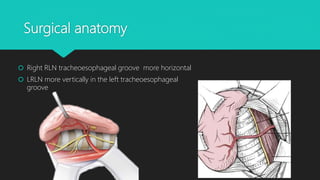
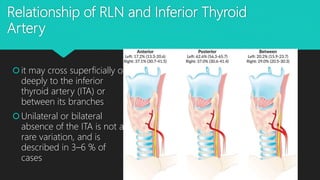
This document discusses the surgical anatomy and identification techniques for the recurrent laryngeal nerve (RLN) during thyroid surgery, highlighting the American Thyroid Association's guidelines and various approaches to RLN identification. A new medial approach is introduced, particularly useful in complex cases including revision surgeries and thyroid cancers with local invasion, yielding successful identification of RLNs in all cases studied. The study conducted on 71 patients demonstrated that this approach does not increase the risk of operative complications, making it a valuable technique for surgeons in specific situations.
![Introduction
2015 American Thyroid Association Guidelines
recommend “Visual identification of the recurrent
laryngeal [RLN] during dissection in all cases”](https://image.slidesharecdn.com/r-190117222927/85/Recurrent-laryngeal-nerve-2-320.jpg)