RANDOMIZATION
IN
CLINICAL TRIALS
Moderator:
Dr DhirendraK Mahawar
Associate Professor
Department of Pharmacology
SMS Medical College, Jaipur
Presented by:
Dr Harsh & Dr Deep
PG Residents
Department of Pharmacology
SMS Medical College, Jaipur
RANDOMIZATION
Random allocation ofintervention to the participants
All participants have the same chance of being allocated to each of the
study groups
4.
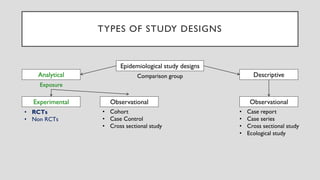
TYPES OF STUDYDESIGNS
Epidemiological study designs
Analytical Descriptive
Experimental Observational Observational
Comparison group
Exposure
• RCTs
• Non RCTs
• Cohort
• Case Control
• Cross sectional study
• Case report
• Case series
• Cross sectional study
• Ecological study
5.
“Prospective, ethically designedinvestigation in human subjects to
objectively discover, verify, & compare the results of two or more
therapeutic measures”
Therapeutic measures = Drugs, dosage regimens, other interventions
May be conducted in:
• Healthy volunteers: Determination of safety, tolerability, Pk
• Volunteer patients: Therapeutic efficacy
CLINICAL TRIALS
6.
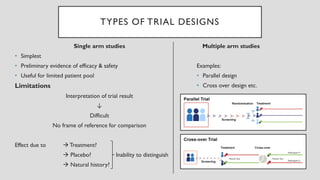
TYPES OF TRIALDESIGNS
Single arm studies
• Simplest
• Preliminary evidence of efficacy & safety
• Useful for limited patient pool
Limitations
Interpretation of trial result
↓
Difficult
No frame of reference for comparison
Effect due to → Treatment?
→ Placebo? Inability to distinguish
→ Natural history?
Multiple arm studies
Examples:
• Parallel design
• Cross over design etc.
7.
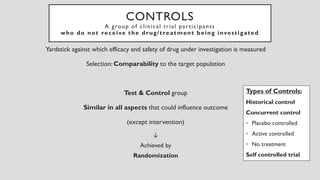
CONTROLS
A group ofclinical trial participants
who do not receive the drug/treatment being investigated
Yardstick against which efficacy and safety of drug under investigation is measured
Selection: Comparability to the target population
Test & Control group
Similar in all aspects that could influence outcome
(except intervention)
Types of Controls:
Historical control
Concurrent control
• Placebo controlled
• Active controlled
• No treatment
Self controlled trial
↓
Achieved by
Randomization
8.
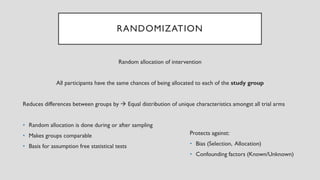
RANDOMIZATION
Random allocation ofintervention
All participants have the same chances of being allocated to each of the study group
Reduces differences between groups by → Equal distribution of unique characteristics amongst all trial arms
• Random allocation is done during or after sampling
• Makes groups comparable
• Basis for assumption free statistical tests
Protects against:
• Bias (Selection, Allocation)
• Confounding factors (Known/Unknown)
9.
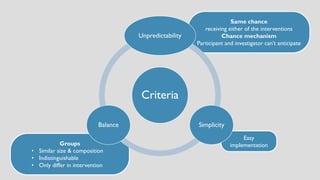
Easy
implementation
Groups
• Similar size& composition
• Indistinguishable
• Only differ in intervention
Same chance
receiving either of the interventions
Chance mechanism
Participant and investigator can’t anticipate
Criteria
Unpredictability
Simplicity
Balance
10.
