BRACHIAL PLEXUS: INTRODUCTION
.
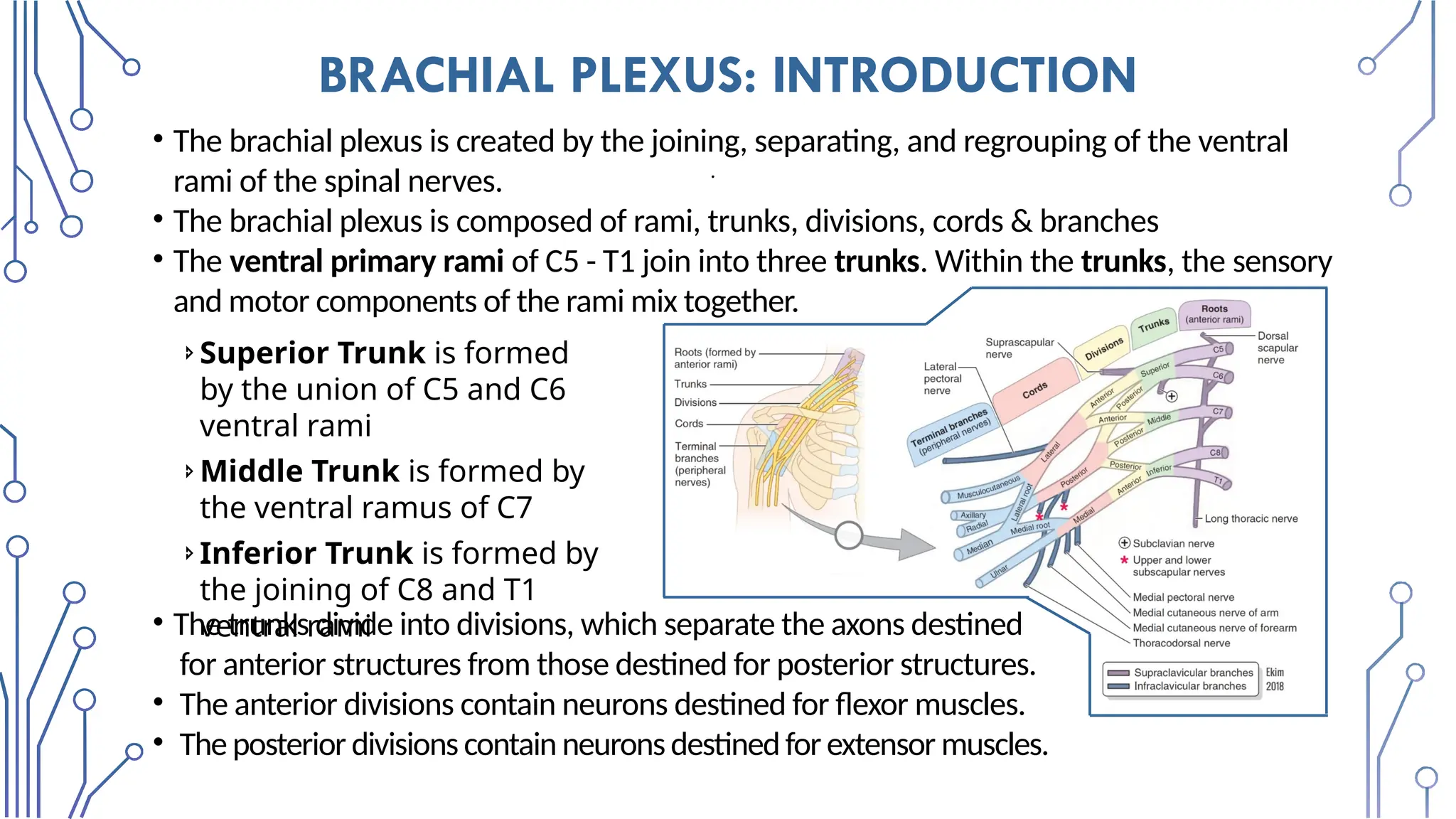
•The brachial plexus is created by the joining, separating, and regrouping of the ventral
rami of the spinal nerves.
• The brachial plexus is composed of rami, trunks, divisions, cords & branches
• The ventral primary rami of C5 - T1 join into three trunks. Within the trunks, the sensory
and motor components of the rami mix together.
Superior Trunk is formed
by the union of C5 and C6
ventral rami
Middle Trunk is formed by
the ventral ramus of C7
Inferior Trunk is formed by
the joining of C8 and T1
ventral rami
• The trunks divide into divisions, which separate the axons destined
for anterior structures from those destined for posterior structures.
• The anterior divisions contain neurons destined for flexor muscles.
• The posterior divisions contain neuronsdestinedfor extensor muscles.
3.
