Downloaded 201 times

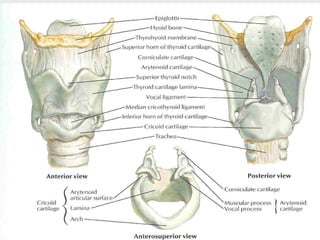
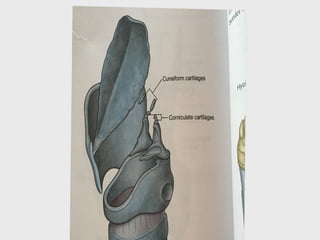
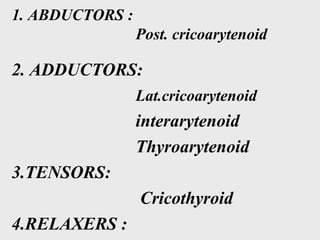
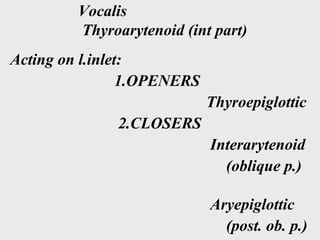
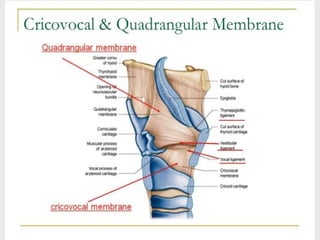
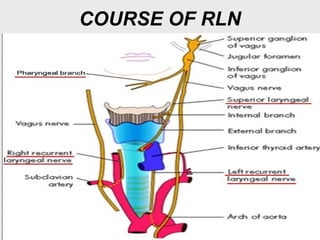
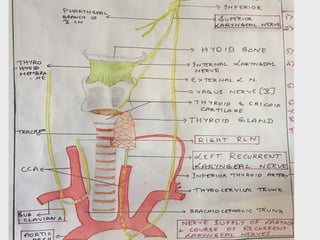
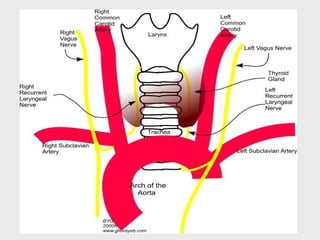
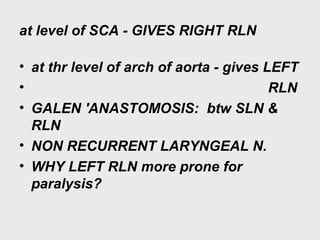
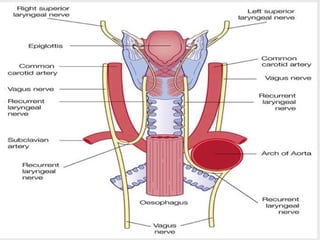
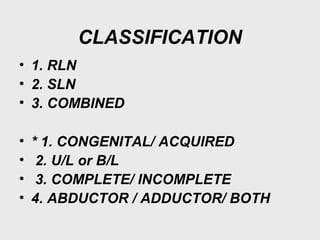
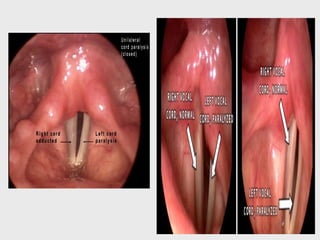

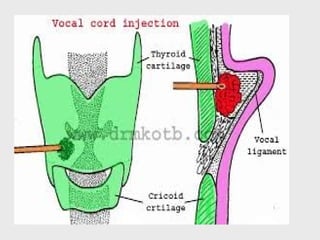
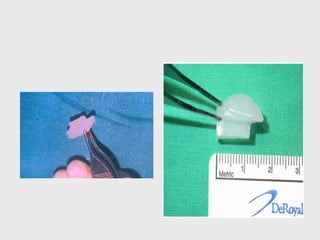
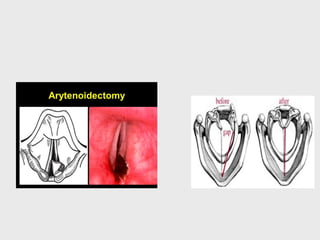
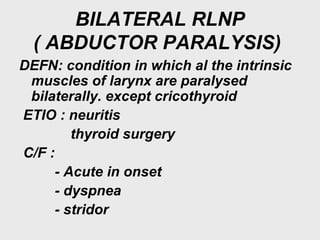
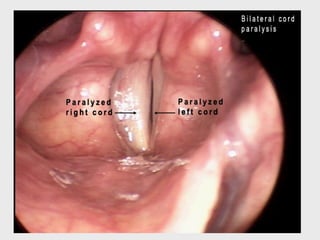
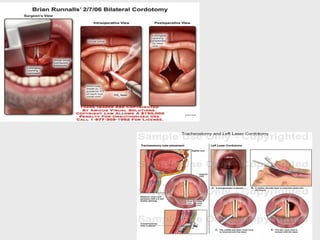
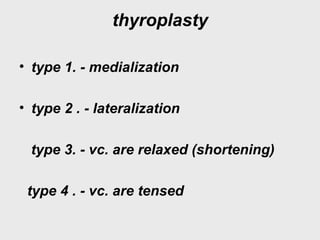
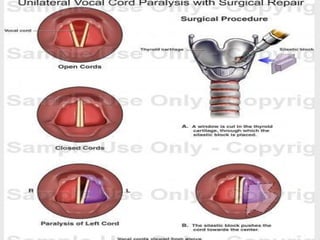



This document discusses recurrent laryngeal nerve paralysis (RLNP). It begins by describing normal vocal cord function and the effects of paralysis. It then covers the anatomy of the larynx and nerves involved. The causes, types, clinical features and investigations of unilateral and bilateral RLNP are explained. Management options are also summarized, including wait and see approach, laryngoplasty procedures, and in severe bilateral cases - tracheostomy or surgical techniques to lateralize the vocal cords.



































































