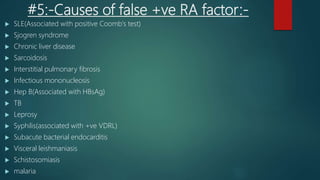
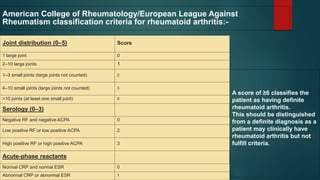
The document provides an overview of various rheumatological diseases, including their common causes and clinical features, such as rheumatoid arthritis, osteoarthritis, gout, and systemic lupus erythematosus. It presents symptomatology, differential diagnoses for polyarthritis, and explains the causes of false positives for rheumatoid factor tests. Additionally, it touches on classification criteria for rheumatoid arthritis based on joint distribution and serology.




















![[Int. med] approach to joint pain from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/064ftjyatacrqjgurlzo-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171713-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

