1. The document proposes a revised electronic medical record data model consisting of assessment objects, management objects, and encounters as the central class.
2. Encounters would contain assessment and management objects and stack together to form episodes of care and disease courses.
3. The model simplifies previous structures and provides a common format for sharing data between different software languages, while allowing flexibility for individual software providers.
Using NLP and curation to make clinical data available for researchWarren Kibbe
While at Northwestern we developed a chart abstraction tool using a data mart to present EHR data to research personnel without double entry. Used in the Brain Tumor Institute. Mike Gurley did the majority of the development.
Odoo OpenERP 7 Medical Healthcare and Hospital Management Systempragmatic123
We provide implementation service for Medical which is an open source, centralized Health and Hospital Information System that provides the following functionality :
1) Electronic Medical Record (EMR)
2) Hospital Information System (HIS)
3) Health Information System
EMR (Electronic Medical Record) is computerized legal medical record created in an organization that delivers care such as Hospital or doctor’s clinic. EMR will provide to improve the quality of life by reducing costs. The use of the system will help to centralize the medical information.
Pragmatic has launched another new and advanced Product in the field of Health-care Management . This Product comes with many features like
1) Patient Management with full patient details like General Information , Socio-Economic Details , Diet and exercise details etc
2) Appointment Management with Features like Confirmation of Appointment , Related Prescriptions , Pediatric Symptom Checklist.
3) Inpatient Management with features like Diet Details , Nutrition and care plan etc.
4) ICU with details like GCS , ECG , APACHE 2 score etc.
5) Roundings with options like Six P's , Vital signs , Respiratory Details etc
6) Patient Ambulatory Care informations.
7) Patient Laboratory test Management.
8) Newborn records with details like Neonatal signs and symptoms ,Neonatal Reflex check.
9) Pharmacy with related entries in Warehouse.
10) Pre - configured data according to ICD-10 Standard for Diseases , Medical procedures , Recreational drugs , Medical Specialties , Disease Categories etc.
11) Various Reports like appointments per doctor , appointments per month , Appointments per specialty.
ABOUT HORIZON HI-TECH SOFT SYSTEMS
Horizon Hi-Tech Soft Systems is a leading-edge Web Application Development and Digital Marketing Company committed to provide a wide array of reliable, innovative and cost-effective digital services to clients across the globe. As a diverse digital services company, Horizon Hi-Tech Soft Systems offers an entire gamut of services under one roof - ranging from CMS website development, custom web application development Search Engine Optimization and other digital marketing services
Complete and accurate clinical documentation in the medical record has a direct impact on the assignment of codes, more accurate levels of reimbursement, and is critical to the higher quality of patient care. This paper describes the development of a system which can automatically flag the cases if there is an opportunity of improvement in patient clinical doc- uments. Automated Clinical Documentation Improvement (CDI) leverages the natural language processing (NLP) and contextual understanding of health record structure with additional business rules logic, helping CDI specialists identify critical documentation information that may be missing from the medical record. This results in more specific coding opportunity and better under- standing of the clinical complexity for accurate reimbursement. This system helped increase CDI specialists’ productivity by efficiently filtering cases which need more attention from them.
Hospital Management System provides the benefits of enhanced administration & control, superior patient care, strict cost control and improved profitability. HMS is powerful, flexible, and easy to use and is designed and developed to deliver real conceivable benefits to hospitals. More importantly it is backed by reliable and dependable support.
SoftClinic software is designed keeping in mind the needs of physicians. It is currently being used by over 600+ doctors/physicians every day in more than 15 countries.
Awarded one of the Best Hospital Management Software by various Physicians & Surgeons Association, SoftClinic can be used not only by physicians but also by small Hospitals & Nursing homes.
SoftClinic software (with 9 modules) is the only hospital management software available in the market at the cost of a Clinic Management software.
Learn about the AORN Syntegrity® Framework, standardized clinical content providing a consistent method for documenting perioperative patient care that has been validated by expert perioperative nurses. This framework aligns documentation with nursing workflow enabling reliable and valid data to be captured. Documentation represents the perioperative nursing plan of care via the most up-to-date version of the PNDS language (3rd version) and complements a perioperative information system or Electronic Health Record.
