
Recommended
More Related Content
What's hot
What's hot (20)
Similar to 38-character for pneumonia document
Similar to 38-character for pneumonia document (20)
Recently uploaded
Recently uploaded (20)
38-character for pneumonia document
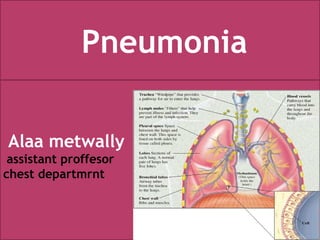
- 1. Alaa metwally assistant proffesor chest departmrnt Pneumonia
- 2. Pneumonia is: an inflammation of the gas exchanging part of the lung (parenchyma of the lung). Most cases of pneunomia are caused by microorganism. Pneumonitis is: an inflammation of the gas exchanging part of the lung due to non infectious causes including aspiration of food or gastric acid foreign bodies, chemicals and lipoid substances. Hypersensitivity reaction and drug or radiation induced pneumonitis. PNEUMONIA, Definition
- 3. 1 : Anatomical classification. A – Lobar pneumonia .Where the consolidation involves all or part of the lobe. B – Bronchopneumonia: The consolidation involves scattered lobules C - Interstitial pneumonia: Inflammatory infiltrate involve mainly interstitial tissue between alveoli as in viral pneumonia. . PNEUMONIA, Classification
- 4. PNEUMONIA, Classification •Community acquired pneumonia (CAP): •Pneumonia which occurred in the community , ambulant patient •Hospital acquired and health care acquired pneumonia (HAP): •Pneumonia occurred after 48 hours of hospital admission, or frequent visits of health care facilities (e.g. hemodialysis patients). •Ventilator associated pneumonia (VAP): •Pneumonia occurred after 48 hours of intubation and/ or mechanical ventilation.
- 5. 2 : Etiological classfication.The cause of pneumonia is often difficult to determine because culture of lung secretions is invasive and rarely performed. • Culture obtained from upper respiratory tract or sputum generally not accurate and usually reflect contamination rather than true pathological organism. PNEUMONIA, Classification
- 6. PNEUMONIA Bacterial.Common. • Streptococcus pneumoniae, Group B streptococci, Group A streptococci . • Mycoplasma pneumoniae. • Chlamydia pneumoniae Adolescent. • Chlamydia trachomatis Infant. • Mixed anaerobes Aspiration pneumonia. • Gram-negative enteric bacilli. E coli, PNEUMONIA, Classification
- 7. Uncommon. - Haemphilus influenza post viral. - Staphylococcus aureus - Moraxella catarrhalis - Neisseria meningitides - Francisella tularensis animal contact - Nocardia species Immunocompromized Pts. - Chlamydia psittaci Bird contact. - Yersinia pestis Plague - Legionella species Exposure to contamianted water. PNEUMONIAPNEUMONIA, Classification
- 8. • Viral, Common Respiratory syncytial virus Parainflueza type 1 – 3 Influeza A . B Adenovirus Metapneumovirus Un Common Rhinovirus Enterovirus Neonates Herpes simplex Neontes Cytomegalovirus Immunosuppressed person. Measles Varicella Hantavirus SARS. PNEUMONIA, Classification
- 9. • Fungal. Histoplasma capsulatum Bird bat contact Cryptococcus neoformans Bird contact. Aspergillus species Immunosuppressed. Mucomycosis Immunosuppressed Coccidioides immitis Blastomyces dermatitides •Rickettsial Coxiella burnetii Goat sheep cattle exposure Rickettsia rickettsiae PNEUMONIA, Classification
- 10. • Mycobacterial Mycobacterium Tuberculosis Developed countries Nycobacterium avium-inteacellulare Immunosuppressed. •Parasitic Pneumocystis Carini Immunosuppressed. Steroid. Eosinophilic Ascaris . Loeffler syndrom •Non infectious causes -Aspiration Of food. -Gastric acid. -foreign body. -Hydrocarbon Kerosen -Lipoid substances - Aspiration of amniotic fluid. PNEUMONIA, Classification