SUPPLY DISTRIBUTION OFTHE BRACHIAL PLEXUS
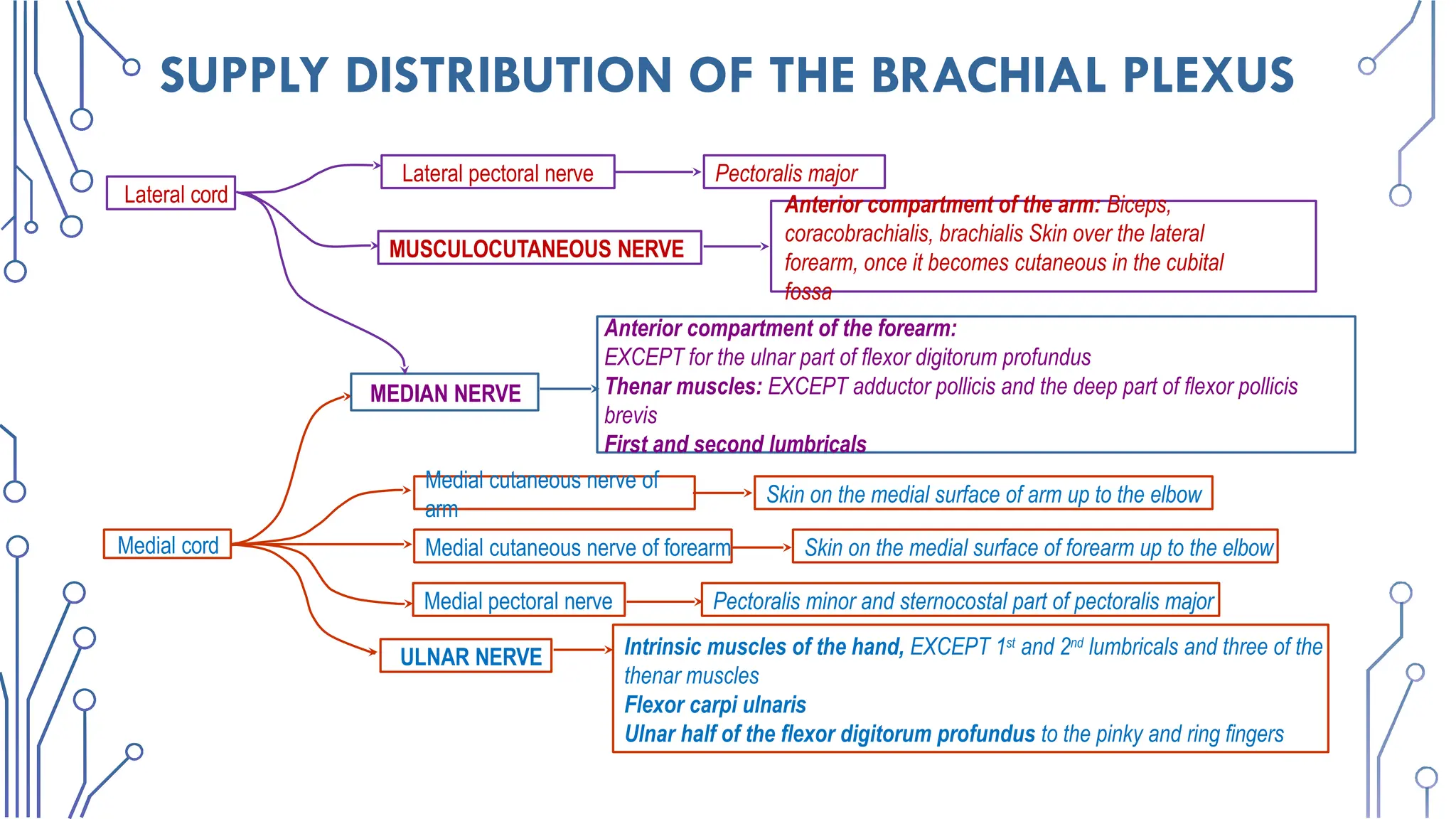
Medial cutaneous nerve of
arm
Skin on the medial surface of arm up to the elbow
Medial cord Medial cutaneous nerve of forearm Skin on the medial surface of forearm up to the elbow
Medial pectoral nerve Pectoralis minor and sternocostal part of pectoralis major
ULNAR NERVE Intrinsic muscles of the hand, EXCEPT 1st
and 2nd
lumbricals and three of the
thenar muscles
Flexor carpi ulnaris
Ulnar half of the flexor digitorum profundus to the pinky and ring fingers
MEDIAN NERVE
Anterior compartment of the forearm:
EXCEPT for the ulnar part of flexor digitorum profundus
Thenar muscles: EXCEPT adductor pollicis and the deep part of flexor pollicis
brevis
First and second lumbricals
MUSCULOCUTANEOUS NERVE
Anterior compartment of the arm: Biceps,
coracobrachialis, brachialis Skin over the lateral
forearm, once it becomes cutaneous in the cubital
fossa
Lateral cord
Pectoralis major
Lateral pectoral nerve
4.
SUPPLY DISTRIBUTION OFTHE BRACHIAL PLEXUS
Upper subscapular nerve Superior half of subscapularis
Posterior cord AXILLARY NERVE
Glenohumeral joint
Teres minor
Deltoid, Skin over the deltoid
RADIAL NERVE
All muscles in the posterior compartment
of the arm and forearm
Skin over posterior and inferolateral forearm
Some of the dorsum of the hand
Thoracodorsal nerve Latissimus Dorsi
Lower subscapular nerve Inferior half of subscapularis and teres major
Serratus anterior
Rhomboids;
levator scapulae
Subclavius,
Sternoclavicular joint
Supraspinatus
Infraspinatus
Glenohumeral joint
Supraclavicular branches
Long Thoracic nerve
Dorsal scapular nerve
Nerve to subclavius
Suprascapular nerve
5.
SUPPLY DISTRIBUTION OFTHE BRACHIAL PLEXUS
The divisions fuse into cords that retain the anterior-posterior
segregation but allow further mixing of axons from different spinal
segments. The cords are named for their anatomical relationship relative
to the to the second part of the axillary artery.
Branches are the named nerves that branch from the brachial plexus.
The branches can be described as organized into different groups.
Terminal branches are the nerves formed from the distal terminations of
the medial, lateral, and posterior cords (light blue branches on picture).
Infraclavicular branches are named nerves that branch from the medial,
lateral, and posterior cord (dark blue branches on picture).
Supraclavicular branches are branches of the rami or trunks (dark purple
branches on picture).
6.
