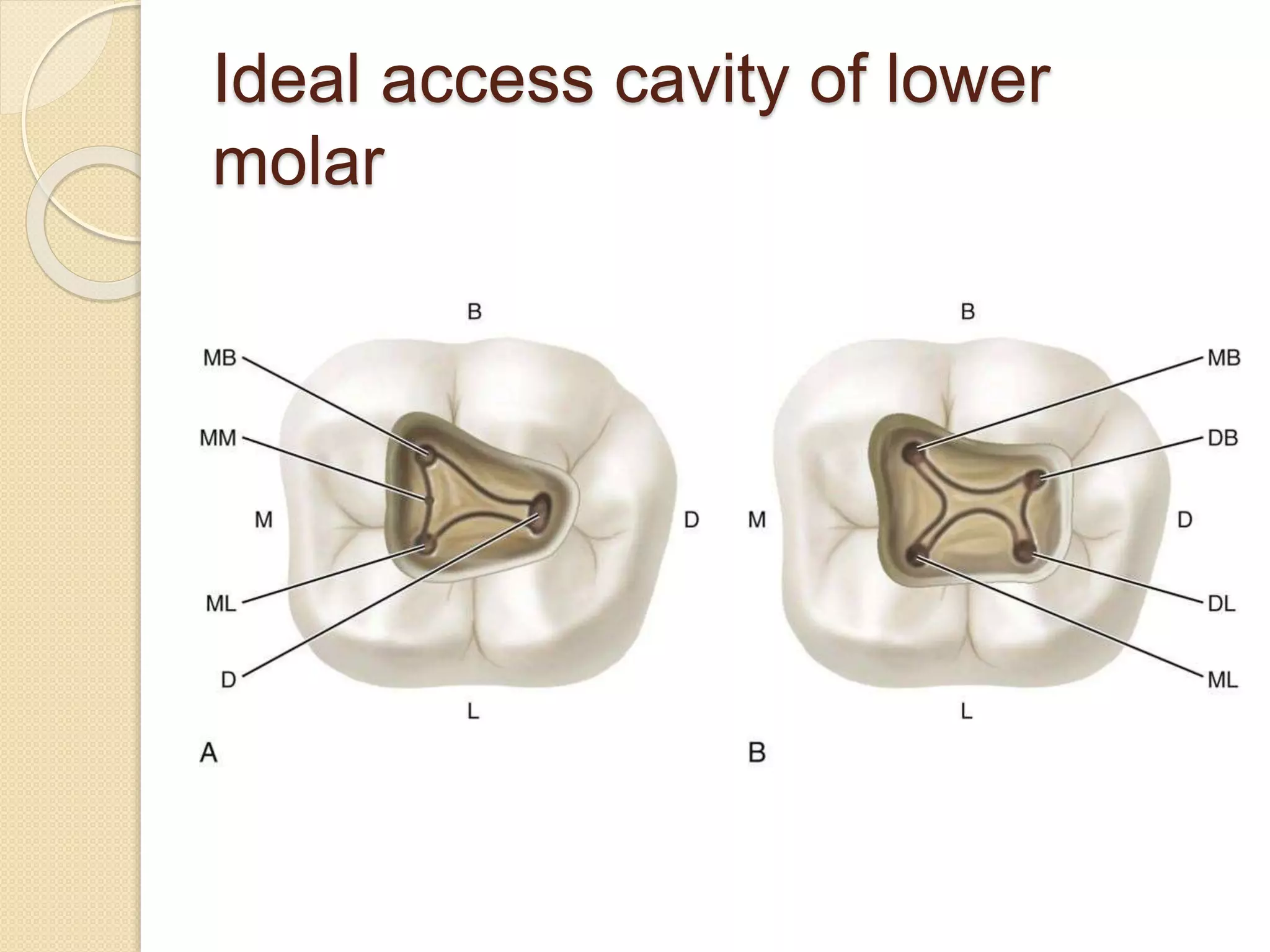
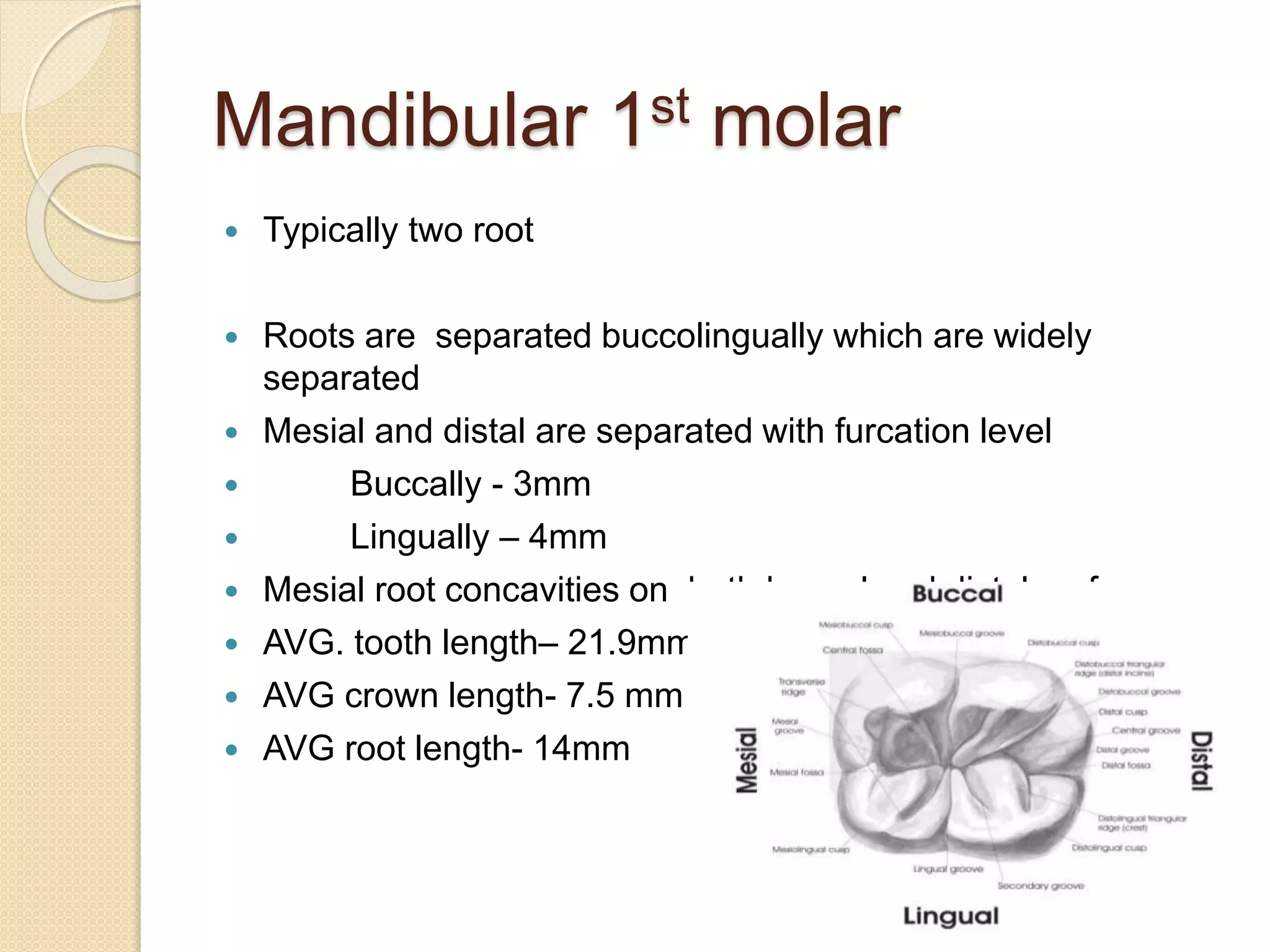
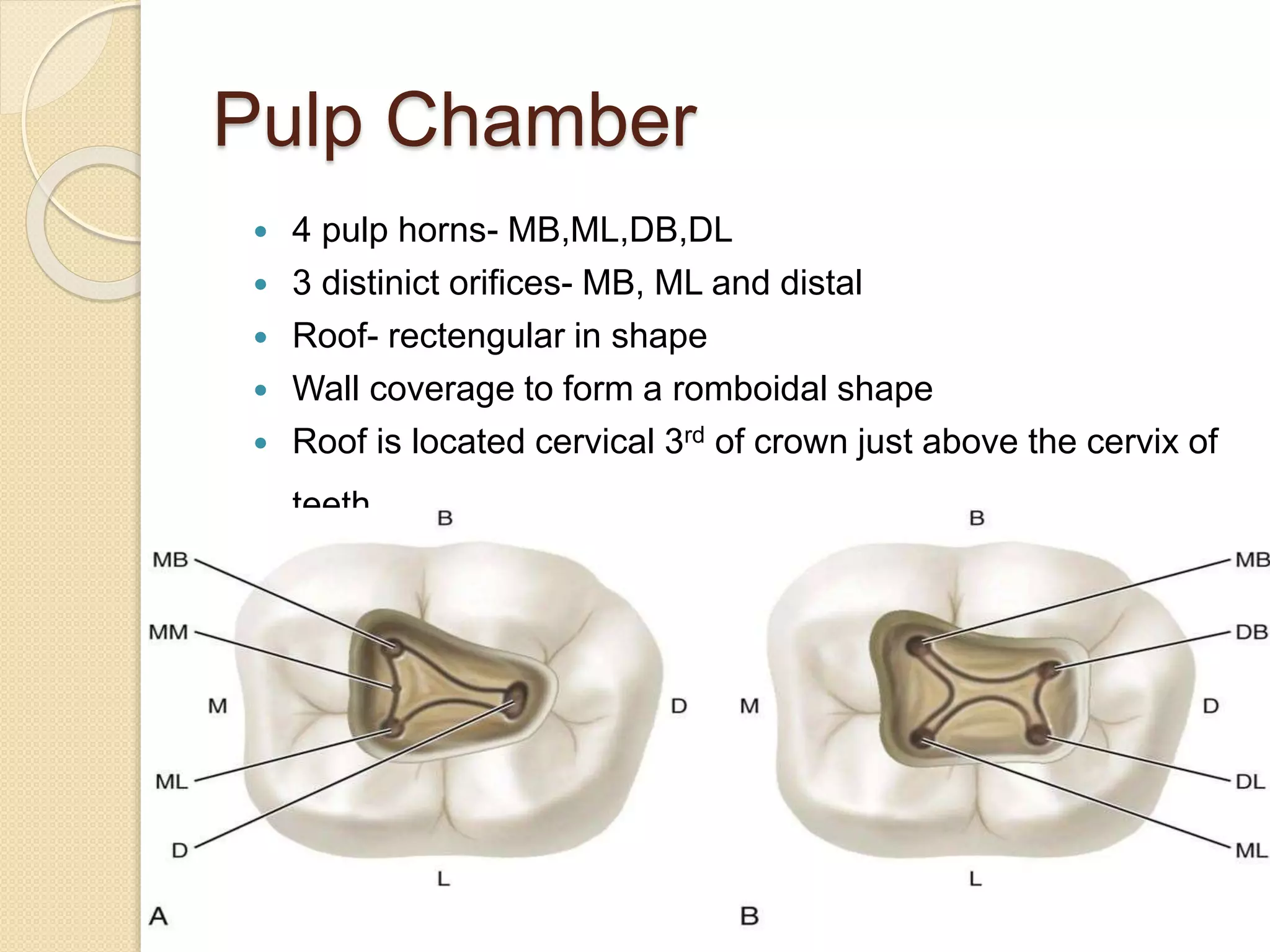
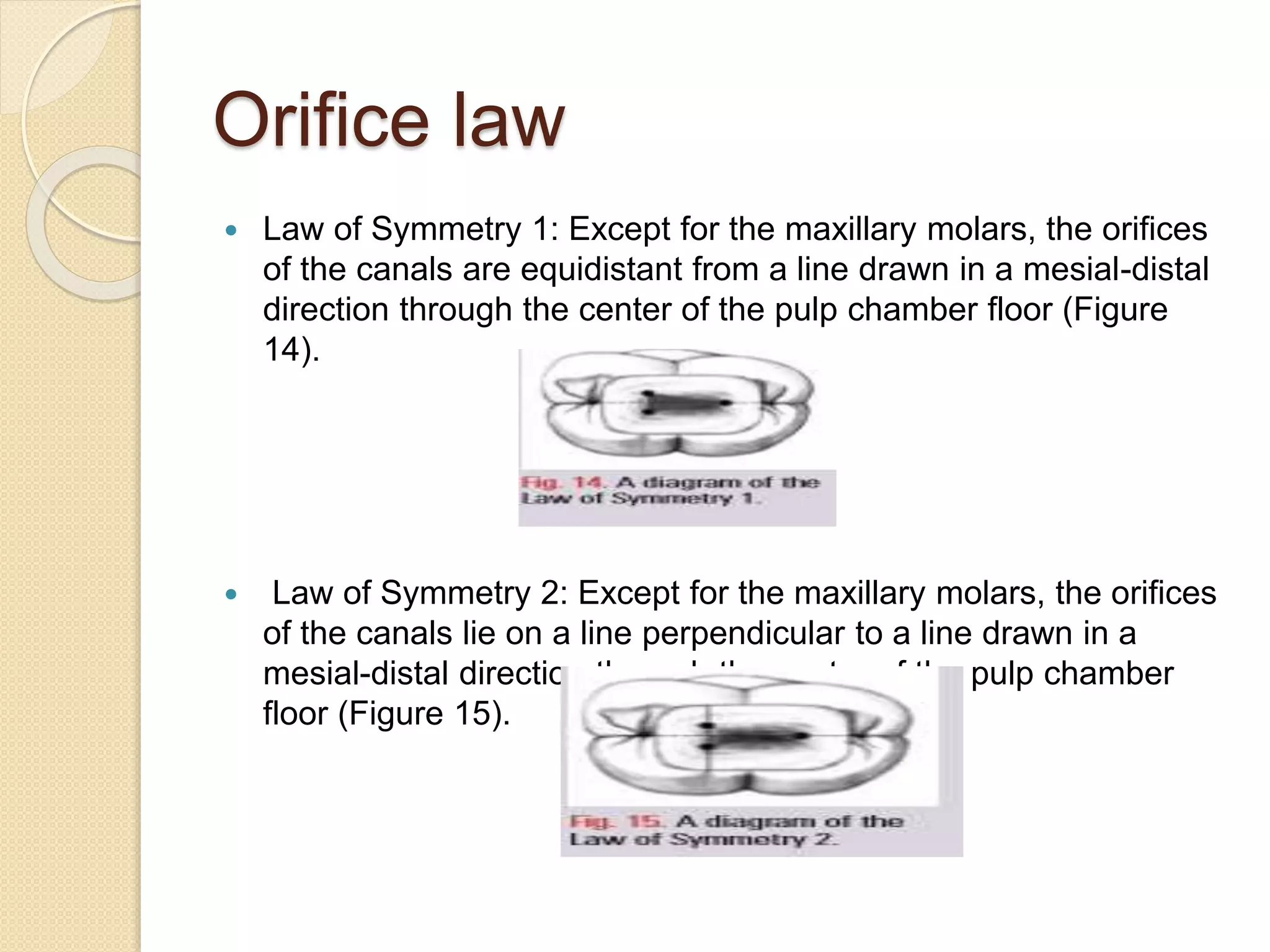