A presentation in March 2012 presented at the Ramathibodi Hospital Administration School, Faculty of Medicine Ramathibodi Hospital, Mahidol University in Bangkok, Thailand. Presentation partly in English and partly in Thai.
Using NLP and curation to make clinical data available for researchWarren Kibbe
While at Northwestern we developed a chart abstraction tool using a data mart to present EHR data to research personnel without double entry. Used in the Brain Tumor Institute. Mike Gurley did the majority of the development.
Odoo OpenERP 7 Medical Healthcare and Hospital Management Systempragmatic123
We provide implementation service for Medical which is an open source, centralized Health and Hospital Information System that provides the following functionality :
1) Electronic Medical Record (EMR)
2) Hospital Information System (HIS)
3) Health Information System
EMR (Electronic Medical Record) is computerized legal medical record created in an organization that delivers care such as Hospital or doctor’s clinic. EMR will provide to improve the quality of life by reducing costs. The use of the system will help to centralize the medical information.
Pragmatic has launched another new and advanced Product in the field of Health-care Management . This Product comes with many features like
1) Patient Management with full patient details like General Information , Socio-Economic Details , Diet and exercise details etc
2) Appointment Management with Features like Confirmation of Appointment , Related Prescriptions , Pediatric Symptom Checklist.
3) Inpatient Management with features like Diet Details , Nutrition and care plan etc.
4) ICU with details like GCS , ECG , APACHE 2 score etc.
5) Roundings with options like Six P's , Vital signs , Respiratory Details etc
6) Patient Ambulatory Care informations.
7) Patient Laboratory test Management.
8) Newborn records with details like Neonatal signs and symptoms ,Neonatal Reflex check.
9) Pharmacy with related entries in Warehouse.
10) Pre - configured data according to ICD-10 Standard for Diseases , Medical procedures , Recreational drugs , Medical Specialties , Disease Categories etc.
11) Various Reports like appointments per doctor , appointments per month , Appointments per specialty.
ABOUT HORIZON HI-TECH SOFT SYSTEMS
Horizon Hi-Tech Soft Systems is a leading-edge Web Application Development and Digital Marketing Company committed to provide a wide array of reliable, innovative and cost-effective digital services to clients across the globe. As a diverse digital services company, Horizon Hi-Tech Soft Systems offers an entire gamut of services under one roof - ranging from CMS website development, custom web application development Search Engine Optimization and other digital marketing services
Complete and accurate clinical documentation in the medical record has a direct impact on the assignment of codes, more accurate levels of reimbursement, and is critical to the higher quality of patient care. This paper describes the development of a system which can automatically flag the cases if there is an opportunity of improvement in patient clinical doc- uments. Automated Clinical Documentation Improvement (CDI) leverages the natural language processing (NLP) and contextual understanding of health record structure with additional business rules logic, helping CDI specialists identify critical documentation information that may be missing from the medical record. This results in more specific coding opportunity and better under- standing of the clinical complexity for accurate reimbursement. This system helped increase CDI specialists’ productivity by efficiently filtering cases which need more attention from them.
Hospital Management System provides the benefits of enhanced administration & control, superior patient care, strict cost control and improved profitability. HMS is powerful, flexible, and easy to use and is designed and developed to deliver real conceivable benefits to hospitals. More importantly it is backed by reliable and dependable support.
SoftClinic software is designed keeping in mind the needs of physicians. It is currently being used by over 600+ doctors/physicians every day in more than 15 countries.
Awarded one of the Best Hospital Management Software by various Physicians & Surgeons Association, SoftClinic can be used not only by physicians but also by small Hospitals & Nursing homes.
SoftClinic software (with 9 modules) is the only hospital management software available in the market at the cost of a Clinic Management software.
Learn about the AORN Syntegrity® Framework, standardized clinical content providing a consistent method for documenting perioperative patient care that has been validated by expert perioperative nurses. This framework aligns documentation with nursing workflow enabling reliable and valid data to be captured. Documentation represents the perioperative nursing plan of care via the most up-to-date version of the PNDS language (3rd version) and complements a perioperative information system or Electronic Health Record.
A presentation in March 2012 presented at the Ramathibodi Hospital Administration School, Faculty of Medicine Ramathibodi Hospital, Mahidol University in Bangkok, Thailand. Presentation partly in English and partly in Thai.