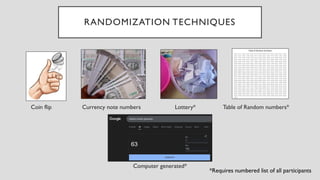
RANDOMIZATION TECHNIQUES
Coin flipCurrency note numbers Lottery* Table of Random numbers*
Computer generated*
*Requires numbered list of all participants
11.
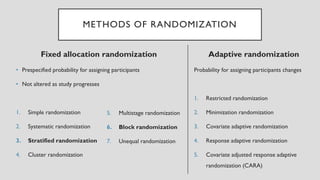
METHODS OF RANDOMIZATION
Fixedallocation randomization
• Prespecified probability for assigning participants
• Not altered as study progresses
1. Simple randomization
2. Systematic randomization
3. Stratified randomization
4. Cluster randomization
Adaptive randomization
Probability for assigning participants changes
1. Restricted randomization
2. Minimization randomization
3. Covariate adaptive randomization
4. Response adaptive randomization
5. Covariate adjusted response adaptive
randomization (CARA)
5. Multistage randomization
6. Block randomization
7. Unequal randomization
12.
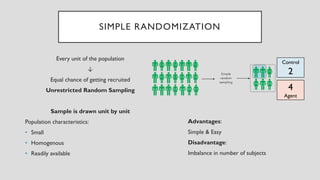
4
Agent
Control
2
SIMPLE RANDOMIZATION
Every unitof the population
↓
Equal chance of getting recruited
Unrestricted Random Sampling
Sample is drawn unit by unit
Population characteristics:
• Small
• Homogenous
• Readily available
Advantages:
Simple & Easy
Disadvantage:
Imbalance in number of subjects
13.
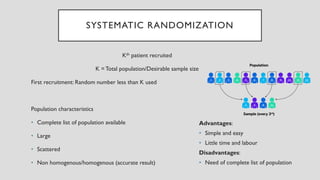
SYSTEMATIC RANDOMIZATION
Kth patientrecruited
K =Total population/Desirable sample size
First recruitment: Random number less than K used
Population characteristics
• Complete list of population available
• Large
• Scattered
• Non homogenous/homogenous (accurate result)
Advantages:
• Simple and easy
• Little time and labour
Disadvantages:
• Need of complete list of population
14.
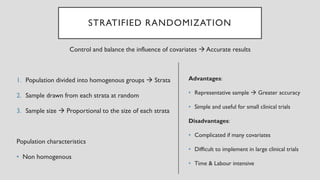
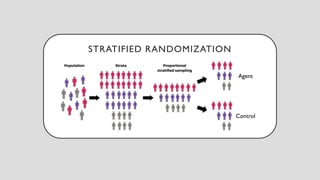
STRATIFIED RANDOMIZATION
Control andbalance the influence of covariates → Accurate results
1. Population divided into homogenous groups → Strata
2. Sample drawn from each strata at random
3. Sample size → Proportional to the size of each strata
Population characteristics
• Non homogenous
Advantages:
• Representative sample → Greater accuracy
• Simple and useful for small clinical trials
Disadvantages:
• Complicated if many covariates
• Difficult to implement in large clinical trials
• Time & Labour intensive
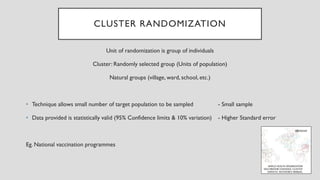
CLUSTER RANDOMIZATION
Unit ofrandomization is group of individuals
Cluster: Randomly selected group (Units of population)
Natural groups (village, ward, school, etc.)
• Technique allows small number of target population to be sampled - Small sample
• Data provided is statistically valid (95% Confidence limits & 10% variation) - Higher Standard error
Eg. National vaccination programmes
17.
