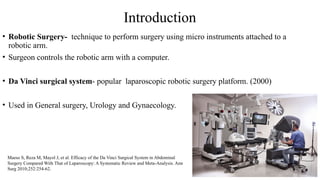
Introduction
• Robotic Surgery-technique to perform surgery using micro instruments attached to a
robotic arm.
• Surgeon controls the robotic arm with a computer.
• Da Vinci surgical system- popular laparoscopic robotic surgery platform. (2000)
• Used in General surgery, Urology and Gynaecology.
Maeso S, Reza M, Mayol J, et al. Efficacy of the Da Vinci Surgical System in Abdominal
Surgery Compared With That of Laparoscopy: A Systematic Review and Meta-Analysis. Ann
Surg 2010;252:254-62.
3.
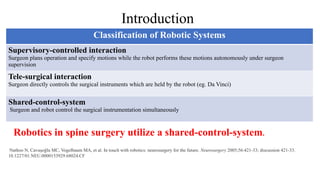
Robotics in spinesurgery utilize a shared-control-system.
Nathoo N, Cavuşoğlu MC, Vogelbaum MA, et al. In touch with robotics: neurosurgery for the future. Neurosurgery 2005;56:421-33; discussion 421-33.
10.1227/01.NEU.0000153929.68024.CF
Classification of Robotic Systems
Supervisory-controlled interaction
Surgeon plans operation and specify motions while the robot performs these motions autonomously under surgeon
supervision
Tele-surgical interaction
Surgeon directly controls the surgical instruments which are held by the robot (eg. Da Vinci)
Shared-control-system
Surgeon and robot control the surgical instrumentation simultaneously
Introduction
4.
Principle
Shared Control system:
•Surgeon and robot control the surgical instrumentation
simultaneously toward a shared surgical goal
• User maintains some degree of direct or indirect control
over an automated system.
augment the surgeon’s tactile processes while refining
intraoperative judgment.
Navigation and Robotics in Spine Surgery. Alexander Vaccaro; Jaykar Panchmatia; David Kaye; Srinivas Prasad.
5.
Spine Robots
First spinerobot - the Spine Assist/Renaissance (Mazor) – 2004 FDA approved
Spine robotic systems:
• Mazor Robotics (Medtronic)
• ROSA One (Zimmer Biomet)
• Excelsius GPS (Globus Medica).
Mazor Robot
Galetta MS, Leider JD, Divi SN, Goyal DKC, Schroeder GD. Robotics in spinal surgery. Ann Transl Med. 2019
Sep;7(Suppl 5):S165. doi: 10.21037/atm.2019.07.93. PMID: 31624731; PMCID: PMC6778279.
6.
Applications
Pedicle screw placement- prime area of robotic spine surgery at present.
Spinal fusion and Instrumentation procedures.
Future Directions:
• Spinal tumor resection.
• Revision surgery.
• Vertebroplasties.
• Deformity correction.
7.
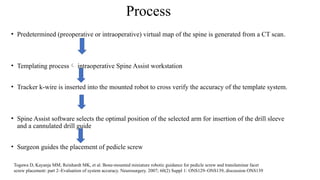
Process
• Predetermined (preoperativeor intraoperative) virtual map of the spine is generated from a CT scan.
• Templating process intraoperative Spine Assist workstation
• Tracker k-wire is inserted into the mounted robot to cross verify the accuracy of the template system.
• Spine Assist software selects the optimal position of the selected arm for insertion of the drill sleeve
and a cannulated drill guide
• Surgeon guides the placement of pedicle screw
Togawa D, Kayanja MM, Reinhardt MK, et al. Bone-mounted miniature robotic guidance for pedicle screw and translaminar facet
screw placement: part 2–Evaluation of system accuracy. Neurosurgery. 2007; 60(2) Suppl 1: ONS129–ONS139, discussion ONS139
Outcomes In RoboticSurgery
• In a meta-analysis performed by Verma et al. data from 23 studies were included and evaluated the
placement of 5,992 pedicle screws in Robotic Assisted (RA) and Free Hand (FH) surgery.
Significant increase in the accuracy rate of RA surgery
• Shin et al. performed a meta-analysis, evaluating over 7,000 placed pedicle screws and reported an incidence
of Misplaced screws of 15% in the FH group and 6% in the RA group
• In a study conducted by Schatlo et al., 95 patients with degenerative lumbar disease underwent either RA or
FH screw placement. Clinically acceptable screw accuracy was 91.4% in the RA group compared to
87.2% in the FA group
Verma R, Krishan S, Haendlmayer K, Mohsen A. Functional outcome of computer-assisted spinal pedicle screw placement: a systematic review and meta-analysis of 23
studies including 5,992 pedicle screws. Eur Spine J. 2010 Mar;19(3):370-5. doi: 10.1007/s00586-009-1258-4. Epub 2010 Jan 6. PMID: 20052504; PMCID: PMC2899753.