- 11. PNEUMONIA, Predisposing factors Item Example Age Extremes of age (neonates, old age) Diseases DM, renal, hepatic, cardiac, immunocompromised Bad ventilation Poor housing , over crowded places Drugs Long term corticosteroid, immunosuppressive drugs Weather changes Very cold or very hot weather Poor hygene Dental cares, bad oral hygene Local defense abnormality Impaired consciousness, sedative drugs , epilepsy
- 12. PNEUMONIA, • Recurrent pneumonia -Hereditary disorder •Cystic fibrosis •Sickle cell disease -Disorders of immunity •Aqured immunodeficincy syndrome (AIDS) •Bruton agammaglobulemia •Selective IgG subclass deficiencies •Common variable immunodeficiency syndrom •Sever combined immunodeficiency syndrom -Disorders of leukocytes •Chronic granulomatous disease. •Hyperimmunoglobulin E syndrome. •Leukocyte adhesion defect
- 13. PNEUMONIA, etiology Disorders of cilia • Immotile cilia syndrom • Kartagener syndrom Anatomic disorder •Sequestration •Lobar emphysema •Esophageal reflux •Foreign body •Tracheo esophageal fistula ( H type ) •Gastroesophageal reflux •Bronchietasis •Aspiration ( oro pharyngeal in coordination )
- 14. PNEUMONIA • Pathogenesis, The lower respiratory tract is normally sterile by •Physiologic defense mechanisms including •Mucociliary clearance •Normal secretion such as secretory immunoglobulin A IgA •Clearing of air way by coughing •Immunologic defense mechanism of lung limit invasion by pathogenic organisms, including macrophages are present in alveoli and bronchioles secretory IgA and others immunoglobulins
- 15. PNEUMONIA, pathology Viral pneumonia : Usually result from spread of infection along the airway. Accompanied by direct injury of respiratory epithelium resulting in air way obstruction from swelling abnormal secretion and cellular debris small calibar of air way in young infant makes them particularly susceptible to sever infection. Viral infection predispose to secondary bacterial infection by disturbing normal host defense mechanism altering secretion and modifying bacterial flora.
- 16. PNEUMONIA •Bacterial infection In bacterial infection pathologic process varies according to the invading organism : M . Pneumoniae attaches to the respiratory epithelium inhibit ciliary action and Lead to cellular destruction and an inflammatory response in the submucosa as the infection progresses sloughed cellular debris inflammatory cell and mucus cause airway obstruction with spread of infection occuriang along the bronchial Tree as in viral pneumoia. - S . Pneumoniae Produce local edema that aids in the proliferation of organism and their spread Into adjacent portion of lung often resulting in the characteristic focal lobar Involvement
- 17. PNEUMONIA -Grop A . Streptococcus pathology Includes necrosis of tracheobronchial mucosa formation -of large amount of exudate edema and local hemorrhage with extension into the Interalveolar septa and involvement of lymphatic vessel and pleura. -S – aureus pneumonia produces Toxin and enzymes as hemolysin coagulase and -staphylo kinase. It causes broncho pneumonia often unilateral characterized by prensence of hemorrhagic necrosis and irregular areas of cavitation of ,lung parenchyma •Resulting in pneumatoceles empyema or broncho pulmonary fistula Pyopneumothorax.
