Downloaded 14 times
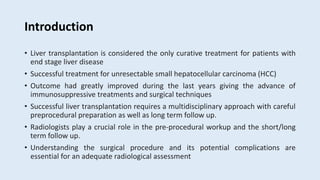
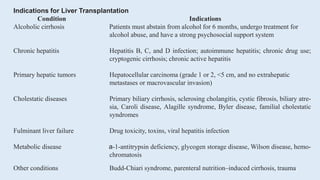







This document discusses imaging of the liver preoperatively for liver transplantation. Radiologists play a key role in evaluating patients' anatomy and suitability for transplantation. Preoperative imaging assesses liver parenchyma for tumors or other abnormalities, calculates liver volumes, and precisely maps the hepatic vasculature. Living donor liver transplantation requires imaging the donor's liver to ensure the safety of donation and adequate remnant liver volume. The document outlines various surgical techniques for cadaveric and living donor transplantation.














































































