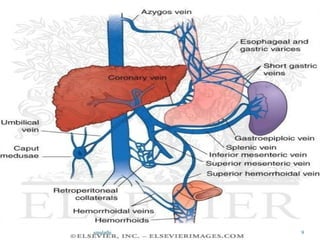
This document discusses portal hypertension (PH), including its definition, classification, pathophysiology, etiology, clinical features, complications, and diagnosis. Some key points:
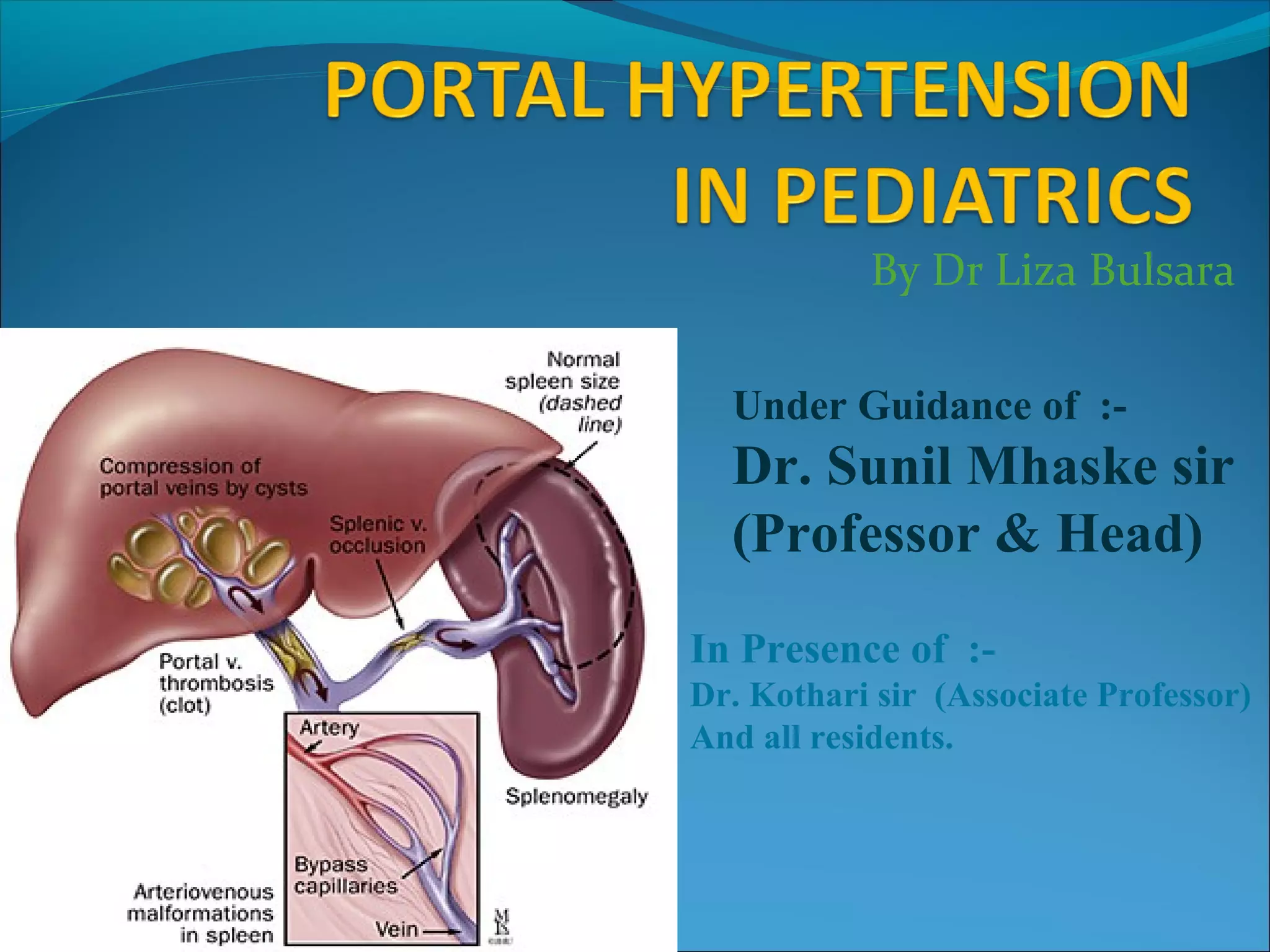
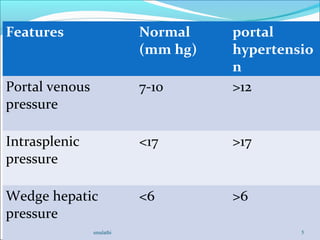
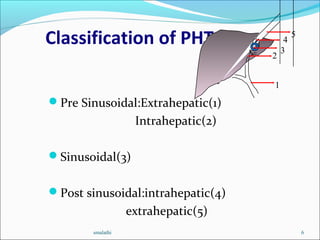
1. PH is defined as a portal venous pressure gradient above 10 mmHg. It can be pre-sinusoidal, sinusoidal, or post-sinusoidal based on location of blockage.
