Download to read offline





















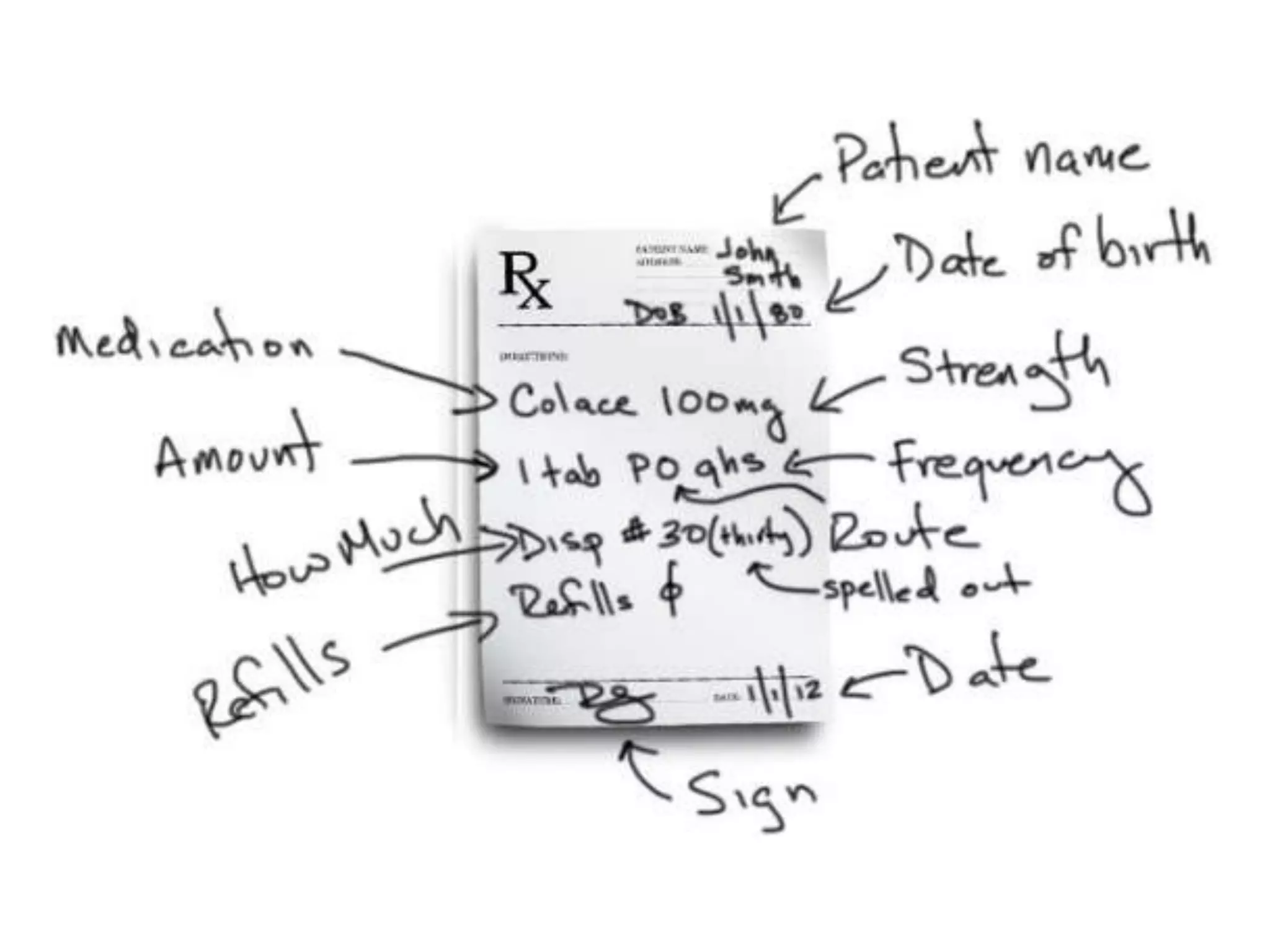



























The document provides guidance on rational prescription writing, including introducing the concept of "P-drugs" or personal first-choice drugs, outlining the steps in prescription writing, common abbreviations, and important instructions and information to provide to patients. It also discusses medication errors and how electronic prescribing can help reduce errors by suggesting alternative drugs. The overall goal is to teach students how to properly treat patients through skillful prescribing rather than just knowledge of drugs.