Case scenario:
Mrs. Nasima,a 31-year-old, homemaker who came to the gynae opd and presents
with a history of secondary infertility. She underwent bilateral ovarian cystectomy 5
months back for having chocolate cysts. She and her husband have been
attempting to conceive their second child for the past 2 years without success. She
reports a shorter menstrual cycles every 20-25 days with moderate lower
abdominal pain during her cycle. Her past obstetric history includes a single
uncomplicated pregnancy and vaginal delivery 09 years back.
Endometrioma also knownas chocolate cysts or endometriotic cysts, are a
localized form of endometriosis and are usually within the ovary. They are readily
diagnosed on ultrasound, with most demonstrating classical radiographic
features.
Epidemiology
These occur in up to 10% of women of reproductive age.
7.
Endometriomas are cysticlesions that stem from endometriosis. Endometriosis is
a common, estrogen-dependent, inflammatory, gynecologic disease process in
which functional endometrial tissue is abnormally present outside the uterine
cavity.
8.
Approximately 17 to44% of women diagnosed with endometriosis will experience
an endometrioma. These lesions are commonly referred to as “chocolate cysts” due
to the dark brown, old blood that accumulates within them, resembling “melted
chocolate”. Endometriomas indicate a more severe disease state in patients with
endometriosis and can lead to specific issues, such as decreased ovarian reserve.
The cysts may be up to 20 cm in size although they are usually smaller (2-5 cm).
9.
Etiology
Endometriomas are
most commonly
thoughtto be caused
when the seeding of
ectopic endometrial
tissue occurs, most
often on the ovary,
bleeds, causing a
hematoma.
This typically occurs with
the natural menstrual
cycle of a woman because
the ectopic endometrial
tissue is still hormonally
active.
Therefore, this tissue
will naturally shed with
the withdrawal of
progesterone after the
breakdown of the
corpus luteum.
10.
Pathology
Although the pathogenesisis still under discussion, three theories have emerged:
1. Metaplastic transformation of the peritoneal epithelium into functional
endometrium.
2. Peritoneal seeding due to retrograde menstruation.
3. Activation of mesenchymal cells differentiation caused by endometrium in the
peritoneal cavity from retrograde flow.
General risk factorsfor the development of endometrioma
include:
1. Nulliparity.
2. Early menarche (typically before 11 to 13 years old).
3. Late menopause, short menstrual cycles (less than 27 days).
4. Heavy menstrual bleeding.
5. Mullerian anomalies that stops blood from flowing normally during period.
6. Low body mass index (BMI).
7. Exposure to diethylstilbestrol in utero.
8. Have a close relative (for example: parent, sibling, or aunt) with endometriosis.
13.
Clinical presentation
The symptomsdo not necessarily correlate with disease severity and include
1. Pelvic pain (nearly 71-87% of women),
2. Dysmenorrhea,
3. Dyspareunia,
4. Infertility in 20-50% of patients,
5. Irregular periods,
6. Unusual or heavy bleeding during periods.
14.
Diagnosis of chocolatecyst:
• Step 1: Medical History
• Step 2: Physical Examination
• Step 3: Imaging and Tests
• Step 4: Laparoscopy
15.
Ultrasound
The appearances ofendometriomas can be quite variable. The classical example is an avascular
unilocular cyst containing low-level, homogeneous "ground-glass" like internal echoes, as a result of the
hemorrhagic debris. This appearance occurs in 50% of cases.
fig: USG showing homogenous ground glass appearance in endometrioma.
Fig: Homogenous lowlevel internal echoes with no internal flow at doppler. Fig: Ground glass like echoes.
19.
MRI
•T1
• Typically, lesionsappear hyperintense while acute hemorrhage occasionally appears hypointense.