SUPRACLAVICULARBRANCHES:DORSALSCAPULAR,LONGTHORACIC,SUPRASCAPULAR,AND
SUBCLAVIANNERVES
Nerve Origin Course
Structures
innervated
Dorsal
scapular
Posterioraspect of
anterior ramus of C5
with a frequent
contribution from C4
Pierces middle scalene; descends
deep to Levator scapulae and
Rhomboids
Motor:
Rhomboids; occasionally
supplies Levator scapulae
Long
thoracic
Posterior aspect of
anterior rami of C5, C6,
C7
Passes through cervico-axillary
canal, descends posterior to C8
and T1 roots of plexus (anterior
rami); runs inferiorly on superficial
surface of serratus anterior
Motor:
Serratus anterior
Suprascapula
r
Superior trunk, receiving
fibers from C5, C6 and
often C4
Passes laterally across lateral
cervical region (posterior triangle
of neck), superior to brachial
plexus; then passes through
Motor:
Supraspinatus and
Infraspinatus muscles
Sensory:
7.
Long Thoracic Nerve(Distal
Part)
Serratus Anterior Muscle
Long Thoracic
Nerve
Subclavian Nerve
Subclavius Muscle
Scalenus Anterior Muscle
(Cut)
Scalenus Medius
Muscle
Posterior View of Brachia Plexus with Middle
Scalene (Faded)
Scalenus Middle
(Faded)
Superior Trunk of
Brachial
Plexus(Truncus
superior
plexusbrachialis)
Suprascapular Nerve
Dorsal Scapular
Nerve
8.
INFRACLAVICULAR BRANCHES:
UPPER ANDLOWER SUBSCAPULAR,THORACODORSAL NERVES
Nerve Origin Course
Structures
innervated
Upper
subscapular
Side branch of
posterior cord,
receiving fibers from
C5
• Courses posteriorly to
enter subscapularis
Motor:
superior portion of
subscapularis muscle
Lower
subscapular
Side branch of
posterior cord,
receiving fibers from
C6
• Courses inferolaterally
(deep to subscapular
artery and vein) to enter
subscapularis and teres
major muscles
Motor:
inferior portion of the
subscapularis and
teres major muscles
Thoracodors
al
Side branch of
posterior cord,
receiving fibers from
C6, C7, C8
• Arises between upper
and lower subscapular
nerves (middle scapular
nerve)
• Courses inferolaterally
Motor:
Latissimus dorsi
muscle
9.
INFRACLAVICULAR BRANCHES:
MEDIAL CUTANEOUSNERVES OF ARM AND FOREARM
Nerve Origin Course
Structures
innervated
Medial
cutaneous
nerve of arm
Side branches of
medial cord,
receiving fibers
from C8, T1
•Smallest nerve of brachial
plexus
•Courses along medial side of
axillary and brachial veins
and communicates with
intercostobrachial nerve
Sensory: skin of
medial side of arm, as
far distal as medial
epicondyle of
humerus and
olecranon of ulna
Medial
cutaneous
nerve of
forearm
•Initially runs with ulnar
nerve
•Then pierces deep fascia
with basilic vein and enters
Sensory: skin of
medial side of
forearm, as far distal
as wrist
10.
TERMINAL BRANCHES: MUSCULOCUTANEOUSNERVE
Nerve Origin Course Structures innervated
Musculo-
cutaneou
s
Terminal
branch of
lateral cord,
receiving
fibers from
C5–C7
•Exits axilla by
piercing
coracobrachialis
•Descends through
the arm between
biceps brachii and
brachialis
•Continues into
forearm as lateral
cutaneous nerve
of forearm
Motor: muscles of
anterior compartment
of arm
(coracobrachialis,
biceps brachii &
brachialis)
Sensory: skin of
lateral aspect of
forearm
CLINICAL ANATOMY: Lesions of the musculocutaneous nerve can result in
both muscle weakness and loss/reduction of sensation.
• Weakness of elbow flexion and supination result. Supination weakness
occurs because the biceps brachii is major contributor to supination of the
forearm.
• Sensory loss occurs on the lateral side of the forearm in the domain of the
lateral cutaneous nerve of the forearm.
11.
TERMINAL BRANCHES: MEDIANNERVE
Nerve Origin Course Structures innervated
Median
Lateral root of
median nerve is a
terminal branch of
lateral cord (C6,
C7) Medial root of
median nerve is a
terminal branch of
medial cord (C8,
T1)
•Lateral and medial roots
merge to form median
nerve (lateral position
relative to the axillary
artery)
•Descends through arm
adjacent to brachial artery,
with nerve gradually
crossing anterior to artery
to lie medial to artery in
cubital fossa
Motor: muscles of anterior
forearm compartment (except
flexor carpi ulnaris and ulnar half
of flexor digitorum profundus),
lumbricals of digits 2, 3 and
thenar muscles (abductor pollicis
brevis, opponens pollicis, flexor
pollicis brevis)
Sensory: skin of palm, palmar
side of digits 1-3, lateral palmar
side of digit 4 and the distal half
on the dorsal surface of digits 1-4
CLINICAL ANATOMY:
Lesions of the median nerve (and its branches) will be explored in
upcoming units when we study the anatomical area in which a lesion
typically occurs.
TERMINAL BRANCHES: ULNARNERVE
CLINICAL ANATOMY:
Lesions of the ulnar nerve (and its branches) will be explored in
upcoming units when we study the anatomical area in which a lesion
typically occurs.
