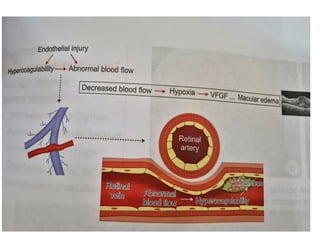
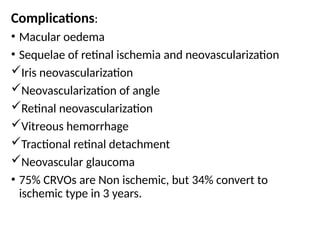
Retinal venous occlusive disease, including branch retinal vein occlusion (BRVO) and central retinal vein occlusion (CRVO), is a common vascular condition caused by thrombosis in the retinal venous system, leading to vision loss and complications such as macular edema. Risk factors include age, hypertension, diabetes, and various systemic conditions, and diagnosis involves a comprehensive ocular examination alongside systemic evaluations. Management options primarily focus on treating underlying conditions and using medications like anti-VEGF agents for macular edema, with varying prognoses based on the occlusion type and associated complications.