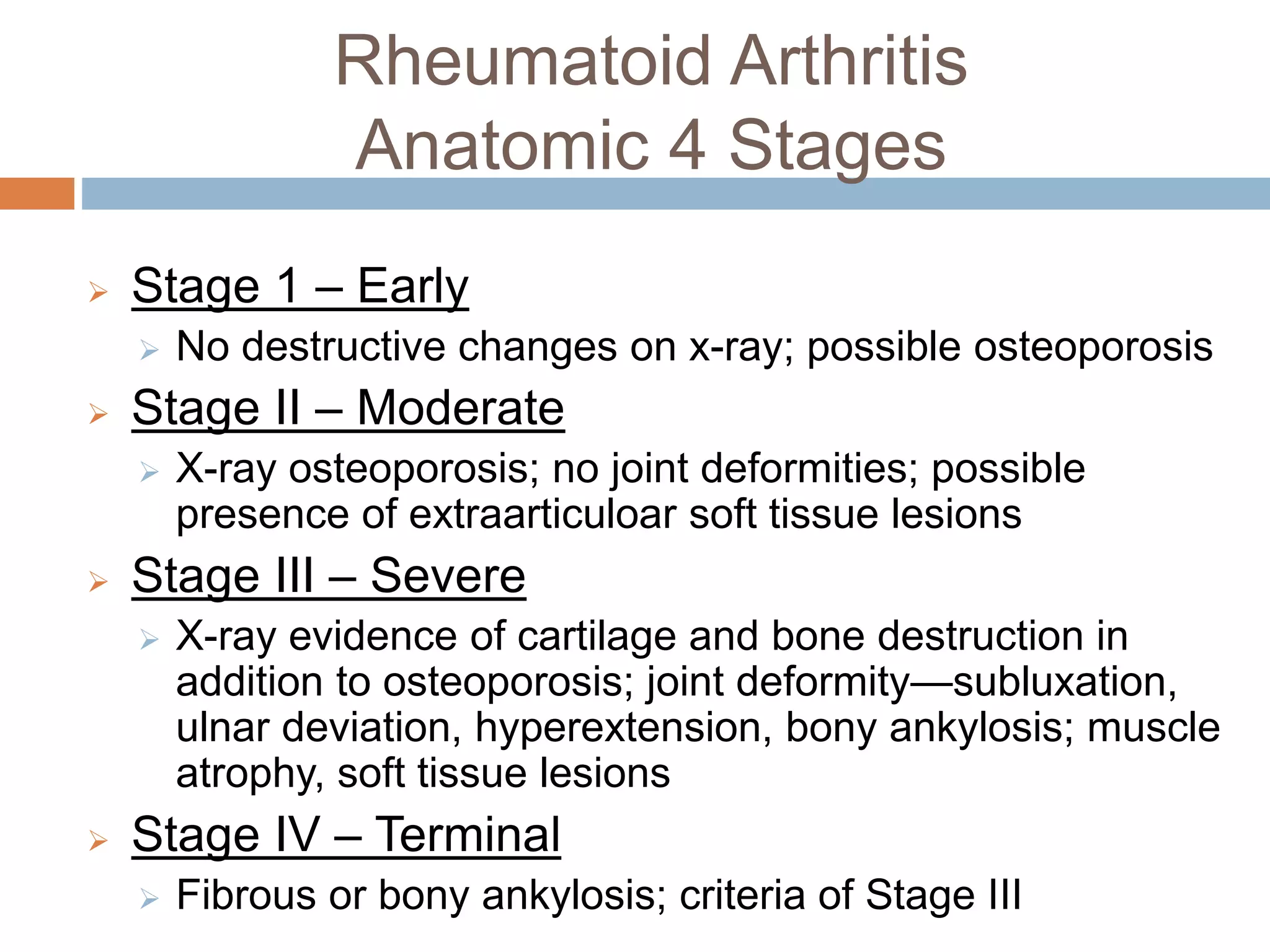
Rheumatoid arthritis is a chronic autoimmune disease that causes inflammation of the synovial joints, resulting in pain, stiffness, and swelling. It affects around 1% of the population worldwide. The cause is unknown but is believed to involve genetic and environmental factors. Diagnosis is based on symptoms, blood tests for rheumatoid factor and CRP levels, and x-ray evidence of joint damage. Treatment aims to reduce inflammation and prevent further joint destruction, using medications like NSAIDs, DMARDs, corticosteroids, and biologics. Surgery may be required in advanced cases to repair damaged joints.