Nerve Origin Course Structures innervated
Ulnar Larger terminal
branch of media
cord, receiving
fibers from C8, T1
and often C7
•Descends medial arm
•Courses posterior to
medial epicondyle of
humerus
•Descends along the
ulnar aspect of forearm
to hand
Motor: flexor carpi ulnaris and
ulnar half of flexor digitorum
profundus (forearm); most intrinsic
muscles of the hand
Sensory: skin of hand medial to
midline of digit 4, medial half of
digit 4, all of digit 5
TERMINAL BRANCHES: AXILLARYNERVE
Nerve Origin Course Structures
innervated
Axillary Terminal branch
of posterior cord,
receiving fibers
from C5, C6
• Exits axilla posteriorly by
passing through the
quadrangular space with
posterior circumflex
humeral artery
• Gives rise to superior
lateral brachial cutaneous
nerve
• Winds around surgical neck
of humerus deep to deltoid
Motor: teres minor
and deltoid muscles
Sensory:
superolateral arm
(skin over inferior
part of deltoid
muscle),
glenohumeral
(shoulder) joint
SURGICAL NECK FRACTUREOF HUMERUS
CLINICAL ANATOMY:
Because of their anatomical relationship to the proximal humerus &
glenohumeral joint, the axillary nerve and posterior circumflex humeral
vessels are at risk of injury in shoulder dislocations and when the surgical
neck of the humerus is fractured.
18.
TERMINAL BRANCHES: RADIALNERVE
Nerv
e
Origin Course Structures
innervated
Radial
Larger terminal
branch of
posterior cord
(largest branch
of plexus),
receiving fibers
from C5–T1
•Exits axilla posterior to axillary
artery and passes posterior to
humerus in radial groove with
deep brachial artery, between
lateral and medial heads of triceps
•Perforates lateral intermuscular
septum
•Enters cubital fossa, dividing into
superficial (cutaneous) and deep
(motor) radial nerves
Motor: all muscles of
posterior compartments of
arm and forearm
Sensory: skin of posterior
and inferolateral arm,
posterior forearm, and
dorsum of hand lateral to
axial line of digit 4
SCAPULAR WINGING
CLINICAL ANATOMY:
Medialwinging of the scapula is the result of serratus anterior paralysis from injury
to the long thoracic nerve. The most common etiology is neuropraxia after blunt
trauma or a stretch injury. In addition, surgical procedures in the thoracic region
such as radical mastectomy, resection of the first rib, and transthoracic
sympathectomy can expose the long thoracic nerve and make it susceptible to
damage.
To test for medial scapular winging, ask patient to push against a wall and observe
the inferior angle of the scapula. If the nerve is damaged, the inferior angle and
medial border will project from the posterior thoracic wall (medial scapular
“winging”). In addition, a person with long thoracic nerve injury will have difficulty
abducting the arm past a horizonal position (90 degrees) due to an inability to
upwardly rotate the scapula.
22.
Two mnemonics thatmight help remember
medial scapular winging:
C5,6,7 wings to heaven: The serratus anterior is
innervated by the long thoracic nerve (C5-C7), so
damage to the nerve results in (medial) winging of
the scapula.
SALT on the birds wings: SA=serratus anterior,
LT=long thoracic nerve. Damage to the long
thoracic nerve results in (medial) winging of the
scapula.
CLINICAL ANATOMY:
Lateral winging of the scapula results from a
dysfunction in the trapezius (spinal accessory nerve:
CN XI) and/or rhomboid muscles (dorsal scapular
nerve). In lateral winging, the scapula is excessively
23.
BRACHIAL PLEXUS: UPPERTRUNK INJURY
Injury to the upper trunk (formed by C5-C6) of the brachial plexus can result in Erb-
Duchenne paralysis (palsy). It is caused by a violent distraction (lateral bending) of the
head away from the shoulder. This can occur in trauma, such as from a fall off a
motorcycle or horse.
In addition, it can occur from traction placed on the brachial plexus during a difficult
birth (a common complication of shoulder dystocia) (bottom right figure). The resulting
presentation of the upper extremity is described as a “waiter’s tip hand,” in which the
arm rests in medial rotation, the forearm is pronated, and the wrist is flexed (bottom left
figure).
24.
BRACHIAL PLEXUS: UPPERTRUNK INJURY
The following nerves are involved in an injury to the upper trunk.
•Axillary nerve:
Deltoid paralysis results in an inability to laterally rotate and
abduct the arm. When at rest, deltoid paralysis results in the arm
by the side and medially rotated (medial rotators are still active).
Loss of skin sensation from lateral aspect of arm
•Suprascapular nerve:
Supraspinatus and infraspinatus paralysis results in an inability to
laterally rotate and abduct. When at rest, supraspinatus &
infraspinatus paralysis results in the arm being medial rotated
(medial rotators are still active).
25.
BRACHIAL PLEXUS: UPPERTRUNK INJURY
Musculocutaneous nerve:
• Biceps brachii, brachialis, and coracobrachialis paralysis results in an inability
to flex the elbow and weakened supination of the forearm. When at rest,
paralysis of these muscles results in a pronated forearm with the elbow
extended (pronators are still active).
•Loss of skin sensation from lateral aspect of forearm
Radial nerve (C5-T1):
Due to C5 and C6 contributing to the radial nerve, and being the primary
innervation of extensor carpi radialis longus, weakened extension at the wrist
also occurs, which causes the resting position of the wrist to be flexed. In some
situations, C7 can also be involved, which will further weaken wrist extension
and elbow extension.
26.
BRACHIAL PLEXUS: LOWERTRUNK INJURY
Injury to nerve roots C8 and T1, or where they combine to form the lower
trunk, is called Klumpke’s paralysis. Injury to only the inferior trunk of the
brachial plexus is rare. Klumpke’s paralysis can be caused by violent
hyperabduction of the arm, as when a person is grasping an object to
prevent a fall. It can also be caused by a difficult breech delivery, or by
pressure on the lower trunk by a cervical rib.
