Downloaded 48 times




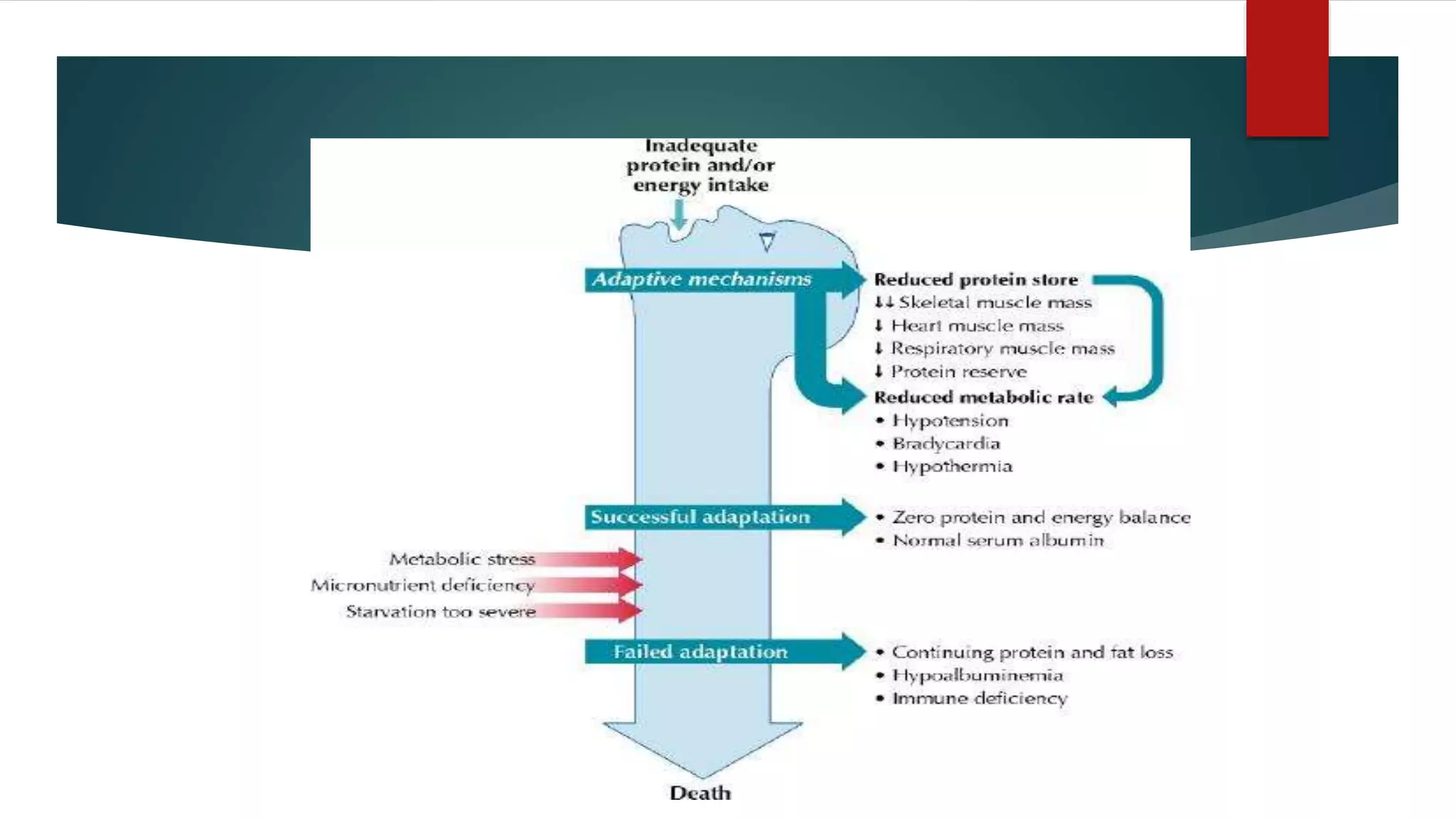















Protein calorie malnutrition (PCM) is a nutritional disorder primarily manifesting as protein-energy malnutrition (PEM), which includes conditions like kwashiorkor and marasmus, largely affecting children in low-income and developing areas. Key causes of PCM are inadequate nutrient intake due to economic, social, and environmental factors, leading to severe health issues such as growth retardation, immune dysfunction, and high mortality rates. Prevention and treatment focus on promoting breastfeeding, improving dietary practices, and providing essential vitamins and minerals, alongside addressing underlying health issues.