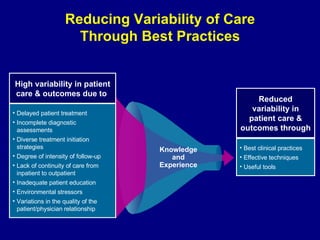
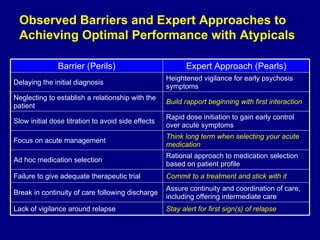
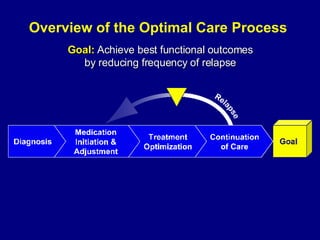
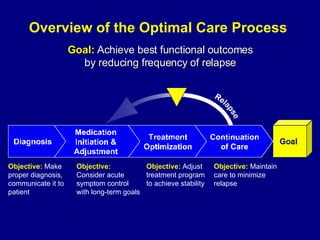
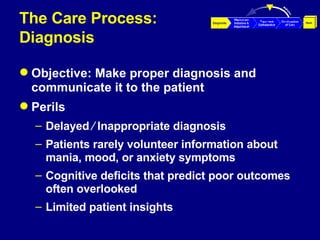
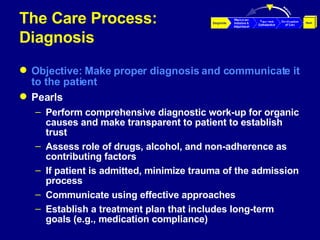
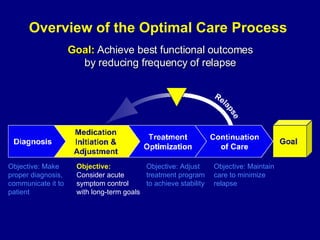
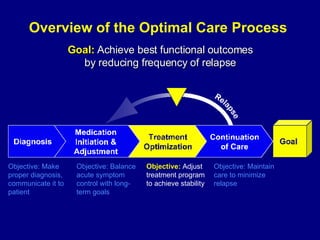
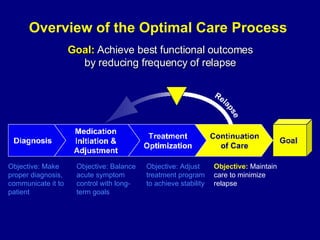
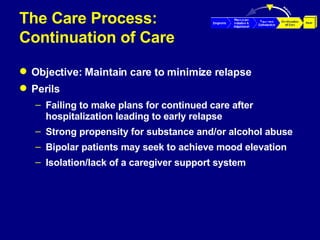
The document discusses optimizing the use of atypical antipsychotics by reducing variability in patient care and outcomes. It outlines a four-step optimal care process: 1) making a proper diagnosis and communicating it to the patient, 2) considering acute symptom control and long-term goals in medication initiation, 3) adjusting treatment to achieve stability, and 4) maintaining care to minimize relapse. Barriers to optimal care are identified along with expert approaches to address them at each step of the care process.


































![Ch1 Ppt Lect 1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/ch1-ppt-lect-11-1194021199672814-4-thumbnail.jpg?width=640&height=640&fit=bounds)










![[ppt] RCpsych - Failing medical care of psychiatric patients (vMar11)](https://cdn.slidesharecdn.com/ss_thumbnails/mitchell11-failingmedicalcareofpsychiatricpatientsv3ajmitchell-110307123958-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)









































