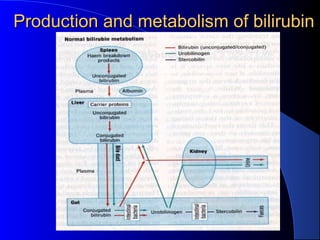
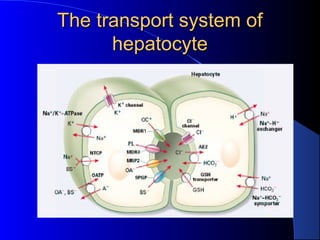
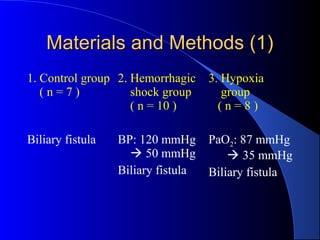
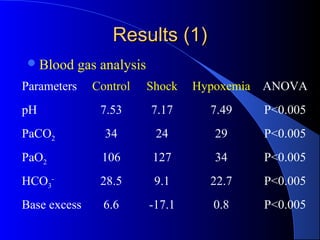
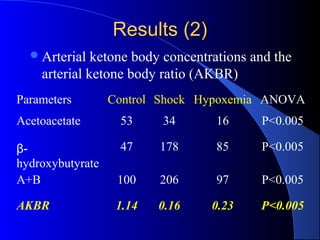
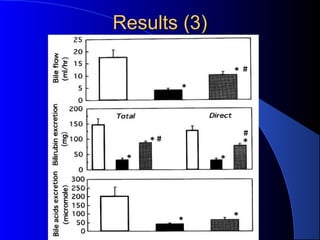
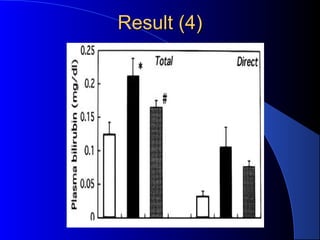
This document discusses a case of a 60-year-old male patient presenting with septic shock and predominantly conjugated hyperbilirubinemia without elevated liver enzymes. It then reviews the production, transport, and causes of conjugated hyperbilirubinemia, both intrahepatic and extrahepatic. The document also summarizes a study showing that hemorrhagic shock and hypoxemia can decrease hepatic energy status and impair bilirubin excretion from hepatocytes into bile, potentially explaining post-traumatic jaundice.