This document provides guidance on performing a physical assessment of a child. It discusses:
1) Major differences between assessing children versus adults, including differences in growth, development, motor skills and other areas.
2) Standard measurements and exam techniques are described for different age groups from newborns to adolescents.
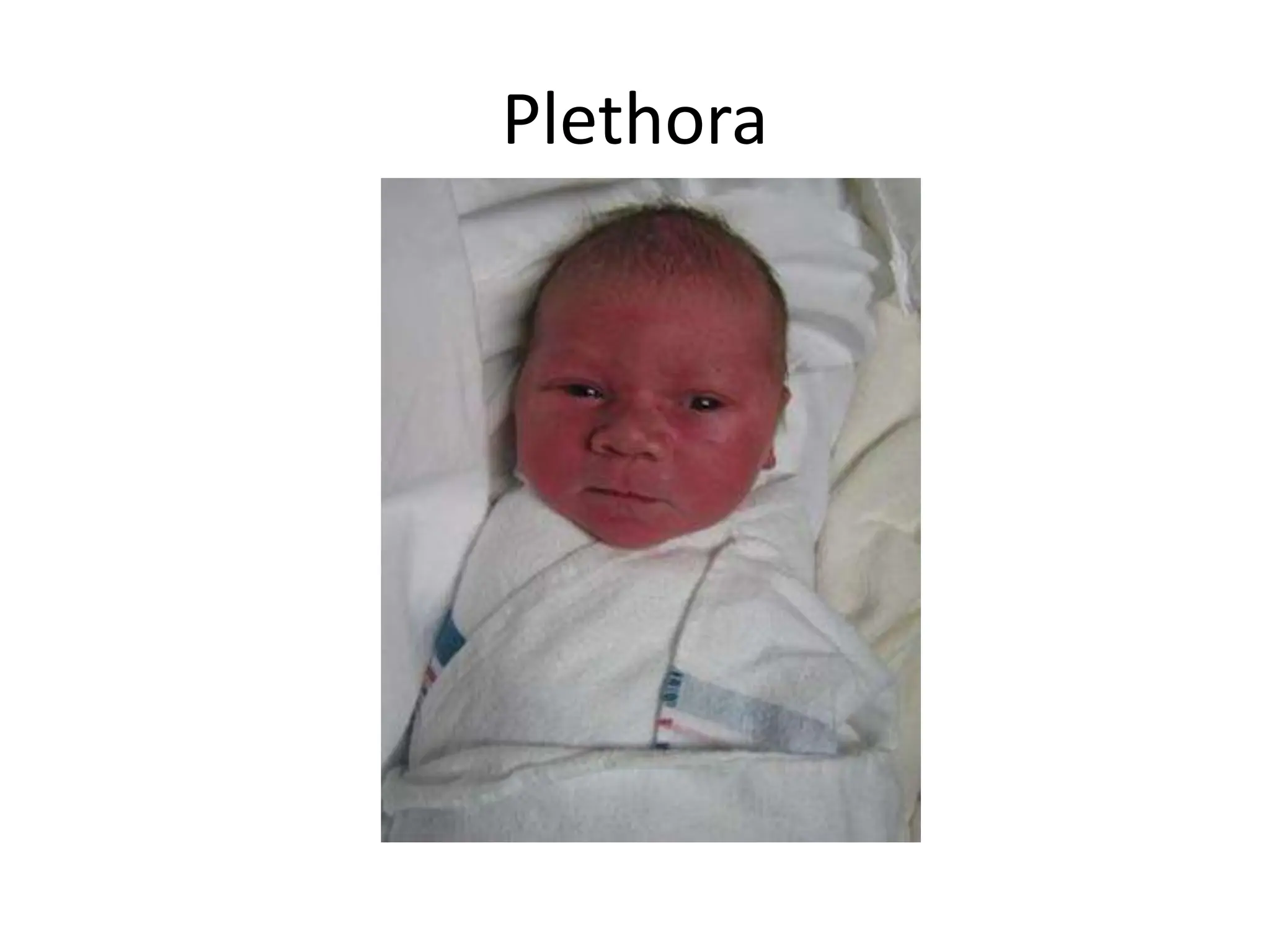
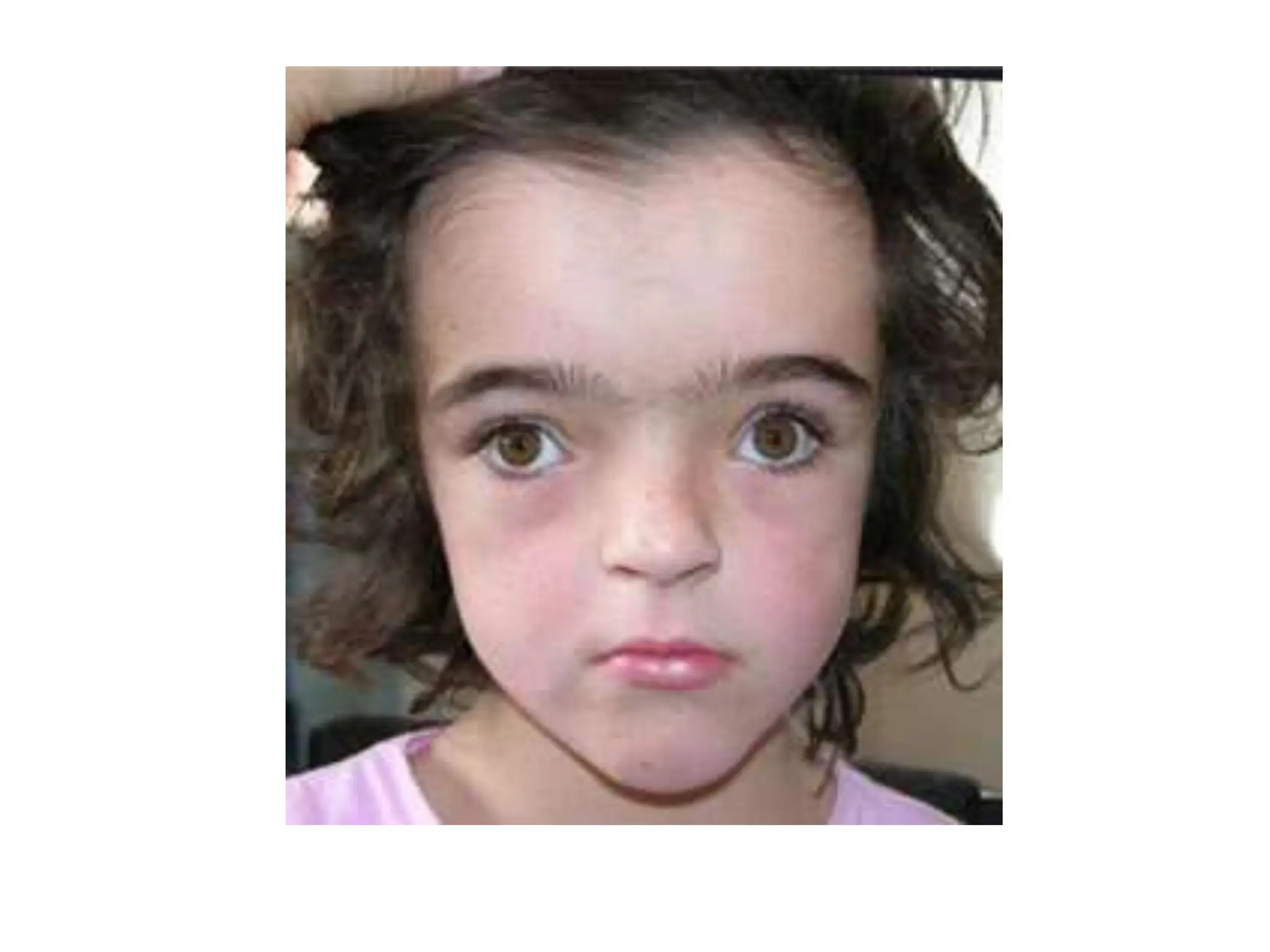
