDY
RanibizumabDosE Comparison and the Role of
LAser in the managemenT of REtinal Vein
Occlusions (RELATE)
Ongoing study
If higher doses of anti-VEGF more effective
If Laser treatment of peripheral ischemia could
decrease the no. of injections
84.
Role of LASERin RVO begins to
evolve
Ultra wide field FFA view of periphery
If ischemia do PRP
PRP decreases VEGF production / inflammation
Decreased ME
85.
If targetingPRP to only peripheral ischemic areas
can stop the cycle of ischemia while preserving
more peripheral vision ???
86.
Limitations
Various studiesare incomparable
Unmatched in design
Wide disparity in the sham groups
Apart from ME, other facets like ocular
neovascularisation , scantily studied
87.
No robustevidence as to how the concurrent
systemic abnormalities , affect the course and
consequences of RVO, with or without intervention.
88.
VEGFs areonly small link in cascade involved in
pathogenesis of RVO
Maintaining a normal balance b/w anti angiogenic
and proangiogenic factors would be more suitable
approach rather than targeting only proangiogenic
VEGFs