This document is the disclaimer for the 8th edition of the Philippine National Formulary. It states that the medicines and prescribing information listed were compiled through collaboration of various experts applying current clinical practice standards. However, there is no guarantee that new medicines or information made available after compilation are included. It also notes that the information provided is a synopsis and not a complete representation of official product labeling. Readers are advised to confirm the information with other sources, especially for new updates.













![iv
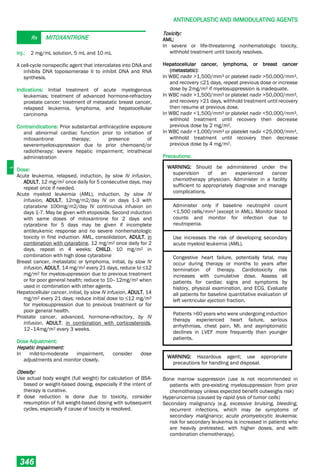
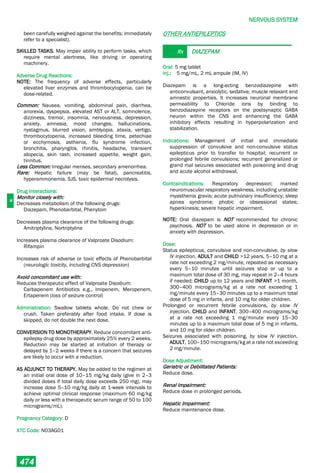
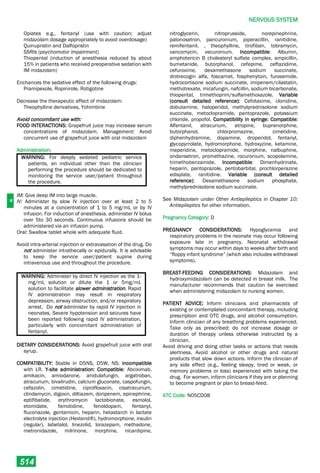
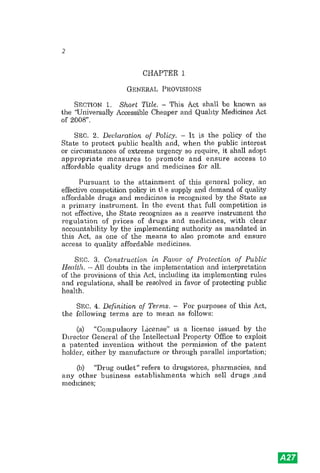
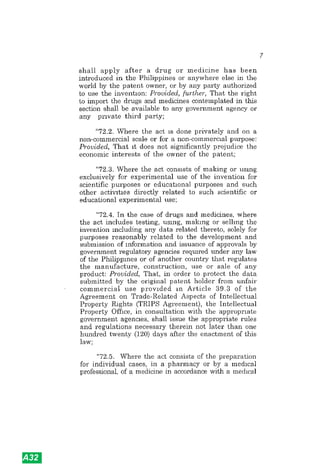
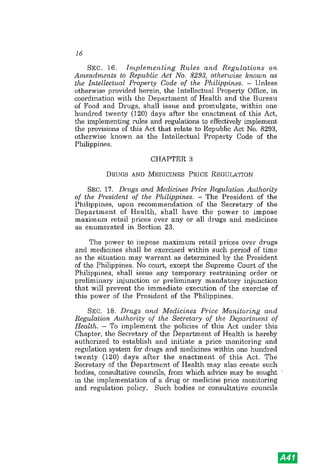
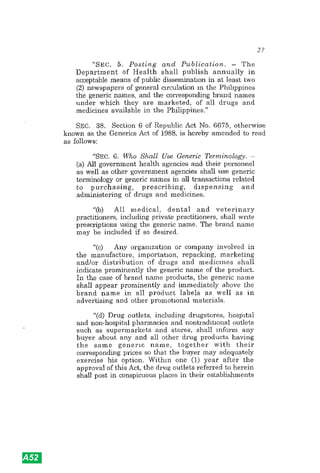
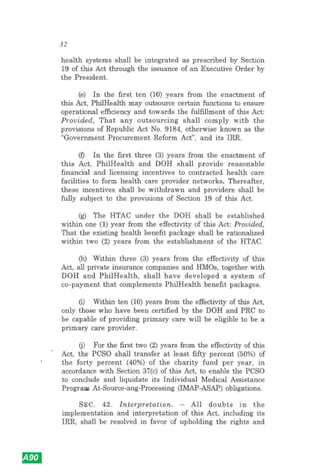
SYMBOLS AND ABBREVIATIONS
ACE - Angiotensin-converting
enzyme
ADR - Adverse drug reaction
AIDS - Acquired
Immunodeficiency
Syndrome
a.m. - Morning; before noon
Amp - Ampule
AV - Atrioventricular
BCG - Bacille Calmette-Guérin
BP - Blood pressure
BSA - Body surface area
cap., caps - Capsule(s)
CNS - Central Nervous System
comp. - Compound
cr., crm. - Cream
CR - Controlled-release
CSF - Cerebrospinal fluid
D5NS - Glucose (dextrose) 5% in
normal saline (0.9%)
D5W - Glucose (dextrose) 5%
solution
DOTS - Directly observed
treatment, short-course
DMARD - Disease modifying agents
in rheumatoid disorders
DPI - Dry powder inhaler
EC - Enteric-coated
ECG - Electrocardiogram
emuls. - Emulsion
EPS - Extrapyramidal syndrome
ER - Extended Release
FC - Film-coated
G - Gram
GFR - Glomerular Filtration Rate
GI - Gastrointestinal
gtt(s) - Drop(s)
h, hr. - Hour
HAI - Hospital-Acquired
Infections
HIV - Human
Immunodeficiency Virus
HRT - Hormone Replacement
Therapy
(ID) - Intradermal
(IM) - Intramuscular
Inj. - Injection
INR - International Normalized