• Endometriomas with high T1 signal characteristically do not show loss of signal on T1 fat-suppressed sequences, which is
important for differentiating it from a mature cystic teratoma of the ovary.
Fig: axial T1WI Fig: Sagittal T1WI
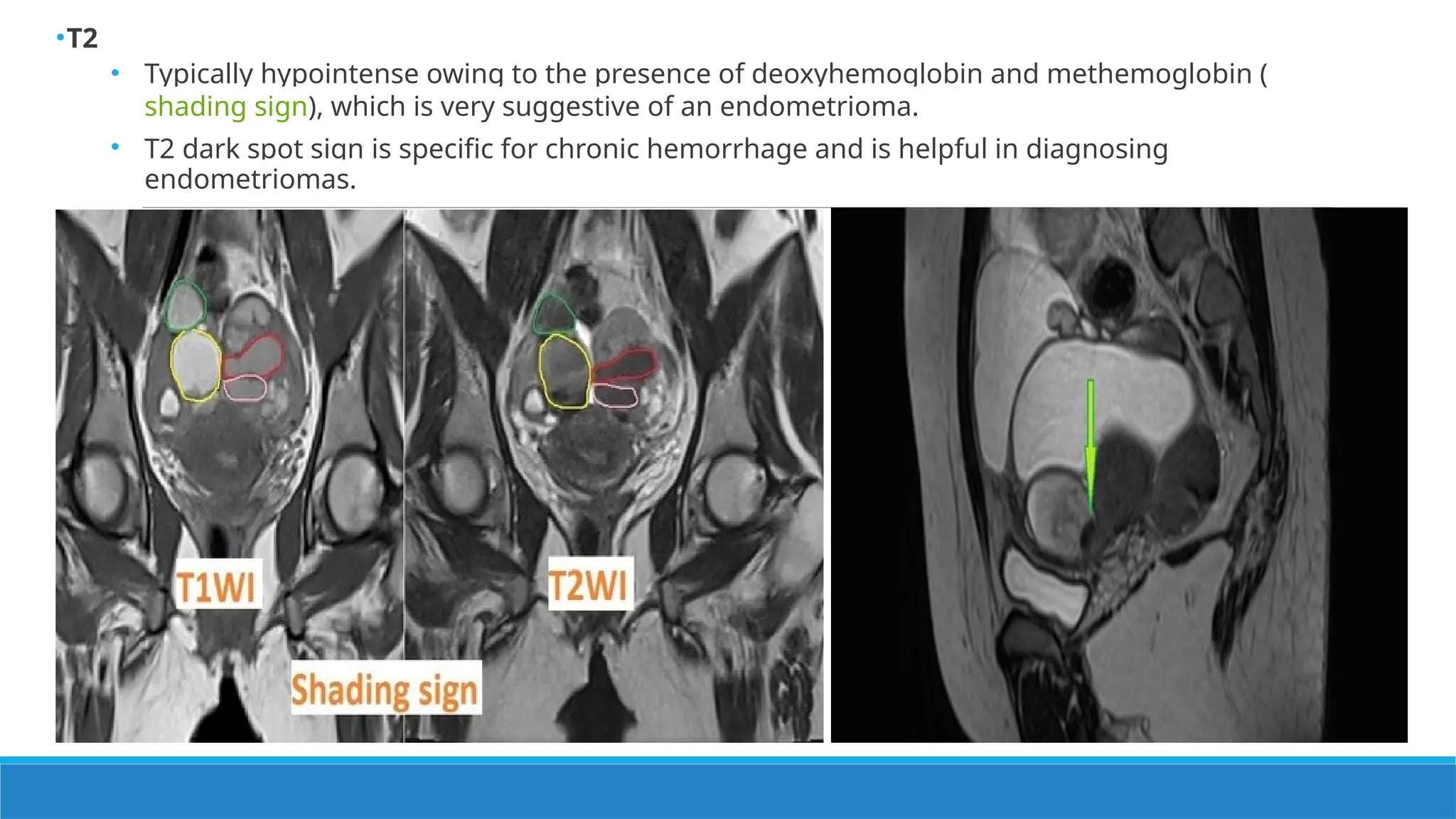
•T2
• Typically hypointenseowing to the presence of deoxyhemoglobin and methemoglobin (
shading sign), which is very suggestive of an endometrioma.
• T2 dark spot sign is specific for chronic hemorrhage and is helpful in diagnosing
endometriomas.
Plain radiograph:
Not usuallyhelpful in diagnosis. ~10% of endometriomas can calcify.
Computed Tomography:
Endometriomas on CT tend to be complex pelvic cystic masses often with increased
attenuation components representing hemorrhage. These appearances are non-
specific.
25.
Laboratory evaluations thatcan be considered for these patients
include :
• Complete blood count (CBC),
• Cancer antigen (CA)-125,
• Urinalysis and
• Sexually transmitted infection (STI) testing
Types of lesionsEndometrioma Hemorrhagic ovarian
cyst
Dermoid
Clinical features Chronic pelvic pain,
Infertility
Sudden onset and
recurrent lower
abdominal pain.
Fullness in the lower
abdomen.
USG Findings Cystic lesion with low
level internal echoes.
Cystic lesion with
multiple septation
creating fishnet
appearance.
Cystic lesion containing
heterogenous echoes
with posterior acoustic
shadowing.
MRI findings T1 hyperintense
T2 hypointense with
shading sign and T2
dark spot sign.
brighter on T2-
weighted images &
absence of the
"shading sign.
will show fat
suppression on MRI
fat-suppressed
sequences.
Complications
• Chronic pelvicpain.
• Infertility.
• If the endometrioma is 6 cm or large, this puts the patient at increased risk for
ovarian torsion, which is a surgical emergency and can lead to loss of the ovary.
•Endometriomas have the potential to decidualise during pregnancy resulting in the
formation of vascularized, papillary projections and these changes give an
appearance mimicking malignancy thus careful follow-up imaging is
recommended.
•Endometriomas carry a small risk of upgrading to malignancy.
31.
Treatment
Expectant management maybe adopted in the younger asymptomatic patients and
adolescents provided that malignancy can be excluded.
Drugs used For medical management:
•GnRH agonists,
•Combined oral contraceptive,
•Progestin and
•Analgesics.
32.
Surgery is indicatedwhen
• An endometrioma persists and is greater than > 4 cm.
• Severe chronic pelvic pain.
• Infertility.
If not surgically excised, follow-up should be at least yearly.
33.
Prognosis
• Endometriomas areusually benign entities, there is an ~1% rate of malignant
transformation. Malignant transformation is uncommon in masses <6 cm.
• Patients with endometriomas signify those with more severe disease and thus can
have more long-term complications from the disease. Even if treatment is effective
for patients for a time, it is, unfortunately, a condition with a high level of
reoccurrence.
34.
The takeaway
1. Chocolatecysts are a subgroup of endometriosis.
2. The presence of endometriomas indicates a more severe stage of
endometriosis.
3. Endometriomas can lead to chronic pelvic pain and infertility and often require
surgery for treatment.
4. When initially evaluating these patients, most often, a pelvic ultrasound is
performed. It is crucial when looking at any adnexal masses to describe them
appropriately.
35.
References
• Textbook ofRadiology and Imaging by David Sutton (eighth edition)
• DC Dutta’s textbook of Gynecology.
• Different journals, articles.
• Radiopaedia.

















































































![Radiologic_Anatomy_of_the_Brachial_plexus [final].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicanatomyofthebrachialplexusfinal-250811175545-691d20d9-thumbnail.jpg?width=640&height=640&fit=bounds)




