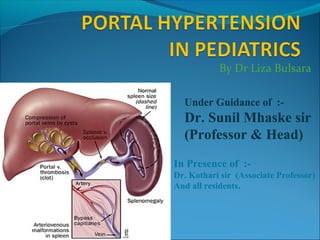
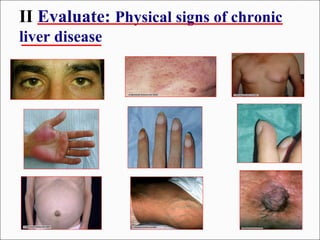
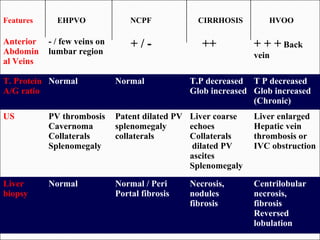
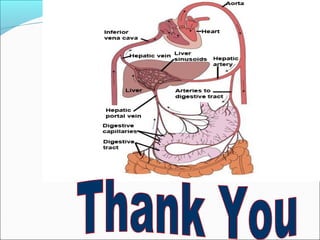
2. Common causes are cirrhosis, portal or hepatic vein thrombosis, and Budd-Chiari syndrome. Cirrhosis results from fibrosis narrowing hepatic sinusoids.
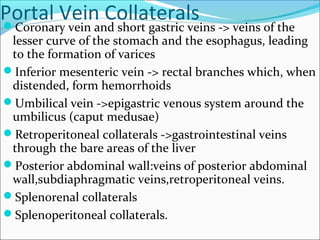
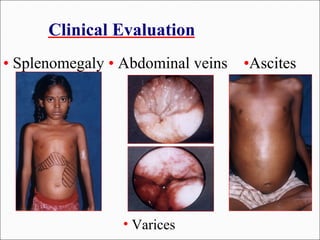
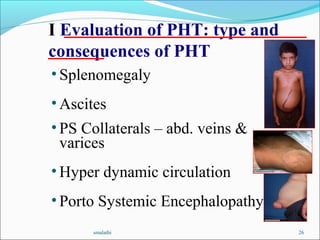
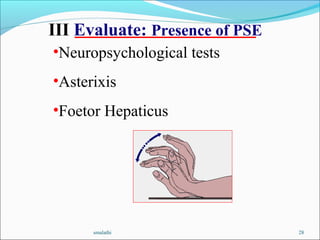
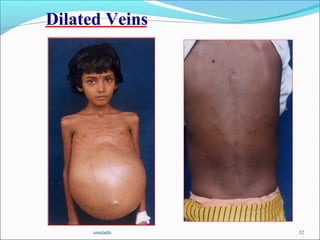
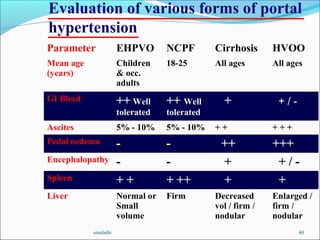
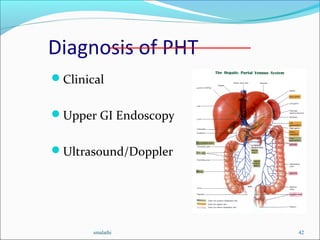
3. Clinical features include splenomegaly, abdominal collaterals, ascites, gastrointestinal bleeding from varices, and hepatic encephalopathy.