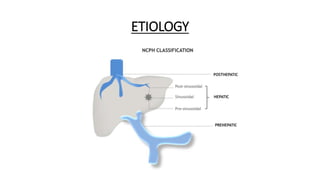
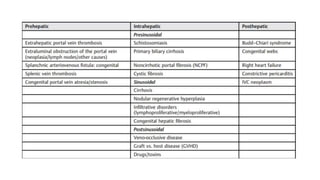
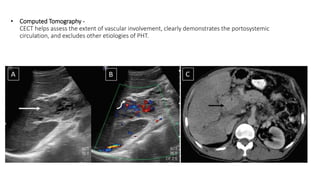
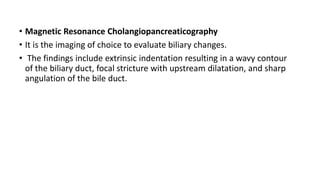
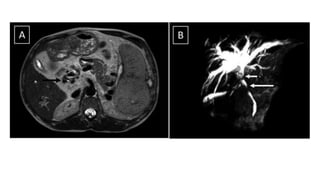
This document discusses portal hypertension and its imaging approach. It defines portal hypertension as increased portal venous pressure due to increased resistance or blood flow. Imaging findings can help identify the underlying etiology, which includes cirrhosis, noncirrhotic portal hypertension, extrahepatic portal vein obstruction, and Budd-Chiari syndrome. Ultrasound, CT, MRI, and Doppler ultrasound are used to evaluate the liver, portal and hepatic vasculature, and for signs of portal hypertension like splenomegaly and collateral vessels. Liver stiffness measurements and hemodynamic studies can also aid diagnosis. The document reviews characteristic imaging findings for each cause of portal hypertension.