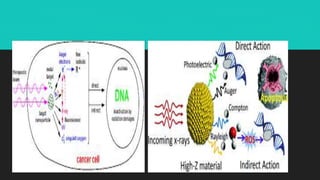
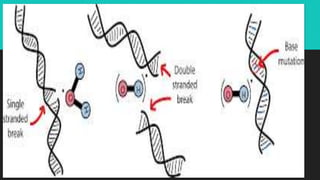
Radiotherapy uses ionizing radiation to treat cancer. There are two main types - external beam radiotherapy which uses radiation from outside the body, and brachytherapy which places radioactive sources inside or near the tumor. The radiation damages cancer cell DNA directly or through free radicals, limiting cell division and causing cell death. Different techniques are used depending on the tumor location and size to deliver precise radiation doses while sparing surrounding healthy tissues.









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