Shin BJ, James AR, Njoku IU, et al. Pedicle screw navigation: a systematic review and meta-analysis of perforation risk for computer-navigated versus freehand
insertion. J Neurosurg Spine 2012;17:113-22. 10.3171/2012.5.SPINE11399
Schatlo B, Molliqaj G, Cuvinciuc V, et al. Safety and accuracy of robot-assisted versus fluoroscopy-guided pedicle screw insertion for degenerative diseases of the lumbar
spine: a matched cohort comparison. J Neurosurg Spine. 2014;20:636-43. 10.3171/2014.3.SPINE13714
10.
Advantages of RoboticSurgery
• Minimal incision.
• Less soft tissue dissection.
• Increased accuracy.
• Reduction in radiation exposure.
• Reduced complication rates Misplaced screws and neurological deficits
Navigation and Robotics in Spine Surgery. Alexander Vaccaro; Jaykar Panchmatia; David Kaye; Srinivas Prasad.
11.
Limitations of RoboticSurgery
• Cost
• Learning curve
• Increased surgical time
• Possible intraoperative discrepancy between preoperative CT imaging and
intraoperative registration. poor image quality, excessive amounts of soft tissue in the patient
hindering proper robotic arm positioning and surgeon error during registration.
Beutler WJ, Peppelman WC, DiMarco LA. The da Vinci robotic surgical assisted anterior lumbar interbody fusion: technical development and case
report. Spine 2013;38:356-63.
12.
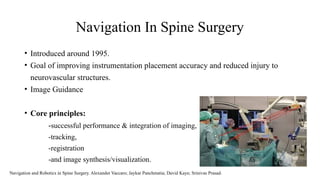
Navigation In SpineSurgery
• Introduced around 1995.
• Goal of improving instrumentation placement accuracy and reduced injury to
neurovascular structures.
• Image Guidance
• Core principles:
-successful performance & integration of imaging,
-tracking,
-registration
-and image synthesis/visualization.
Navigation and Robotics in Spine Surgery. Alexander Vaccaro; Jaykar Panchmatia; David Kaye; Srinivas Prasad.
13.
Navigation In SpineSurgery
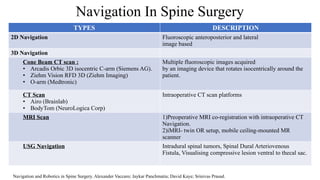
TYPES DESCRIPTION
2D Navigation Fluoroscopic anteroposterior and lateral
image based
3D Navigation
Cone Beam CT scan :
• Arcadis Orbic 3D isocentric C-arm (Siemens AG).
• Ziehm Vision RFD 3D (Ziehm Imaging)
• O-arm (Medtronic)
Multiple fluoroscopic images acquired
by an imaging device that rotates isocentrically around the
patient.
CT Scan
• Airo (Brainlab)
• BodyTom (NeuroLogica Corp)
Intraoperative CT scan platforms
MRI Scan 1)Preoperative MRI co-registration with intraoperative CT
Navigation.
2)iMRI- twin OR setup, mobile ceiling-mounted MR
scanner
USG Navigation Intradural spinal tumors, Spinal Dural Arteriovenous
Fistula, Visualising compressive lesion ventral to thecal sac.
Navigation and Robotics in Spine Surgery. Alexander Vaccaro; Jaykar Panchmatia; David Kaye; Srinivas Prasad.
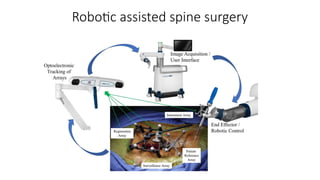
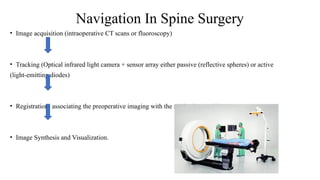
• Image acquisition(intraoperative CT scans or fluoroscopy)
• Tracking (Optical infrared light camera + sensor array either passive (reflective spheres) or active
(light-emitting diodes)
• Registration- associating the preoperative imaging with the navigation tracking system.
• Image Synthesis and Visualization.
Navigation In Spine Surgery
• Advantages:
High accuracyof pedicle screw placement in complex spinal anatomy.
Decreased radiation exposure
Reduced revision rates.
• Limitation:
Longer operating time
Learning Curve
Cost
Navigation In Spine Surgery
18.
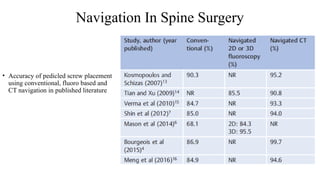
Navigation In SpineSurgery
• Accuracy of pedicled screw placement
using conventional, fluoro based and
CT navigation in published literature
19.
Summary
• Robotic assistanceand Navigation in spine surgery should be used as
an adjunct in optimizing surgical outcome.
• Possess the advantage of increased accuracy and less radiation
exposure.
• Drawback of high acquisition cost and steep learning curve.






















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