• The ulnar nerve and median nerves are the
primary nerves involved in an injury to the
lower trunk of the brachial plexus.
• Most importantly, all the intrinsic hand muscles
are affected in Klumpke’s paralysis.
• The hand is held in a position known as “total”
claw hand, which is when all of the fingers are
in flexion when the hand is at rest. Don’t
confuse “total” claw hand” with “ulnar nerve”
claw hand in which only digits 4 and 5 are in a
flexed position at rest.
27.
BRACHIAL PLEXUS: LOWERTRUNK INJURY
Total claw hand results from the following situation:
• Wrist is slightly extended: loss of some opposition of wrist flexors (total loss of
flexor carpi ulnaris and flexor digitorum profundus, so active flexion of the wrist
will be weak)
• MP joints extended: loss of opposed flexion from lumbricals and interossei
• Flexion of IP joints: loss of opposed extension from lumbricals and interossei
(flexion of of IP joints results from flexor digitorum superficialis still being active
due to receiving innervation from C7)
• At rest, the thumb will retreat posteriorly into the same plane as the fingers.
This due to the loss of innervation to the thenar muscles. This position is
described as “ape hand”.
In addition to claw hand, the following signs will
be present.
• The forearm is supinated due to paralysis of
pronator quadratus.
• Loss of skin sensation from the medial
aspect of the arm, forearm and ulnar
sensory domain of the hand.
28.
Spinal
Segme
nt
Dermatomes Myotomes ReflexTests
C5 Lateral arm Shoulder abduction
Biceps brachii reflex
(anterior arm near ante-
cubital fossa).
C6
Lateral forearm,
thumb, index
finger
Elbow flexion or wrist
extension
Brachioradialis reflex
(lateral aspect of
forearm).
C7
Posterior
forearm, middle
finger
Elbow extension or
wrist flexion
Triceps brachii reflex (at
insertion of triceps
brachii).
C8
Medial forearm,
ring and little
Grip strength, shake
30.
PERIPHERAL NERVE TEST
NerveType Function
Axillary Nerve
Sensory Lateral arm
Motor Shoulder abduction
Musculocutaneous
Nerve
Sensory Anterior arm
Motor Elbow flexion
Radial Nerve
Sensory 1st Dorsal web space
Motor Wrist extension and thumb
extension
Median Nerve
Sensory Pad of Index finger,
Motor Thumb pinch and abduction
Ulnar Nerve
Sensory Pad of little finger
Motor Finger abduction
31.
MR BRACHIAL PLEXUS- PROTOCOL
Coronal 3D STIR (include both shoulders) FOV - 350.
Coronal MIP FOV- 350mm.
Coronal T1 (include both shoulders) FOV - 320mm.
Axial STIR (C5 to inferior axilla, single-side) FOV -200mm.
Axial T1 (single-side) FOV - 200mm.
Sagittal T2 (C-spine to midpoint of arm) FOV - 240mm.
Oblique sagittal T1/T2/STIR
MR neurography
Contrast if required
32.
MR BRACHIAL PLEXUS- SPECIFIC SEQUENCE
Intravenous Gadolinium:
Administered in patients with tumors or mass lesion
Not administered in patients with traumatic brachial plexopathy.
Traumatic brachial plexus injury:
Sagittal T2- weighted images are obtained through the cervical
spine followed by axial T2- weighted images from C4 to T2 levels.
3D gradient echo (GRE) sequence with thin slices – to look for the
nerve root avulsion.
Thoracic outlet syndrome- sagittal T1-weighted image are obtained
through the symptomatic side extending from midline to the axilla with
arm in hyper abducted position.
These are compared with similar sagittal T1-weighted images
obtained with arm in neutral position by the side of body.
H/O road trafficaccident few days back.
Clinical Presentation:
Intense pain in the right arm and shoulder, with edema.
Decreased sensitivity and incapacity to move wrist and fingers.
Shoulder and arm radiographs was normal.
36.
CT findings includean
epidural and/or paravertebral
fluid collection, which can be
associated with vertebral
fracture, and, if chronic, can
be associated with osseous
remodeling and foraminal
widening.
MRI will show a fluid collection, epidural
and/or paravertebral, well-delineated,
with the epidural fat providing a natural
contrast to the extent of the collection.
The collection is lacking of neural
elements, is hypointense on T1,
hyperintense on T2 and STIR, with no
enhancement afterT1 contrast.
Key Diagnostic
Features:
Fast-spin-echo T2-
weighted sequence can be
helpful to define dural
margin and presence or
absence of nerve roots,
which are absent in cases
of nerve root avulsion.
POSTTRAUMATIC PSEUDOMENINGOCELE ANDNERVE ROOT
AVULSION
• Absence of rootlets/roots
• Spinal cord signal intensity
• Pseudomeningocele: leakage of fluid through a meningeal tear
highly indicative but not pathognomonic
23% root avulsion don't have puseudomeningocele and
pseudomeningocele like lesions are seen in 24% cases without
root avulsion
Denervation of ipsilateral paraspinal muscles (supplied by dorsal
branch of spinal nerve)
40.
POSTTRAUMATIC PSEUDOMENINGOCELE ANDNERVE ROOT
AVULSION
Background: A pseudomeningocele is an abnormal perivertebral
circumscribed fluid collection of CSF, which communicates through the
neural foramen or through a vertebral defect, associated with dural tear
after spinal surgery (durotomy) or nerve root avulsion and tear of nerve
root sleeve during spinal trauma. Most adult brachial plexus injuries are
posttraumatic, caused by traction in situations of high-energy forces
(abduction or downward displacement of the arm), with avulsion of one
or more nerve roots from spinal cord. Nerve root avulsion is classified as
preganglionic(lesion central to dorsal root ganglion) or postganglionic
(injury peripheral to ganglion). The most common signs/symptoms are
localized soft tissue swelling, pain, and paralysis of ipsilateral limb.
