Downloaded 13 times

















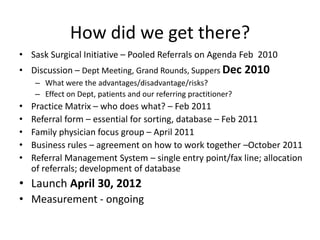

























The document discusses a presentation by Dr. Corrine Jabs on the implementation of pooled referrals within the Regina Qu'Appelle Health Region's obstetrics and gynecology department. The initiative aims to reduce wait time variability, improve patient access, and streamline the referral process, addressing challenges such as inconsistent information and overloaded offices. The session covers the project's objectives, the adopters' journey, ongoing measurement of impact, and the benefits of leveraging data for quality improvement.











































































