Ratio
IU - International Unit(s)
(IV) - Intravenous
L - Liter
LA - Long-Acting
lin. - Liniment
lot. - Lotion
MAOI - Monoamine Oxidase
Inhibitor
MDI - Metered Dose Inhaler
MDR-TB - Multidrug-resistant
tuberculosis
mEq - Milliequivalent
Mg - Milligram
mL - Milliliter
Mmol - Millimole
MR - Modified release
[includes CR, ER, SR, LA]
nebul. - Spray
NSAID - Non-steroidal Anti-
Inflammatory Drugs
p.m. - Afternoon / Evening
RE - Retinol Equivalent
Resp. Soln. - Respiratory Solution
Rx - Prescription
(SC) - Subcutaneous
(SL) - Sublingual; under the
tongue
sig. - Signa / write on label
Soln. - Solution
spp. - Species
SR - Sustained Release
SSRI - Selective Serotonin
Reuptake Inhibitor
supp. - Suppository
susp. - Suspension
syr. - Syrup
tab., tabs. - Tablet(s)
TB - Tuberculosis
top. - Topical
XDR-TB - Extensively Drug-resistant
Tuberculosis](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-24-320.jpg)



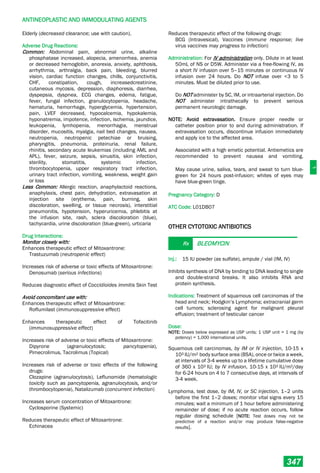
![xii
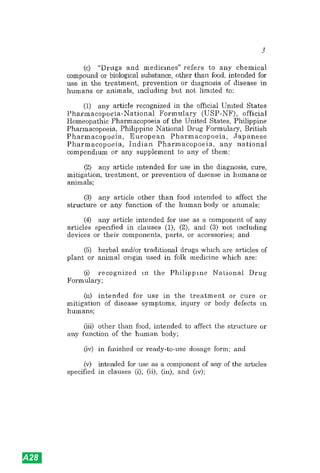
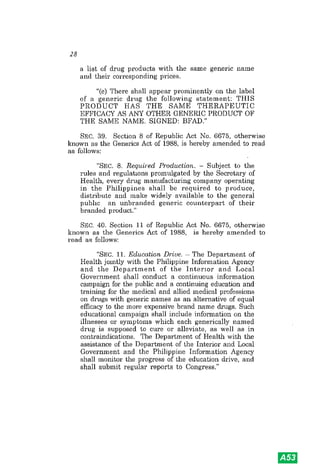
d. INCOMPATIBILITIES BETWEEN MEDICINES AND IV FLUIDS
Medicines should not be added to blood, amino acid solutions, or fat emulsions.
o Certain medicines, when combined with intravenous fluids, may be
inactivated by pH changes, precipitation, or chemical reaction.
e. ADVERSE EFFECTS CAUSED BY TRADITIONAL MEDICINES
Patients who have been, or are taking, traditional herbal remedies may
develop ADRs. In these types of preparation, it is not always easy to identify the
responsible constituents. Refer to the medicine and toxicology information
service if available or to suitable literature.
f. EFFECT OF FOOD ON MEDICINE ABSORPTION
Food delays gastric emptying and reduces the rate of absorption of many
medicines; however, the total amount of medicine absorbed may or may not be
reduced. On the other hand, some medicines are taken with food, either to
increase absorption or to decrease the irritant effect on the stomach.