41.
Axial T2 fatsat
Post-traumatic multiple right brachial plexus(C6 down to D2) pseudo-meningoceles resulting from
their related nerve root avulsions. Acute denervation changes of the right shoulder girdle
musculature.
Coronal STIR
Coronal T1 Coronal T2
Axial T2
TREATMENT
Injury levelis critical to treatment planning and prognosis,
because the integrity of nerve roots is key for surgical decision.
Preganglionic avulsions are normally not feasible to repair
surgically, and thus have a worse prognosis.
Postganglionic avulsions are surgically managed, with excision of
damaged segment and nerve autograft between nerve ends, and
have a better prognosis.
In the patient with preganglionic avulsions and
pseudomeningocele, a conversative approach was followed with
medical treatment of symptoms, physiotherapy, and small
improvement.
INTERSCALENE TRIANGLE
Thenerve roots and the subclavian artery enter the
interscalene triangle.
It is formed by the anterior scalene and middle scalene muscles.
Just lateral of the interscalene triangle the three trunks are
formed
Interscalene Triangle Identification of Trunks
47.
INTERSCALENE FAT PAD
Importance:
The earliest sign of extra-thoracic and brachial plexus involvement is
invasion of the interscalene fat pad by tumor.
This fat pad lies between the anterior and the middle posterior
scalene muscles and cephalad to the lung apex.
The trunks of the brachial plexus
are found in this fat pad.
In advanced disease there is
direct extension and invasion of
the brachial plexus, intercostal
nerves, stellate ganglion,
neighboring ribs, and vertebrae.
48.
IDENTIFICATION OF ROOTS
The brachial plexus is predominantly formed by the
ventral rami of the spinal nerves of C5 through T1.
They exit the neural exit foramina and form the
roots.
On the sagittal images the proximal part of the first
rib issued to identify the C8 and T1 nerve roots, with
C8 above and T1 below the first rib.
Identification of Roots
Interscalene triangle: medial
aspect
Subclavian artery : C5 to C7 superior and C8, T1
posterior
49.
IDENTIFICATION OF TRUNKS
Justlateral to the interscalene triangle the three trunks are formed, the superior (ST), the
middle (MT) and inferior trunk (IT).
3 in number
Supraclavicular region, between anterior and middle scalene muscles
Landmark: lateral scalene triangle
50.
IDENTIFICATION OF TRUNKS
Justlateral to the interscalene triangle the three trunks are formed, the superior (ST), the middle (MT) and inferior trunk (IT).
3 in number
Supraclavicular region, between anterior and middle
scalene muscles
Landmark: lateral scalene triangle
Interscalene triangle: lateral aspect
Subclavian artery: upper, middle are superior
and lower is posterior
51.
IDENTIFICATION OF DIVISIONS
The divisions are located at the level where the branch plexus crosses the clavicle.
The cords are positioned above and around the axillary artery and they are named
after their position relative to the axillary artery.
On sagittal MRI images the lateral cord is located most anterior, the posterior cord
most superior and the medial cord most posterior.
6 in number
Lateral to scalene muscles
Landmark : lateral border of first rib and retroclavicular
PERIPHERAL NERVES
5terminal branches
Landmark: based on quadrants
Before this posterior cord gives off axillary nerve
Anterior superior – Median
Posterior superior – Musculocutaneous
Posterior inferior -Radial
Anterior inferior - Ulnar
54.
CLASSIFICATION OF BRACHIALPLEXUS PATHOLOGIES
Brachial Plexus -
Pathologies
Traumatic Non-Traumatic
a. Infective
b. Inflammatory
c. Neoplasm
d. Radiation
e. Vascular
f. Extrinsic compression
Nerve continuity Grade of injury
Continuous Discontinuous
Sunderland
classification
55.
TRAUMATIC BRACHIAL PLEXOPATHY
Thereare two distinctive populations affected by traumatic brachial
plexopathy.
Neonates sustain a traction injury due to shoulder dystocia during
vaginal delivery.
The second population is young men in the second and third decades –
- fall from a height
- motorcycle or motor vehicle crash
- penetrating injury from a gunshot
56.
Neurapraxia
Sunderland -
Grade I
endoneurium
myelinsheath injured - conduction block
increased T2/STIR signal in the nerve,
muscle appears normal
Axonotmesis
Sunderland - Grade
II/III axonal disruption with
intact endoneurium,
perineurium and
epineurium
thickened, T2/STIR hyperintense nerve with
denervation edema in muscles
myelin sheath epineurium
perineurium
axon
axonal and
endoneurial disruption
with intact perineurium
and epineurium
perineurium
endoneurium epineurium
57.
Axonotmesis with neuromain
continuity
Sunderland - Grade IV
epineurium
axonal, endoneurial and perineurial disruption with
disruption of nerve fascicles but intact epineurium
thickened, T2/STIR hyperintense nerve with focal
enlargement, denervation edema in muscles
Neurotmesis
Sunderland - Grade
complete disruption of continuity of nerve
disruption of continuity of nerve, muscle shows
denervation edema and undergoes atrophy with time
58.
SEDDON-SUNDERLAND CLASSIFICATION OFNERVE INJURIE
Seddon Sunderland
class Injury Recovery prognosis Treatment
indicated
Neuropraxia
(Compression
)
I
Neuropraxia: localized and reversible conduction
blockade
Complete No
Axonotmesis
(crush)
II
Axonotmesis: axonal disruption Complete No
III Axonotmesis: axonal and endoneurial sheath
disruption
Incomplete,
Wallerian degeneration
Medication
IV Axonotmesis: axonal, endoneurial sheath, and
perineurial sheath disruption
Wallerian degeneration,
incomplete
Surgical
V Neurotmesis: axonal, endoneurial sheath, and
perineurial sheath, and epineurial sheath disruption
Wallerian degeneration,
incomplete Surgical
Neurotmesis
(transection)
VI Combination of the above injuries Incomplete,
unpredictable
Surgical
60.