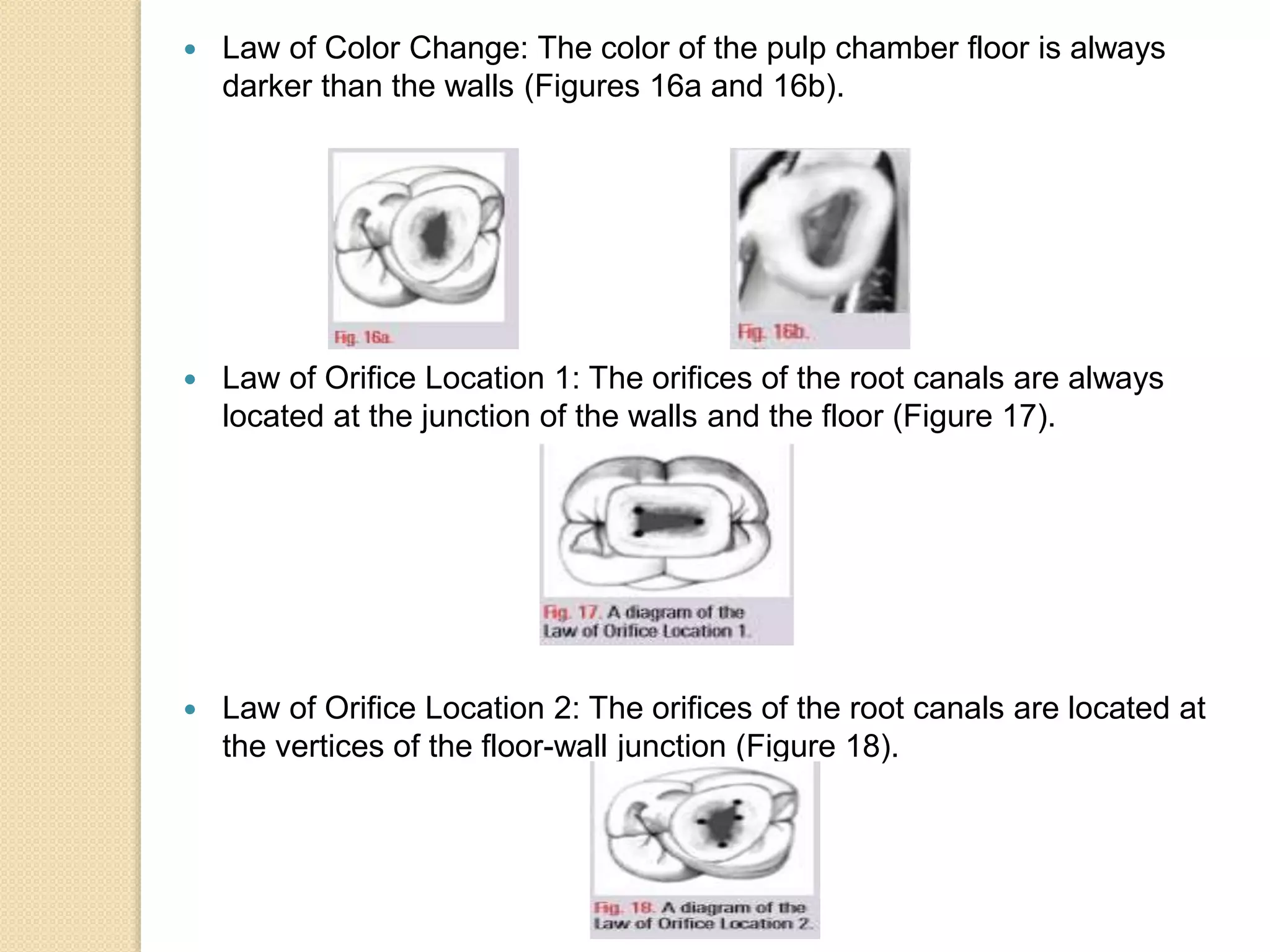
The document discusses the importance of proper access cavity preparation in lower first molars for successful root canal treatment. It outlines the anatomy of the lower first molar, including the typical root and canal morphology. The objectives of an ideal access are to locate all root canal orifices and maintain tooth structure. Laws of orifice location are described to help practitioners identify canal openings based on anatomical landmarks of the pulp chamber floor and walls. Common problems in access preparation and visualizing the floor are addressed, along with remedies to overcome each issue.