



![Marc Imhotep Cray, M.D.
Rifampin
Adverse Effects:
flu-like syndrome
hepatotoxicity [(hepatitis; elevated liver function tests (LFTs)]
drug-drug interactions (cytochrome P-450 inducer)
proteinuria
thrombocytopenia
red-orange discoloration of tears, sweat, urine and stool
o Contact lenses can be permanently stained with this orange
discoloration
o This side effect can be a source of great concern to individuals who
are not warned of its possibility](https://image.slidesharecdn.com/pulmonary-tuberculosis-pharmacology-160214082712/85/Pulmonary-tuberculosis-pharmacology-20-320.jpg)

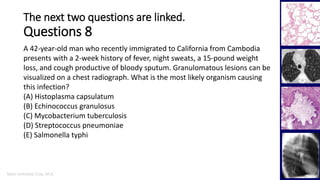
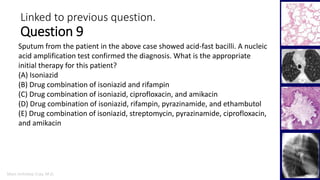
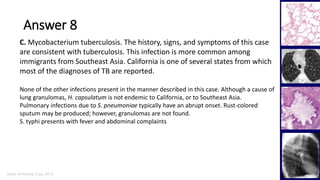
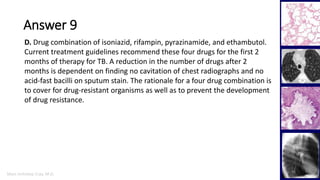


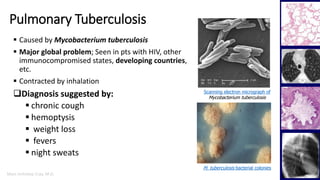
A 42-year-old HIV-positive man presents with symptoms of hemoptysis, weight loss, fever, cough, and chills. Imaging and testing reveal a lung lesion and acid-fast bacilli in a sputum sample, indicating pulmonary tuberculosis. The patient is not taking his HIV medications and has a low CD4 count, placing him at high risk. He is admitted to isolation and started on multidrug TB treatment while drug susceptibility testing is performed.