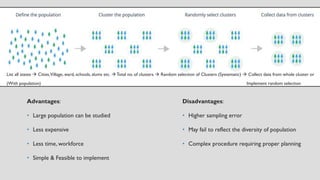
Advantages:
• Large populationcan be studied
• Less expensive
• Less time, workforce
• Simple & Feasible to implement
List all states → Cities,Village, ward, schools, slums etc. →Total no. of clusters → Random selection of Clusters (Systematic) → Collect data from whole cluster or
(With population) Implement random selection
Disadvantages:
• Higher sampling error
• May fail to reflect the diversity of population
• Complex procedure requiring proper planning
18.
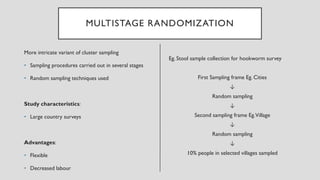
MULTISTAGE RANDOMIZATION
More intricatevariant of cluster sampling
• Sampling procedures carried out in several stages
• Random sampling techniques used
Study characteristics:
• Large country surveys
Advantages:
• Flexible
• Decreased labour
Eg. Stool sample collection for hookworm survey
First Sampling frame Eg. Cities
↓
Random sampling
↓
Second sampling frame Eg.Village
↓
Random sampling
↓
10% people in selected villages sampled
19.
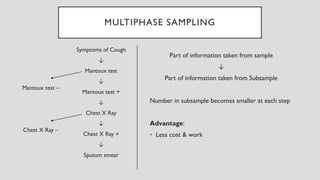
MULTIPHASE SAMPLING
Symptoms ofCough
↓
Mantoux test
↓
Mantoux test +
↓
Chest X Ray
↓
Chest X Ray +
↓
Sputum smear
Part of information taken from sample
↓
Part of information taken from Subsample
Number in subsample becomes smaller at each step
Advantage:
• Less cost & work
Mantoux test –
Chest X Ray –
20.
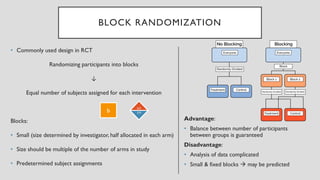
BLOCK RANDOMIZATION
• Commonlyused design in RCT
Randomizing participants into blocks
↓
Equal number of subjects assigned for each intervention
Blocks:
• Small (size determined by investigator, half allocated in each arm)
• Size should be multiple of the number of arms in study
• Predetermined subject assignments
Advantage:
• Balance between number of participants
between groups is guaranteed
Disadvantage:
• Analysis of data complicated
• Small & fixed blocks → may be predicted
b/2
b/2
b
21.
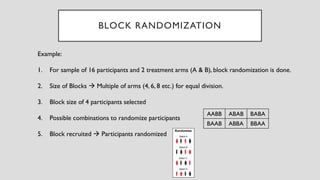
Example:
1. For sampleof 16 participants and 2 treatment arms (A & B), block randomization is done.
2. Size of Blocks → Multiple of arms (4, 6, 8 etc.) for equal division.
3. Block size of 4 participants selected
4. Possible combinations to randomize participants
5. Block recruited → Participants randomized
BLOCK RANDOMIZATION
AABB ABAB BABA
BAAB ABBA BBAA
22.
UNEQUAL RANDOMIZATION
• Equalrandomization → Maximizes statistical power
• Issues: Ethical/Economical/Practical
Eg. Cost difference between treatments, Outcome difference between arms (Placebo)
↓
Randomize fewer patients into expensive treatment or to less efficacious treatment
• Smaller randomization ratio may be used (2:1)
• Modest loss of statistical power → Cost savings / More practical & ethical design
23.
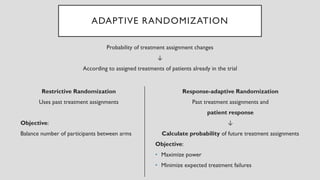
ADAPTIVE RANDOMIZATION
Restrictive Randomization
Usespast treatment assignments
Objective:
Balance number of participants between arms
Probability of treatment assignment changes
↓
According to assigned treatments of patients already in the trial
Response-adaptive Randomization
Past treatment assignments and
patient response
↓
Calculate probability of future treatment assignments
Objective:
• Maximize power
• Minimize expected treatment failures
24.
