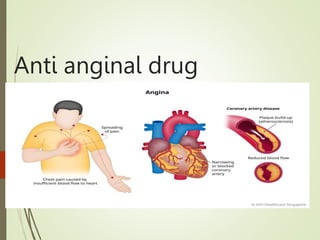
2. Angina
Angina Pectoris is a symptom of myocardial ischemia and occurs due to an imbalance
between the myocardium’s oxygen demand and oxygen supply.
3. • Characteristic abrupt, severe, pressing-like substernal chest pain radiating
towards neck, jaw, back, and arms. Patients may also experience dyspnea or
atypical symptoms such as indigestion, nausea, vomiting, or diaphoresis.
• Usually precipitated by exercise, excitement, or a heavy meal.
• Transient episodes (15 seconds to 15 minutes) of myocardial ischemia (stable
angina) do not result in cellular death; as occurs in myocardial infarction (MI).
4. TYPES OF ANGINA
Typical Angina (Classical Angina)
Pain is commonly induced by exercise, excitement,
or a heavy meal.
Secondary to advanced atherosclerosis of
coronary vessels.
Associated with ST-segment depression on ECG.
Usually lasts 1-15 minutes.
The ST Segment represents the
interval between ventricular
depolarization and repolarization.
The most important cause of ST
segment abnormality (elevation or
depression) is myocardial ischaemia
or infarction.
5. Variant Angina (Prinzmetal
Angina)
• Pain is induced while at rest.
• Symptoms are caused by decreased blood flow to the heart muscle from the
spasm of the coronary artery.
• Although individuals with this form of angina may have significant coronary
atherosclerosis, the angina attacks are unrelated to physical activity, heart rate,
or blood pressure.
• Associated with ST-segment elevation on ECG.
• Generally responds promptly to coronary vasodilators, such as nitroglycerin and
calcium-channel blockers.
• But β-blockers are contraindicated.
6. Unstable angina (Acute
Coronary Syndrome)
• May involve coronary spasm and may also have the component of
atherosclerosis.
• The duration of manifestation is longer than the first two and has the
manifestation of myocardial infarction (MI).
• Lies between stable angina and MI.
• The pathology is similar to that involved in MI: a platelet-fibrin thrombus
associated with a ruptured atherosclerotic plaque but without complete
occlusion of the blood vessel.
9. Nitrates/Organic Nitrates
• Nitroglycerine, Isosorbide dinitrate, Isosorbide mononitrate.
• Preload reduction: Peripheral pooling of blood → decreased venous return
(preload reduction).
• After load reduction: Nitrates also produce some arteriolar dilation → slightly
decrease total peripheral resistance or afterload on the heart.
• Redistribution of coronary flow: In the arterial tree, nitrates preferentially relax
bigger conducting coronary arteries than arterioles or resistance vessels.
10.
11. MOA: The organic nitrate agents are prodrugs that are sources of NO. NO
activates the soluble isoforms of guanylyl cyclase, thereby increasing
intracellular levels of cGMP. In turn, cGMP promotes the
dephosphorylation of the myosin light chain and the reduction of
cytosolic Ca++ and leads to the relaxation of smooth muscle cells in
a broad range of issues.
12. Adverse effects:
Headache is the most common adverse effect of nitrates. High doses of nitrates can
also cause postural hypotension, facial flushing, and tachycardia.
Phosphodiesterase type 5 inhibitors such as sildenafil potentiate the action of
nitrates. To preclude the dangerous hypotension that may occur, this combination is
contraindicated.
Tolerance to the action of nitrates develops rapidly as the blood vessels become
desensitized to vasodilation. Tolerance can be overcome by providing a daily
“nitrate-free interval” to restore sensitivity to the drug.
Sudden withdrawal after prolonged exposure has resulted in a spasm of coronary
and peripheral blood vessels. Withdrawal of nitrates should be gradual.
13. β-Blockers
• Atenolol, Bisoprolol, Metoprolol, Propranolol
• Atenolol, metoprolol, propranolol, bisoprolol are used only for the prophylactic
therapy of angina; they are of no value in an acute attack.
• Effective in preventing exercise-induced angina.
• But are ineffective against the vasospastic form.
• Cardioselective β-blockers, such as metoprolol or atenolol, are preferred. Thus,
Propranolol is not preferred.
• Agents with intrinsic sympathomimetic activity (for example, pindolol) are less
effective and should be avoided in angina.
• The dose should be gradually tapered off over 5 to 10 days to avoid rebound
angina or hypertension.
14. MOA:
• Suppress the activation of the heart by blocking B1 receptors.
• I. Decrease the heart rate, resulting in:
• 1. decreased myocardial oxygen demand.
• 2. Increased oxygen delivery to the heart.
• II. Decrease myocardial contractility, helping to conserve energy/ decreased demand.
• III. Reduce the work of the heart and causing a slight decrease in BP
• ↓ HR,
• ↓ contractility,
• ↓ systolic wall tension,
• ↑ perfusion time
• Reasons for Using Nitrates and β-Blockers in Combination in Angina
• β-Blockers prevent reflex tachycardia and contractility produced by nitrate-induced hypotension.
• Nitrates prevent any coronary vasospasm produced by β- Blockers.
• Nitrates prevent increases in left ventricular filling pressure or preload resulting from the negative
inotropic effects produced by β-Blockers.
