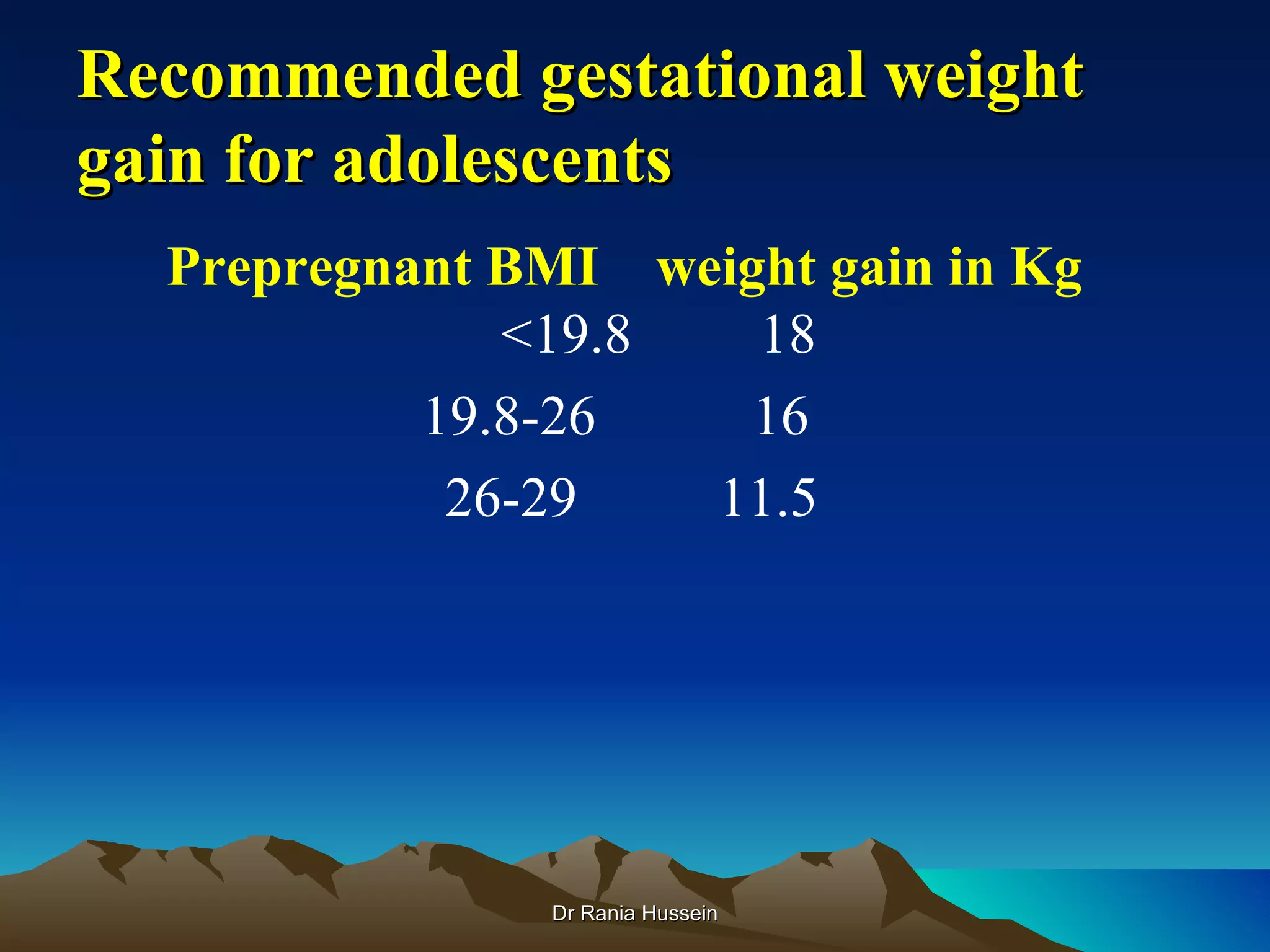
This document discusses gastrointestinal issues and nutrition in pregnancy. It covers common problems like nausea and vomiting, heartburn, constipation, as well as cravings and aversions. It provides treatment recommendations. It also discusses the benefits of and recommendations for exercise during pregnancy. Additionally, it covers high risk factors in pregnancy such as maternal age, obesity, diabetes, hypertension, and substance use. Throughout it emphasizes the importance of adequate nutrition and hydration for both maternal and fetal health.