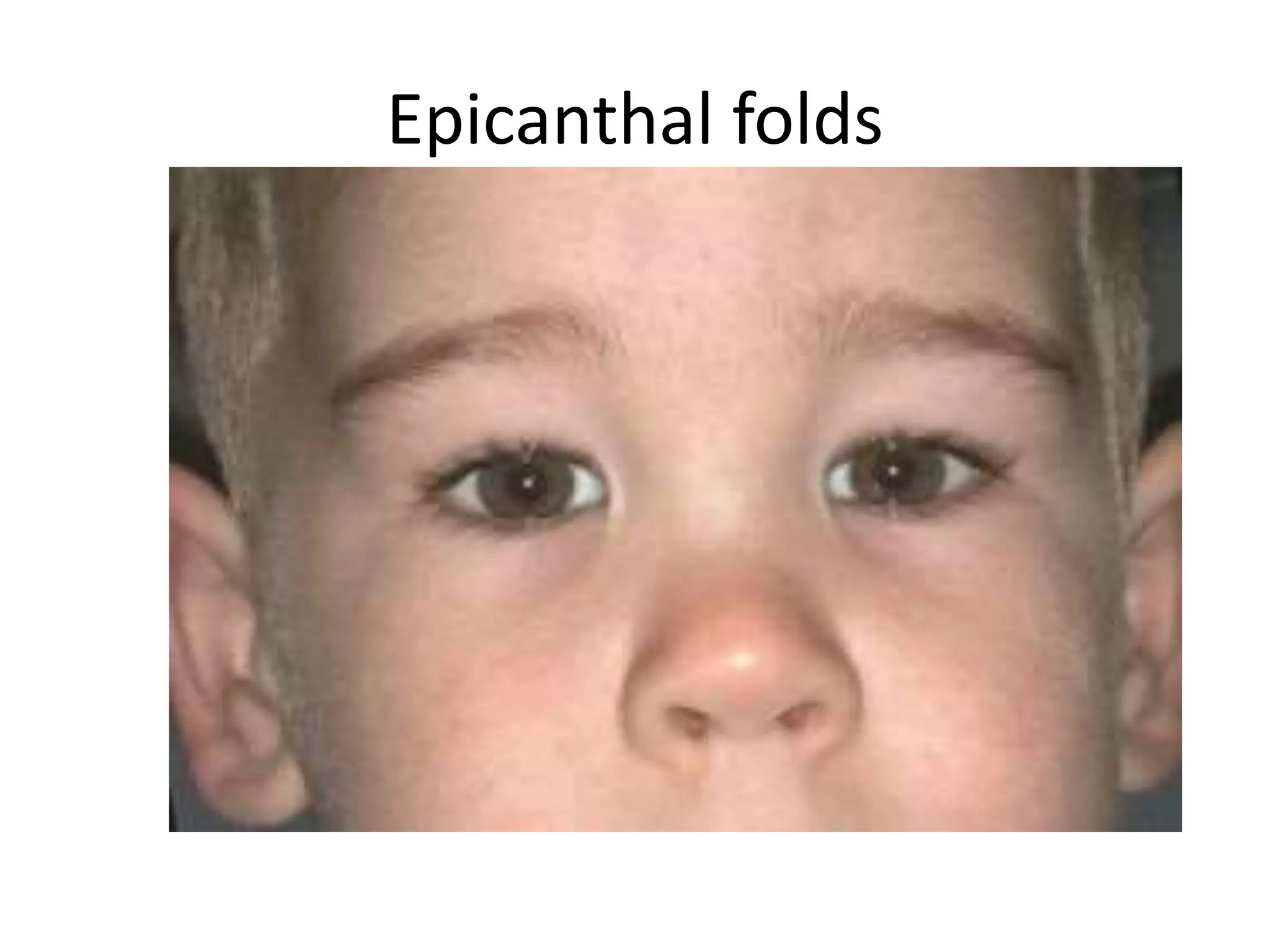
3) A systematic approach is outlined covering the skin, hair, head, eyes, ears, nose, mouth, neck, chest, and other body systems. Common variations, findings and pediatric conditions are also addressed.