E PRESCRIPTION WRITING
1. PRESCRIPTION FORM
Administrative Order No. 62 (series of 1989) on the rules and regulations to
implement prescribing requirements under the Generics Act defines a prescription as
a written order and instruction of a validly-registered physician, dentist or veterinarian
for the use of a specific medicine (or medical device) for a specific patient.
The most important requirement for a prescription is that it should be clear. It
should be legible and indicate precisely what should be given. The language used may
be in English, Filipino, or the local dialect.
In accordance with R.A. 5921, or the Pharmacy Act as amended, all prescriptions
should contain the following information:
o The patient’s name, age and sex;
o The prescriber’s name, office address, professional registration number, and
professional tax receipt number; and,
o Date of the prescription
In addition, Section 3 of the Generics Act lists the following specific guidelines to
prescribing:
o Generic names shall be used in all prescriptions. For drugs with a single active
ingredient, the generic name of that active ingredient shall be used in
prescribing. For drugs with two or more active ingredients, the generic name as
determined by the Philippine FDA shall be used.
o The generic name must be written in full, but the salt or chemical form may be
abbreviated. The symbol Rx means prescription which originated in medieval
manuscripts as an abbreviation of the Latin verb recipe. The imperative form is
recipere which means “to take” or “take thus.”)
o The generic name must be clearly written immediately after the Rx symbol or on
the order chart.
o The pharmaceutical form (e.g., “tablet”, “oral solution”, “eye ointment”) should
also be stated.
o The strength of the medicine should be stated in standard units using
abbreviations which are consistent with the Système International (SI) [Refer to
Appendices for abbreviations and symbols].](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-32-320.jpg)








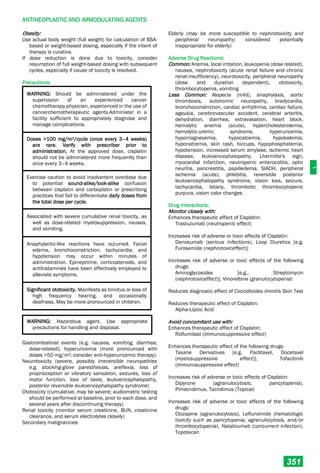
![A
ALIMENTARY TRACT AND METABOLISM
1
ALIMENTARY TRACT AND METABOLISM
DRUGS FOR ACID-RELATED
DISORDERS
ANTACIDS
OTC
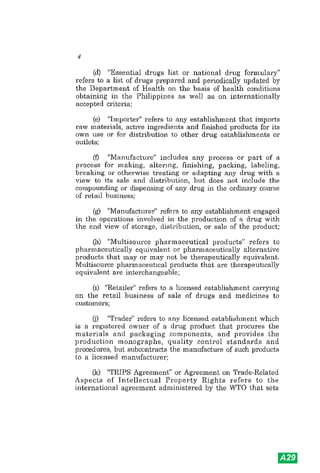
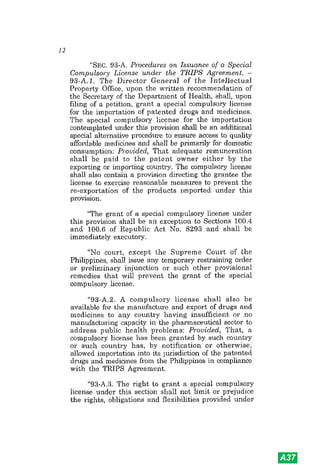
ALUMINUM HYDROXIDE +
MAGNESIUM HYDROXIDE
Oral: 200 mg aluminum hydroxide + 100 mg magnesium
hydroxide tablet
225 mg aluminum hydroxide + 200 mg magnesium
hydroxide per 5 mL suspension, 60 mL and 120 mL
An antacid that combines aluminum hydroxide and
magnesium hydroxide to reduce effect on bowel
movement and to relieve epigastric pain from peptic
ulcer through acid neutralization.