15. Calcium Channel Blockers
(CCBs)
• Amlodipine, Diltiazem, Felodipine, Nicardipine, Nifedipine, Verapamil.
• MOA
• Calcium is essential for muscular contraction.
• The CCBs protect the tissue by inhibiting the entrance of Ca+2 into cardiac and
smooth muscle cells of the coronary and systemic arterial beds.
• All CCBs are therefore arteriodilators that cause a decrease in vascular
resistance. Cause peripheral arterial vasodilation.
• Reduce myocardial contractility (-ve inotropic action).
• Result: decreased myocardial oxygen demand.
16. Pharmacological actions
Smooth muscle: The CCBs cause relaxation by decreasing the intracellular
availability of Ca++. The dihydropyridines (DHPs) have the most marked
smooth muscle relaxant and vasodilator action; verapamil is somewhat weaker
followed by diltiazem.
Heart: Calcium influx is increased in ischemia because of the membrane
depolarization that hypoxia produces. The calcium channel blocker protects the
tissue by inhibiting the entrance of calcium into cardiac and smooth muscle
cells of the coronary and systemic arterial beds and decreases smooth muscle
tone and vascular resistance, afterload.
17. Calcium Channel Blockers:
• Phenyl alkylamine: Verapamil:
• It dilates arterioles and decreases total peripheral resistance.
• It slows atrioventricular (AV) conduction directly and decreases heart rate,
contractility, blood pressure, and oxygen demand.
• It also has some α adrenergic blocking activity.
• Verapamil has greater negative inotropic effects than amlodipine, but it is a weaker
vasodilator.
• Verapamil should not be given with β blocker, digoxin, cardiac depressants like
quinidine and disopyramide it may cause bradycardia
• Verapamil and beta blockers can have similar actions in the body, so combining
them can cause your heart rate to slow down too much (bradycardia). It can also
make heart contractions weaker and lower your blood pressure too much.
Symptoms of this interaction may include dizziness, difficulty breathing, and
fatigue.
18. • Benzothiazepines: Diltiazem:
• Diltiazem also slows AV conduction, decreases the rate of firing of the sinus
node pacemaker, and is also a coronary artery vasodilator.
• Diltiazem can relieve coronary artery spasm and is particularly useful in
patients with variant angina.
• It is somewhat less potent vasodilators than nifedipine and verapamil and
has modest direct negative inotropic action, but the direct depression of SA
node A-V conduction is equivalent to verapamil.
19. • Dihydropyridine (DHP) Calcium channel blockers: Nifedipine:
• Nifedipine is the prototype DHP with a rapid onset and short duration of
action. It causes arteriolar dilation and decreases total peripheral resistance.
• Nifedipine is usually administered as an extended-release oral formulation.
• It causes direct depressant action on the heart in a higher dose.
• ADR: Frequent side effects are palpitation, flushing, ankle edema, hypotension,
headache, drowsiness, and nausea. Nifedipine has paradoxically increased the
frequency of angina in some patients.
20. Other dihydropyridines (DHP) calcium channel blockers:
Amlodipine, an oral dihydropyridine, functions mainly as an arteriolar vasodilator.
• Nitrendipine is a calcium channel blocker with additional action of
vasodilation action. Vasodilation action is due to the release of NO from the
endothelium and inhibits cAmp phosphodiesterase.
• Lacidipine is a highly vasoselective newer DHP.
• Nimodipine is short-acting DHP that penetrates the blood-brain barrier very
efficiently due to high lipid solubility.
• DHP with long duration of action: Lercanidipine, Benidipine.
21. Uses:
Calcium channel blockers can be safely given to patients with obstructive
lung disease and peripheral vascular disease in whom β blockers are
contraindicated.
CCB is used for the treatment of:
Angina pectoris
Hypertension
Cardiac arrhythmias
Hypertrophic cardiomyopathy
ADR: Lightheadedness. Low blood pressure. Slower heart rate.
22. Potassium Channel
Openers:
Nicorandil:
Antianginal action of nicorandil is mediated through ATP-sensitive K+ channels
(KATP) thereby hyperpolarizing vascular smooth muscles.
Nicorandil is well absorbed orally, nearly completely metabolized in the liver, and
excreted in the urine. Administered I.V. during angioplasty for acute MI, it is
believed to improve outcome.
ADR: Flushing, palpitation, weakness, headache, dizziness, nausea, and vomiting
23.
24. OTHER ANTIANGINAL
DRUGS
Antianginal Drugs Pharmacological Action
Dipyridamole
• Dipyridamol inhibits platelet aggregation.
• It is a powerful coronary dilator.
Trimetazidine
• These antianginal drugs act by
hemodynamic mechanisms.
• The MOA of trimetazidine is uncertain, but
it may improve cellular tolerance to ischemia
by inhibiting mitochondrial long-chain 3-
ketoacyl-CoAhiolase.
Ranolazine
• This novel antianginal drug primarily acts by
inhibiting late Na+ current in the
myocardium.
Ivabradine
• This ‘pure heart rate lowering antianginal
drugs has been introduced recently as an
alternative to β blocker.
• It blocks cardiac pacemaker (sino-atrial) cell
‘f’ channels.
Oxyphedrine • Improve myocardial metabolism.