BRACHIAL PLEXUS NEURITIS
•Acute brachial plexitis presents with shoulder and upper arm pain
lasting for few days to weeks followed by upper arm weakness.
• Idiopathic brachial neuritis is of unknown cause but an immune-
mediated inflammatory reaction.
• Probable etiologies – viral
infection, vaccination, surgery
61.
CLASSIFICATION OF NEONATALBRACHIAL PLEXUS INJURY
Superior Nerve Injury Inferior Nerve Injury
Extra foraminal Intra foraminal
Well-developed investing fascia
protects the upper nerve roots
from proximal traction
Partial or complete avulsion of the
nerve root.
62.
OBSTETRICS BRACHIAL PALSY-NARAKA’S CLASSIFICATION
Types
Common
terminology
Nerve/Root
deficits
Deformity involved
Type-I Erb’s palsy C5–C6
Shoulder Adduction, Shoulder
internal rotation,
Elbow extension and forearm pronation
(Erb’s posture)
Type-II
Extended Erb’s
palsy
C5–C7(or C5–C8)
Erb’s posture with wrist flexion
(“waiters tip”)
Type-III
Pan plexus without
Horner syndrome
C5–T1 Flail arm
Type-IV
Pan plexus with
Horner syndrome
C5–T1 and
sympathetic
chain
Flail arm with Horner syndrome
Type-v Klumpke C8–T1 Paralyzed hand
Ref: https://www.researchgate.net/publication/355889284_Current_Management_Strategies_in_Neonatal_Brachial_Plexus_Palsy
63.
NEOPLASM
Four typesof neurogenic tumors of the brachial plexus
- Schwannoma
- Neurofibroma
- Plexiform neurofibroma
- Malignant Peripheral Nerve Sheath Tumor (MPNST).
Fig.1. Sagittal viewfrom T2-weighted
magnetic resonance imaging of the
patient's cervical spine shows cystic
lesions with high signal intensity,
extending from the seventh cervical
vertebra to the first thoracic vertebra.
Fig. 2. Axial view from T2-weighted magnetic resonance imaging
of the patient's cervical spine (Fig-2A) shows cystic lesions with
high signal intensity in the neural foramen of the seventh cervical
vertebra. Axial view from T1-weighted magnetic resonance
imaging of the patient's cervical spine (Fig-2B) shows cystic lesions
with low signal intensity, extending from the seventh cervical
vertebra to the first thoracic vertebra.
OTHER TUMORS OFBRACHIAL PLEXUS
• Can be benign or malignant soft tissue tumors, bone tumors or
metastatic disease.
• The most common benign soft tissue tumors is lipoma followed
by aggressive fibromatosis.
• Malignant soft tissue tumors.
70.
METASTATIC TUMOURS
• Breastcarcinoma - most common source of metastatic disease
causing brachial plexopathy.
• Other metastatic sources include lung carcinoma and head and
neck cancers.
• Metastatic lymphadenopathy - surround the neurovascular
bundle, resulting in vascular or neural compromise.
• Metastatic disease from all causes - T1 hypointense and T2
heterogeneously hyperintense lesion.
71.
SUPERIOR SULCUS TUMOR
Alsoknown as Pancoast tumor.
Non-small cell lung carcinomas that arise from the lung apex and
invade the thoracic inlet.
Tumor infiltration of the stellate ganglion causes Horner’s
syndrome, which is characterized by miosis, ptosis and anhydrosis.
Pancoast's syndrome –
- Pain in the shoulder and arm
- Weakness and atrophy of the muscles of the hand
- Horner's syndrome.
72.
PANCOAST TUMOR -IMAGING
MRI useful to assess the extension of tumors towards brachial
plexus, vertebral bodies, intervertebral foramina and the
subclavian vessels.
Infection may radiographically mimic a malignant superior
sulcus tumor Especially Nocardia is known to invade the thoracic
wall.
Contra-indications for surgery:
Brachial plexus involvement above C8.
Vertebral body invasion of more than 50%
Extensive mediastinal involvement with invasion of
oesophagus or trachea.
73.
INTERSCALENE TRIANGLE -INVASION
• Pancoast tumours will be involving the interscalene triangle (middle
compartment).
• Connective-tissue sheath, covering the brachial plexus will initially
displace the nerve roots or trunks superiorly without actually
invading them.
• Sensory dysfunction may occur because of extrinsic
74.
SONOGRAPHY OF BRACHIALPLEXUS
Uses-
• Entrapment neuropathies due to- Cervical rib, elongated C7
transverse process.
• Nerve tumors from brachial plexus.
• Guiding interventions (i.e., biopsy & brachial plexus anesthesia).
• Can detect root avulsion, nerve injury in form of a neuroma, and
scar tissue formation.
75.
THORACIC OUTLET SYNDROME
•Dynamically induced compression of neural and/or arterial
structures crossing the cervicothoracobrachial junction.
• The three spaces that are evaluated on sagittal T1-weighted
images are-
Interscalene triangle-
Costoclavicular region-
Retro-pectoralis minor spaces.
• MRI - important role in,
Demonstrating neurovascular compression.
Localizing the cause of compression.
Identifying the structure causing the compression.
76.
CAUSES OF THORACICOUTLET SYNDROME
• The costoclavicular space is the most common site of compression
followed by interscalene triangle.