Indication: Symptomatic relief of symptoms related to
hyperacidity from heartburn, hiatal hernia, upset
stomach, peptic ulcer, peptic esophagitis, or gastritis.
Contraindications: Severe renal impairment;
hypophosphatemia; undiagnosed GI and rectal bleeding;
porphyria; appendicitis.
Dose:
Hyperacidity, by mouth, ADULT, 10-20 mL 4 times daily
(maximum 80 mL daily).
Dose Adjustment:
Renal Impairment:
Use with caution due to risk of accumulation and toxicity.
For mild-to-moderate renal impairment, dose reduction is
warranted.
For severe impairment, avoid use and refer patient to a
specialist.
Precautions:
WARNING: Aluminum and magnesium salts may be
hazardous in patients with renal insufficiency. If
intensive antacid therapy is to be used, only non-
systemic (non-absorbable) antacids should be
considered because of the potential danger of
alkalosis with systemic therapy.
Acute porphyria; prolonged antacid therapy may result in
hypophosphatemia (i.e., decreased phosphate
absorption in the GI tract); dehydration; fluid restriction;
constipation; diarrhea; hepatic impairment; renal
impairment; GI disorders associated with decreased
bowel motility or obstruction; some products may contain
phenylalanine.
Elderly (may be predisposed to diarrhea or constipation);
children.
Adverse Drug Reactions:
Common: Constipation, diarrhea, GI irritation.
Less Common: Chalky taste, fecal discoloration,
hypophosphatemia, nausea, vomiting.
Rare: Anemia, encephalopathy, fecal impaction,
hypermagnesemia, hypophosphatemia, intestinal
obstruction, osteomalacia, proximal myopathy.
Drug Interactions:
Monitor closely with:
Increases excretion due to urine alkalinization:
Acetylsalicylic Acid
Reduces absorption of the following drugs:
Azithromycin, Chloroquine, Digoxin, Enalapril, Isoniazid,
Rifampicin
Avoid concomitant use with:
Reduces therapeutic effect of the following drugs
Bisphosphonates e.g., Alendronate, Iron, Ketoconazole,
Quinolones e.g., Nalidixic acid, Rosuvastatin,
Tetracyclines, e.g., Doxycycline. [Separate dosing by at
least 2 hours before, or 4–6 hours after the antacid]:
Administration: Shake well before use.
Best given 1–3 hours after the last meal to neutralize and
buffer the acid produced.
NOTE: Antacids should preferably not be taken at the same
time as other oral drugs since they may impair
absorption (interactions may be avoided by having an
interval of at least 2 hours between taking an antacid
and the other drug).
Pregnancy Category: B
ATC Code: A02AD01
OTC SODIUM BICARBONATE
Oral: 325 mg and 650 mg tablet
A short-acting, potent systemic antacid that rapidly
neutralizes gastric acid to form sodium chloride, carbon
dioxide, and water. After absorption of sodium
bicarbonate, plasma alkali reserve is increased, and
excess sodium and bicarbonate ions are excreted in
urine, rendering urine less acid.
Indications: Symptomatic relief of hyperacidity (belching,
heartburn, indigestion, gas pains), gastritis, and peptic
ulcer; urine alkalinizer.
Contraindications: Diuretics known to produce
hypochloremic alkalosis; edema; hypertension;
hypocalcemia; hypochloremia; hypernatremia; impaired
renal function; metabolic alkalosis; respiratory alkalosis
or acidosis; any situation where administration of sodium
could be clinically detrimental.
Dose:
Antacid, by mouth, ADULT, 2–8 tablets every 4 hours
(maximum, 48 tablets in 24 hours); ADULT ≥60 years, 2–
4 tablets every 4 hours (maximum, 24 tablets in 24
hours.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-45-320.jpg)


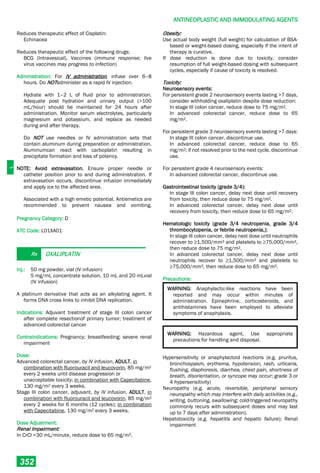
![A
ALIMENTARY TRACT AND METABOLISM
4
by IV intermittent bolus or infusion, ADULT, 50 mg every
6–8 hours; 50 mg every 6–8 hours (if increased doses
are necessary utilize more frequent administration up to
a maximum of 400 mg daily);
by continuous IV infusion, ADULT, 6.25 mg/hour; by IV
injection, INFANT, CHILD, and ADOLESCENT <16 years,
2–4 mg/kg daily divided every 6–8 hours (maximum
dose, 50 mg/dose).
