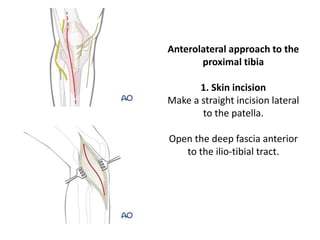
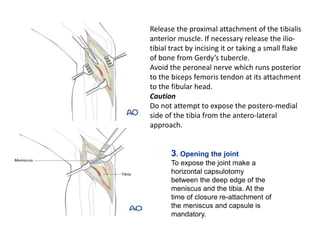
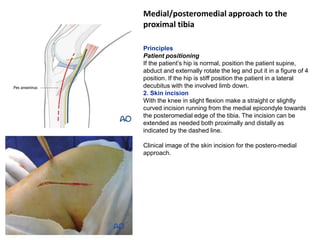
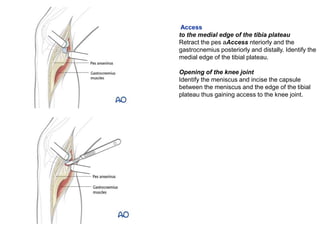
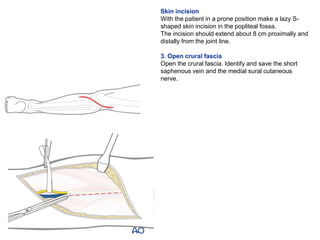
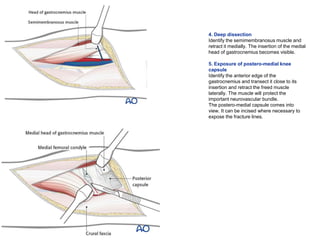
The document describes three approaches to the proximal tibia - anterolateral, medial/posteromedial, and posterior. The anterolateral approach involves a straight incision lateral to the patella to expose the joint and tibia. The medial/posteromedial approach uses a straight or curved incision from the medial epicondyle to expose the pes anserinus, medial edge of the tibia plateau, and knee joint. The posterior approach uses a lazy S-shaped incision in the prone patient to expose the postero-medial knee capsule and treat fractures by incising the capsule.