• The lesions causing compression may be-
Bony abnormalities (cervical rib, long transverse process of
C7vertebra, callus or osteochondroma of clavicle or first rib)
Soft tissue pathologies (fibrous band, hypertrophy of scalenus
anterior muscle, scalenus minimus muscle, and fibrous
scarring).
• Contrast-enhanced MR angiography may be performed with the
arm in elevated position to demonstrate narrowing of subclavian
artery.
77.
MR NEUROGRAPHY
MR neurography,also known as peripheral nerve MRI, uses high-resolution
techniques to visualize nerves throughout the body. A radiologist who
specializes in nerve imaging reviews the images to detect abnormal
features of the nerve that may indicate injury or inflammation, such as
increased brightness or size. By localizing and characterizing nerve
abnormalities, MR neurography aids in the diagnosis and management of
various conditions.
Specially trained HSS
radiologists work closely with
referring physicians to
determine the appropriate
imaging exams for diagnosis
and treatment planning.
MR neurography of the bilateral brachial plexus in a patient with
Parsonage-Turner syndrome demonstrates constrictions (blue arrows) of
both suprascapular nerves.
78.
MR CHARACTERISTICS OFNORMAL PERIPHERAL NERVES
Morphology
Generally similar caliber to adjacent arteries and gradually
tapers distally
Smooth contour and course
Surrounded by perineural fat
Fascicular pattern visible on both T1 and t2 weighted images,
provided the nerve is large enough for this to be discernable·
Signal intensity
Isointense to skeletal muscle on
Isointense to slightly hyperintense on STIR and T2 fat-saturated
images
Enhancement is absent except in specific regions with permeable
blood nerve barrier (e.g. dorsal nerve root ganglion)
79.
CLINICAL APPLICATIONS
Trauma:MRN is particularly useful in evaluating brachial plexus injuries
resulting from trauma, such as those from motor vehicle accidents or
sports injuries.
Tumors: It can help detect and characterize tumors affecting the
brachial plexus, guiding treatment strategies.
Inflammation: MRN can help diagnose inflammatory conditions
affecting the brachial plexus, such as brachial plexitis.
Pre-operative planning: MRN aids in surgical planning by providing
detailed anatomical information and delineating the extent of nerve
involvement.
Post-operative evaluation: It can be used to assess the effectiveness
of treatment or identify persistent surgery.
80.
INDICATIONS OF MRNEUROGRAPHY
Brachial plexus injury or lumbosacral
plexopathy
Traumatic nerve injury
Parsonage-turner syndrome (PTS), also known
as neuralgic amyotrophy
Anterior and posterior interosseous neuropathy
Spinal accessory neuropathy
Thoracic outlet syndrome
Sciatica and piriformis syndrome
Idiopathic neuropathy
Nerve entrapment, including:
Carpal tunnel syndrome (median nerve)
Cubital tunnel syndrome (ulnar nerve)
Tarsal tunnel syndrome (tibial/plantar nerves)
Meralgia paresthetica (lat. femoral cutaneous
nerve)
Drop foot
Nerve injury around metallic hardware
Peripheral nerve sheath tumors (schwannoma
and neurofibroma)
Pudendal neuralgia
Charcot-marie-tooth disease
Chronic inflammatory demyelinating
polyneuropathy (CIDP)
Multifocal motor neuropathy/MADSAM
Occipital neuralgia
Facial nerve palsy/bell’s palsy
Trigeminal neuralgia
MR neurography can be used to diagnose many traumatic and
atraumatic conditions that cause nerve compression, entrapment, or
disruption:
81.
MR neurography showinga tumor (yellow arrowheads)
arising from the ulnar nerve (blue arrows) in the forearm.
MR neurography images of a healthy ulnar nerve
(top row) and an entrapped ulnar nerve in cubital
tunnel syndrome (bottom row). The abnormal signal
hyperintensity (brightness) of the nerve indicates
neuropathy, with the nerve enlarged as it courses
through the cubital tunnel at the elbow.
82.
Advantages:
MRN providesdetailed visualization of the brachial plexus and surrounding structures.
It can be more sensitive than conventional MRI in detecting subtle nerve abnormalities.
It can help differentiate between various causes of brachial plexopathy.
It can be used to monitor the progression or resolution of brachial plexus lesions.
Limitations:
MRN requires specialized hardware and software.
It can be time-consuming, with imaging sessions potentially lasting 30-45minutes.
The image quality and diagnostic accuracy can be affected by patient movement
and the size of the nerve trunk.
83.
ROLE OF DIFFUSIONTENSOR IMAGING (DTI)
DTI is a specialized MRN technique that provides information about
nerve fiber orientation and integrity, which is useful in research
settings and may play a larger role in clinical practice.
84.
CONCLUSION
• Brachial plexushas a complex anatomy and long course.
• Various traumatic and non-traumatic pathologies affecting it can
be evaluated optimally by MRI.
• Knowledge of the anatomy and proper planning of the scan are
essential for complete evaluation of the brachial plexus.
















































































![Radiologic_Anatomy_of_the_Brachial_plexus [final].pptx](https://image.slidesharecdn.com/radiologicanatomyofthebrachialplexusfinal-250811175545-691d20d9/75/Radiologic_Anatomy_of_the_Brachial_plexus-final-pptx-85-2048.jpg)



































































