This document discusses the evolution and effectiveness of light curing technologies in dentistry, including light sources like UV, QTH, LED, plasma arc, and laser, as well as their respective advantages and disadvantages. It highlights the importance of parameters such as power density in achieving effective polymerization, the history and improvements in curing methods over time, and reviews various studies comparing different curing techniques. The document also addresses the clinical implications of curing practices, emphasizing the need for optimal protocols to minimize polymerization stress and ensure successful restorations.



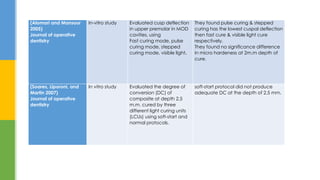

![ Alomari, Qasem D, and Yasar F Mansour. “Effect of LED Curing Modes on Cusp Deflection and Hardness of Composite Restorations.” Operative
Dentistry 30 (6): 684–89. http://www.ncbi.nlm.nih.gov/pubmed/16382590.
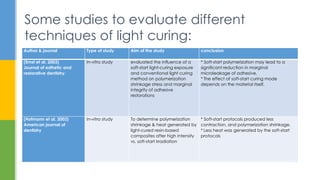
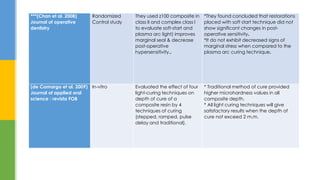
Chan, Daniel C N, W D Browning, K B Frazier, and M G Brackett. 2008. “Clinical Evaluation of the Soft-Start (pulse-Delay) Polymerization Technique in
Class I and II Composite Restorations.” Operative Dentistry 33 (3): 265–71. doi:10.2341/07-120.
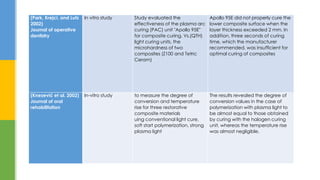
De Camargo, Ericson Janolio, Eduardo Moreschi, Wagner Baseggio, Jaime Aparecido Cury, and Renata Corrêa Pascotto. 2009. “Composite Depth
of Cure Using Four Polymerization Techniques.” Journal of Applied Oral Science : Revista FOB 17 (5): 446–50. doi:10.1590/S1678-77572009000500018.
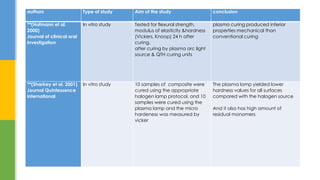
Ernst, Claus-Peter, Nicole Brand, Ulrike Frommator, Gerd Rippin, and Brita Willershausen. 2003. “Reduction of Polymerization Shrinkage Stress and
Marginal Microleakage Using Soft-Start Polymerization.” Journal of Esthetic and Restorative Dentistry : Official Publication of the American Academy
of Esthetic Dentistry ... [et Al.] 15 (2): 93–103; discussion 104. http://www.ncbi.nlm.nih.gov/pubmed/12762473.
Hofmann, Norbert, Tanja Markert, Burkard Hugo, and Bernd Klaiber. 2003. “Effect of High Intensity vs. Soft-Start Halogen Irradiation on Light-Cured
Resin-Based Composites. Part I. Temperature Rise and Polymerization Shrinkage.” American Journal of Dentistry 16 (6): 421–30.
http://www.ncbi.nlm.nih.gov/pubmed/15002959.
Hofmann, N, B Hugo, K Schubert, and B Klaiber. 2000. “Comparison between a Plasma Arc Light Source and Conventional Halogen Curing Units
Regarding Flexural Strength, Modulus, and Hardness of Photoactivated Resin Composites.” Clinical oral investigations 4(3): 140–47.
http://www.ncbi.nlm.nih.gov/pubmed/11000318 (April 24, 2015).
Refrences:](https://image.slidesharecdn.com/lightcure-150430185011-conversion-gate02/85/Light-cure-advanced-56-320.jpg)