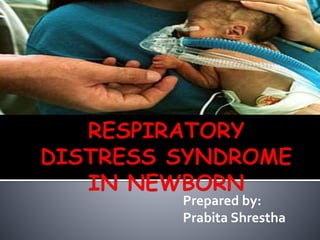
Respiratory distress syndrome (RDS) in newborn
•
7 likes•624 views

This presentation consists of Respiratory distress syndrome in newborn.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (10)
Similar to Respiratory distress syndrome (RDS) in newborn
Similar to Respiratory distress syndrome (RDS) in newborn (20)
Recently uploaded
Recently uploaded (20)
Respiratory distress syndrome (RDS) in newborn
- 2. Respiratory distress syndrome is one of the danger sign of the new born. It almost always occurs in preterm babies. The overall incidence is 10-15% but can be as high as 80% in neonates < 28 weeks. In addition to prematurity, asphyxia, acidosis, maternal diabetes and cesarean section baby and breech delivery can increase the risk of developing RDS.
- 3. Infant respiratory distress syndrome (IRDS), also called neonatal respiratory distress syndrome, respiratory distress syndrome of newborn, or increasingly surfactant deficiency disorder (SDD), and previously called hyaline membrane disease (HMD), is a syndrome in premature infants caused by developmental insufficiency of surfactant production and structural immaturity in the lungs. Increased alveolar fluid content, inadequate clearance of lung fluid, lack or inhibition of surfactant function, or reduced surface area for gas exchange is the basic pathology for respiratory distress.
- 4. 1. PULMONARY: Hyaline membrane disease (HMD) Meconium aspiration Pulmonary hypoplasia Broncho-pulmonary dysplasia Broncho-pneumonia Airway obstruction Transient tachypnea Pneumothorax Pulmonary edema
- 5. 2. CARDIOVASCULAR: Congenital heart disease i. Aortic stenosis ii. Coarctation of aorta iii. Cyanotic –Transposition of great vessels Heart failure Persistent pulmonary hypertension of newborn (PPHN)
- 6. 3. NON-CARDIOPULMONARY: Metabolic acidosis Hypoglycemia Hypo / hyperthermia Asphyxia Drugs (pethidine) Birth trauma Intracranial injury
- 7. Prematurity Maternal diabetes Multiple births Elective cesarean section without labor Perinatal asphyxia Cold stress Sepsis Metabolic acidosis Genetic disorders
- 8. In RDS, the basic abnormality is surfactant deficiency. It is lipoprotein containing phospholipids produced by alveolar cells, which helps to reduce surface tension in the alveoli.
- 9. Normal Expiration With Surfactant Surfactant Function Abnormal Respiration Without Surfactant
- 10. • In the absence of sufactant, surface tension increases and alveoli collapse during expiration. • During inspiration, more negative pressure is needed to keep alveoli patent • There is inadequate oxygenation and increased work of breathing. • Hypoxemia and acidosis results in pulmonary vasoconstriction • It further leads to right to left shunting across the foramen ovale • This worsens the hupoxia and leads to respiratory failure
- 11. Cyanosis Apnea Decreased urine output Grunting Nasal flaring Tachypnea upto 80 – 100 breathes/min Dyspnea Fine respiratory crackles Pronounced intercoastals / substernal retraction Flacidity Unresponsiveness Diminished breath sound Shock like state (in severe distress)
- 12. Blood gas analysis -- shows low oxygen and excess acid in the body fluids Chest x-ray -- shows a "ground glass" appearance to the lungs that is typical of the disease.This often develops 6 to 12 hours after birth. Lab tests – rule out infection as a cause of breathing problems Pulse oxymetry Pulmonary function test
- 13. 1. Taking steps to prevent premature birth can help prevent neonatal RDS. Good prenatal care and regular checkups beginning as soon as a woman discovers she is pregnant can help avoid premature birth. 2. The risk of RDS can also be lessened by the proper timing of a Cesarean delivery if needed. A lab test can be done before delivery to check the readiness of the baby’s lungs. When possible, the delivery should be delayed until tests show that the baby’s lungs have matured.
- 14. 3. Medicines called corticosteroids may help speed up lung maturity in the developing baby. They are often given to pregnant women between 24 and 34 weeks of pregnancy who seem likely to deliver in the next week. At times it may be possible to give other medicines to delay labor and delivery until the steroid medication has time to work. Antenatal corticosteroid therapy consists of either: Betamethasone 12 mg/dose IM for 2 doses, 24 hrs apart, or Dexamethasone 6 mg/dose IM for 4 doses, 12 hrs apart
- 15. 4. Prevent fetal hypoxia in diabetic mothers. 5. Avoid premature induction of labor. 6. Suction immediately after birth to patent the airway. 7. Early surfactant therapy: prophylactic use of surfactant in preterm newborn <27 weeks' gestation.
- 16. Neonates suspected to have RDS needs to treat in NICU. Administer oxygen and IV fluids. Mild distress can be managed without ventilator. If respiratory distress is significant or is associated with hypoxemia, hypercapnia or acidosis, the infant need ventilator support. Administer surfactant therapy: early rescue therapy within 2 hrs after birth is better than late rescue treatment when the full picture of RDS is evident.
- 17. Dosing may be divided into 2 alliquots and adminitered via a 5-Fr catheter passed in the ET
- 18. Antibiotics Amino glucosides pancuronium (musle relaxant) Frusemide Bicarbonate
- 19. Prognosis is good with appropriate and timely treatment. The condition often gets worse for 2 to 4 days after birth. It often improves slowly after that. Some infants with severe respiratory distress syndrome will die. Survival can be high as 60-80 % in infants >1000 gm.
- 20. Septicemia Bronchopulmonary dysplasia (BPD) Patent ductus arteriosus (PDA) Pulmonary hemorrhage Apnea/bradycardia Necrotizing enterocolitis (NEC) Retinopathy of prematurity (ROP) Hypertension Failure to thrive Intraventricular hemorrhage (IVH)
- 21. 1. Dutta D. C. Textbook of Obstetrics, 6th Edition, Page no. 474-477 2. Shrestha T. Essential Child Health Nursing, 1st Edition, Page no. 115-118 3. Tuitui R. Mannual of Midwifery III, 8th Edition, Page no. 223-227 4. http://emedicine.medscape.com/article/976034 -overview 5. https://en.wikipedia.org/wiki/Infant_respiratory _distress_syndrome 6. https://www.nlm.nih.gov/medlineplus/ency/arti cle/001563.htm