Mining Health Examination Records A Graph Based Approachijtsrd
EHR Electronic Health Records collects data on yearly basis and it is used in many countries for healthcare.HER Health Examination Records collects the data on regular basis and identifies the participants at risk that is important for early warning and prevention.the fundamental challenge is for learning classification model for risk prediction with unlabelled data and live data string that established the majority of the collected dataset.the unlabelled data string describes the participants in health examintions whose health conditions can be vary from healthy to highly risky or very ill.in this paper, we propose a graph based,semisupervised learning algorithm called SHG health semi supervised heterogenous graph on Health for risk prediction and assessment to classify a progressively developing condition with the majority of the data unlabelled. An efficient iterative algorithm is designed and developed to proof the convergence is given.extensive experiments based on both real health examination dataset and live datasets to show effectiveness of our method. Jayashri A. Sonawane | Dr. Swati A. Bhavsar ""Mining Health Examination Records - A Graph Based Approach"" Published in International Journal of Trend in Scientific Research and Development (ijtsrd), ISSN: 2456-6470, Volume-3 | Issue-3 , April 2019, URL: https://www.ijtsrd.com/papers/ijtsrd22810.pdf
Paper URL: https://www.ijtsrd.com/engineering/computer-engineering/22810/mining-health-examination-records---a-graph-based-approach/jayashri-a-sonawane
Faro An Interactive Interface For Remote Administration Of Clinical Tests Bas...Kalle
A challenging goal today is the use of computer networking and advanced
monitoring technologies to extend human intellectual capabilities in medical decision making. Modern commercial eye trackers
are used in many of research fields, but the improvement of eye tracking technology, in terms of precision on the eye movements capture, has led to consider the eye tracker as a tool for vision analysis, so that its application in medical research, e.g. in ophthalmology, cognitive psychology and in neuroscience has grown considerably. The improvements of the human eye tracker interface become more and more important to allow medical doctors to increase their diagnosis capacity, especially if the interface allows them to remotely administer the clinical tests more appropriate for the problem at hand. In this paper, we propose a client/server eye tracking system that provides an interactive system for monitoring patients eye movements depending on the clinical test administered by the medical doctors. The system supports the retrieval of the gaze information and provides statistics to both medical research and disease diagnosis.
Cis evaluation final_presentation, nur 3563 sol1SBU
An overview of a Computer Information System (CIS) and considerations that need to be taken with implementing an Electronic Health Record (EHR) in a healthcare setting.
Health institution requires quality data and information management to function effectively and efficiently. It is an understatement to say that many organizations, institutions or government agencies have become critically dependent on the use of database system for their successes especially in the hospital. This work aims at developing an improved hospital information management system using a function-based approach. An efficient HIMS that can be used to manage patient information and its administration is presented in this work. This is with the goal of eradicating the problem of improper data keeping, inaccurate reports, wastage of time in storing, processing and retrieving information faced by the existing hospital information system in order to improve the overall efficiency of the health institution. The system was developed with Hypertext Markup Language (HTML), Cascading Style Sheets (CSS), Hypertext Preprocessor (PHP), and My Structured Query Language (MySQL). The new system was tested using data collected from Renewal Clinic, Ibadan, Nigeria was used as case study were the data for the research was collected and the system was tested. The system provides a vital platform of information storage and retrieval in hospitals.
A comprehensive study on disease risk predictions in machine learning IJECEIAES
Over recent years, multiple disease risk prediction models have been developed. These models use various patient characteristics to estimate the probability of outcomes over a certain period of time and hold the potential to improve decision making and individualize care. Discovering hidden patterns and interactions from medical databases with growing evaluation of the disease prediction model has become crucial. It needs many trials in traditional clinical findings that could complicate disease prediction. A Comprehensive study on different strategies used to predict disease is conferred in this paper. Applying these techniques to healthcare data, has improvement of risk prediction models to find out the patients who would get benefit from disease management programs to reduce hospital readmission and healthcare cost, but the results of these endeavors have been shifted.
The large volumes of data and biosignals produced by the ICU overwhelm doctors and nurses, and do little to help them set priorities for the activities required in these units.