- 18. PNEUMONIA Following changes stages: 1- congestion alveoli are failed with edema fluid and organism. 2- red hepatization alveoli contain polymorph RBCs fibrin edema and organism. 3-grey hepatization deposition of fibrin over the pleural surface phagocytosis starts inside the alveoli which are now filled with polymorph and fibrin. 4-resolution: neutrophil degenerate fibrin thread and remaining bacteria and digested and removed by phagocyte Clinical Manifestation Viral & bacterial pneumonia are often preceded by several day of symptoms of URTI typically rhinitis and cough. In viral pneumonia: fever is usually present lower than in bacteria. Tachypnea increased work of breathing accompanied by intercostal, subcostal and suprasternal retraction nasal flaring and use of accessory muscle. Severe infection accompanied by cyanosis and respiratory fatigue in infant. Auscultation of chest wheezing and crackle
- 19. PNEUMONIA, Diagnosis, Signs and symptoms
- 20. PNEUMONIA In bacterial pneumonia: Sudden shaking chill followed high fever, cough, grunting, chest pain, drowsiness, rapid respiration, dry cough, anxiety circumoaral cyanosis. Physical finding: Depends on the stage of pneumonia diminished breath sound scattered crackels and rhonchi over affected lung. Increasing consolidation or complication. As effusion empyema or pyopneumothorax dullness on percussion and breath Sound. Diminished abdominal distension because of gastric dilation from swallowed air or ileus. Abdominal pain in lower lobe pneumonia Liver may seem enlarged because downward of diaphragm secondary to hyper inflation of lung Neck rigidity without meningitis in right upper lobe.
- 21. PNEUMONIA, Diagnosis: Chest X-ray •Diagnosis of pneumonia may indicate complication pleural effusion or empyema. •Viral pneumonia X-ray hyper inflation with bilateral interstitial infiltrate. •Pneumococcal pneumonia lobar consolifation repeat chest x-ray are not required for proof of cure for patient with uncomplicated pneumonia. WBC can differentiating viral from bacterial (normal in viral pneumonia or elevated in bacterial pneumonia) -Atypical pneumonia due to C.pneumoniae or M.pneumoniae is difficult to distinguish from pneumococal pneumonia by X-ray and other lab. Sputum cultur and sensitivity, for guidance of antibiotic treatment. CT and fibrooptic bronchoscope may be required in certain cases
- 22. PNEUMONIA • Hospitalization of children with pneumonia -Age < 6 month - Sickle cell anemia with acute chest syndrome. - Multiple lobe involvement. -Immunocompromised -Toxic appearance. -Sever respiratory distress -Requirement for supplemental oxygen. -Dehydration -Vomiting. -No response to oral antibiotic. -Non compliant parent.
- 23. PNEUMONIA, Treatment: Treatment based on the cause and site of occurrence. CAP without comorbidity -Amoxicillin clavulente ( 80-90mg/kg/24 hrs ) OR - Cefuroxime.(2nd generation cephalosporin) OR -Macrolide antibiotic such as azilhromjcin . HAP with other comorbidity ceftriaxone plus Macrolide antibiotic such as azilhromjcin Fluroquinolone ( levofloxacin, moxifloxacin, gemifloxacin) HAP ceftriaxone plus Macrolide antibiotic such as azilhromjcin Fluroquinolone ( levofloxacin, moxifloxacin, gemifloxacin). VAP, consider anti-pseudomonal , anti-staph Piperacillin, Ciprofloxacin, Vancomycin or clindamycin .
- 24. PNEUMONIA Deterioration in clinical status antibiotic therapy should be initiated Response to treatment: Patient with uncomplicated bacterial pneumonia respond to therapy with improvement in clinical symptom (fever, cough, tachypnea, chest pain) within 48-96 hrs. Slowly resolving pneumonia 1- complication as empyema. 2- bacterial resistance. 3- non bacterial etiology as viruses and aspiration of foreign bodies or food. 4- bronchial obstruction from endobronchial lesion foreign body or mucus plug. 5- pre-existing diseases such as immunodeficiencies- ciliary dyskinesia- cysticfibrosis pulmonary sequestration cystic adenomatoid malformation. 6- non infectious causes: - bronchoilitis obliterans. - hypersensitivity pneumonitis - eosinophils pneumonia - aspiration - wegener granulomatosis
- 25. PNEUMONIA Complication: •Usually result of direct spread of bacterial infection within thoracic cavity. (pleural effusion- empyema- pericarditis) . •Bacteremia and hematologic spread meningitis suppurative arthritis osteomyelitis. • •Respiratory failure. •Lung abcess. •Bronchiactasis •
- 27. X-RAYS Lobar pneumonia x-ray (RUL)
- 30. THANKS ALOT