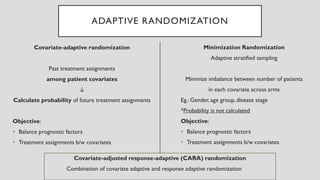
ADAPTIVE RANDOMIZATION
Covariate-adaptive randomization
Pasttreatment assignments
among patient covariates
↓
Calculate probability of future treatment assignments
Objective:
• Balance prognostic factors
• Treatment assignments b/w covariates
Minimization Randomization
Adaptive stratified sampling
Minimize imbalance between number of patients
in each covariate across arms
Eg.: Gender, age group, disease stage
*Probability is not calculated
Objective:
• Balance prognostic factors
• Treatment assignments b/w covariates
Covariate-adjusted response-adaptive (CARA) randomization
Combination of covariate adaptive and response adaptive randomization
25.
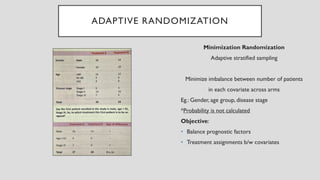
ADAPTIVE RANDOMIZATION
Minimization Randomization
Adaptivestratified sampling
Minimize imbalance between number of patients
in each covariate across arms
Eg.: Gender, age group, disease stage
*Probability is not calculated
Objective:
• Balance prognostic factors
• Treatment assignments b/w covariates
26.
RECOMMENDED METHODS
Large study(several hundred participants)
Blocked randomization or stratified randomization
Small study (~100 participants)
Blocked randomization or stratified randomization
Very small study (~50 participants)
Adaptive randomization
27.
REFERENCES
1. Sougata Sarkar,VartikaSrivastava, Manjushree Mohanty. Postgraduate Pharmacology. Second edition. Hyderabad:
Paras Medical Books; 2025.
2. Rituparna Maiti. Postgraduate topics in Pharmacology.Third Edition. Hyderabad: Paras Medical Books; 2019.
3. Khanal Arun Bhadra, Jaypee Brothers (Jaypeedigital. Mahajan’s Methods in Biostatistics for Medical Students and
ResearchWorkers. Jaypee Brothers Medical Publisher (P) Ltd; 2016.
4. Kamalu I, Niyomwungere F, İlker Etikan.A Comprehensive Analysis of Cluster Sampling versus Multi-Stage Sampling
Techniques: Methodologies,Applications, and Comparative Insights. Pioneer Journal of Biostatistics and Medical
Research [Internet]. 2024 Mar 26;2(1):21–30.
5. WHO. Survey methods [Internet]. www.who.int.Available from: https://www.who.int/teams/immunization-
vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/survey-
methods

![REFERENCES
1. Sougata Sarkar,Vartika Srivastava, Manjushree Mohanty. Postgraduate Pharmacology. Second edition. Hyderabad:
Paras Medical Books; 2025.
2. Rituparna Maiti. Postgraduate topics in Pharmacology.Third Edition. Hyderabad: Paras Medical Books; 2019.
3. Khanal Arun Bhadra, Jaypee Brothers (Jaypeedigital. Mahajan’s Methods in Biostatistics for Medical Students and
ResearchWorkers. Jaypee Brothers Medical Publisher (P) Ltd; 2016.
4. Kamalu I, Niyomwungere F, İlker Etikan.A Comprehensive Analysis of Cluster Sampling versus Multi-Stage Sampling
Techniques: Methodologies,Applications, and Comparative Insights. Pioneer Journal of Biostatistics and Medical
Research [Internet]. 2024 Mar 26;2(1):21–30.
5. WHO. Survey methods [Internet]. www.who.int.Available from: https://www.who.int/teams/immunization-
vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/survey-
methods](https://image.slidesharecdn.com/randomization-251203040306-9d699461/85/Randomization-27-320.jpg)