Similar to Revised electronic medical record data model (20)
1. REVISED ELECTRONIC MEDICAL RECORD DATA MODEL
By M W MAIR, Ophthalmic Surgeon, Timaru, New Zealand
This is a response to The Electronic Medical Record Data Model posted by
the NZHIF.
The model for discussion is found at:
http://fims-www.massey.ac.nz/~jpastor/emr/emr_model/sld001.htm
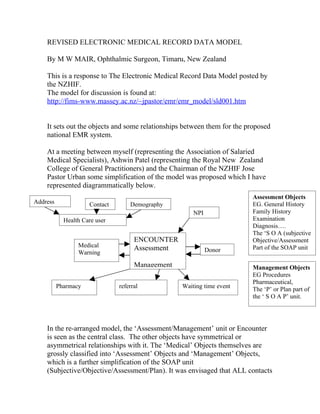
It sets out the objects and some relationships between them for the proposed
national EMR system.
At a meeting between myself (representing the Association of Salaried
Medical Specialists), Ashwin Patel (representing the Royal New Zealand
College of General Practitioners) and the Chairman of the NZHIF Jose
Pastor Urban some simplification of the model was proposed which I have
represented diagrammatically below.
Assessment Objects
Address Contact Demography EG. General History
NPI Family History
Health Care user Examination
Diagnosis….
The ‘S O A (subjective
ENCOUNTER Objective/Assessment
Medical Assessment Part of the SOAP unit
Warning Donor
Management Management Objects
EG Procedures
Pharmaceutical,
Pharmacy referral Waiting time event The ‘P’ or Plan part of
the ‘ S O A P’ unit.
In the re-arranged model, the ‘Assessment/Management’ unit or Encounter
is seen as the central class. The other objects have symmetrical or
asymmetrical relationships with it. The ‘Medical’ Objects themselves are
grossly classified into ‘Assessment’ Objects and ‘Management’ Objects,
which is a further simplification of the SOAP unit
(Subjective/Objective/Assessment/Plan). It was envisaged that ALL contacts
2. between Healthcare Providers and clients could be modeled in this way
including In Patient contacts.
A stack of such encounters with a particular provider or organization would
constitute an ‘Episode of Care’.
A stack of such encounters which was coterminous with the Natural History
of a disease process would constitute a ‘Disease Course’. A ‘Disease
Course’ and an ‘Episode of Care’ would often be coterminous.
Diagram of Two Episodes of Care, One Disease Course
Episode of Care
Episode of Care
Assessment
Objects Disease Course
Management
Objects
A three dimensional diagram of the progression of ‘Encounters’ into
‘Episodes of care’ and ‘Disease Courses’ is shown above. This picture
does not show all the Administrative Objects (such as demographic
details, NPI etc.) which are ‘hung off’ each encounter, for simplicity.
It shows within the ‘Assessment’ and ‘Management’ sections of each
‘Encounter’ an undifferentiated “heap” of medical object instances.
These are the raw data, collected at each encounter. They are
structured into screens and protocols by the end users software, and
the ‘Standard’ does not dictate how those structures should be.
3. Summary
We have been able to agree on a simple structure for the New Zealand
Medical Record Data Model which is diagrammed above.
1.The Objects in the Term Dictionary form a currency for transactions, and
serve more than one purpose. They contain (as Object Instances) the
data collected during ‘Encounters’; they can be used for
epidemiological research; they can be used for accounting and audit.
2.The Standard would specify a common format for objects, which can be
shared between different languages eg C++, Smalltalk, Fox 5, etc, and
suggests that the medical objects are segregated into ‘Assessment’
objects and ‘Management’ objects. This means that there will be a
dated cluster of object instances corresponding to each encounter.
3.The Standard itself should not further structure the data, this being left to
the Software Providers, which will continue to compete both within
and between market niches.
4. Just three levels of client engagement with the Health Sector are
envisaged: The ‘Encounter’, the ‘Episode of Care’, the ‘Disease
Course.’
Agreement about this data model would then permit further agreement on
conventions governing encryption, transmission, security etc. which
must be in place before a National System comes into use. An agreed
minimal structure as outline above is a prerequisite for such a viable
National system.
M. W. Mair
POB 319 Timaru
eyetech@es.co.nz
Monday, December 22, 1997