Dose Adjustment:
Renal Impairment:
For patients with creatinine clearance <50 mL/minute,
adjust dose cautiously. Adjust dosing schedule to not
coincide with the end of hemodialysis.
Precautions:
WARNING: NOT to be used if there is trouble or pain
when swallowing food, vomiting with blood, or bloody
or black stools.
NOT to be used in combination with other acid
reducers. Avoid the use of 150 mg tablet for patients
with kidney disease.
Relief of symptoms does not preclude the presence
of a gastric malignancy.
Rare cases of reversible confusion have been associated
with use, usually among elderly or severely ill patients, or
in patients with renal or hepatic impairment.
Prolonged treatment (≥2 years) may lead to vitamin B12
malabsorption and subsequent vitamin B12 deficiency.
Decreased renal or hepatic function (use with caution).
Elderly (use with caution)
Pregnancy; lactation (excreted into breast milk; use with
caution).
Adverse Drug Reactions:
Common: Headache, abdominal pain, constipation,
diarrhea, nausea, and vomiting.
Less Common: Asystole, atrioventricular block, bradycardia
(with rapid IV administration), premature ventricular
beats, tachycardia, vasculitis.
Drug Interactions:
Monitor closely with:
Decreases absorption of the following drugs:
Cephalosporins, Iron salts [except ferric carboxymaltose,
ferric citrate, ferric gluconate, ferric pyrophosphate
citrate, iron dextran complex, iron sucrose]
Enhances therapeutic effect of: Procainamide
Reduces therapeutic effect of:
Warfarin (decreased prothrombin time)
Avoid concomitant use with:
Decreases absorption of the following drugs:
Cyanocobalamin / Vitamin B12
Decreases serum concentration of Azoles, e.g.,
Ketoconazole
Decreases therapeutic effect of Ranitidine:
Cigarette smoking
Decreases therapeutic effect of Diazepam
Administration:
For IM administration, no dilution is required.
For IV administration, solution must be diluted. May be
administered by intermittent bolus, intermittent IV
infusion, or continuous IV infusion.
Pregnancy Category: B
ATC Code: A02BA02
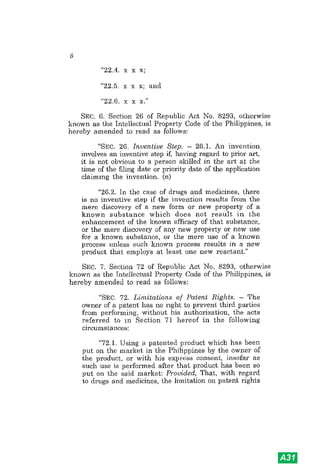
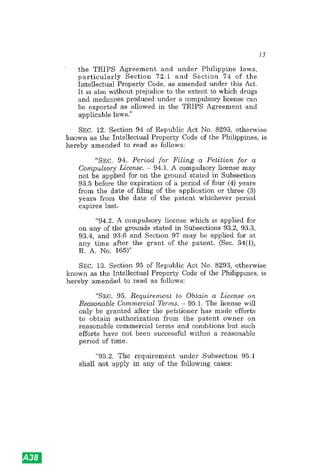
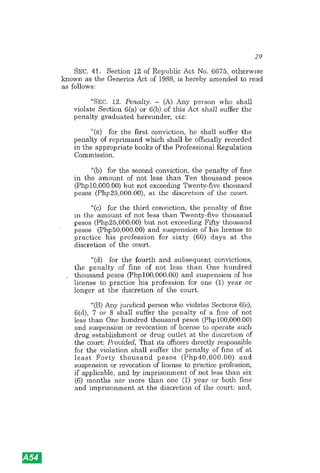
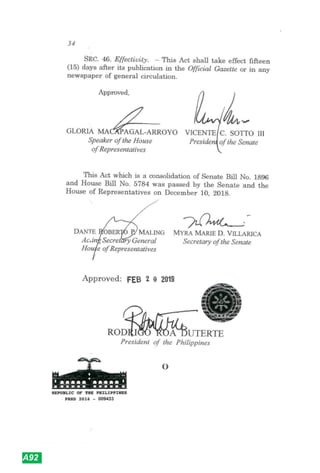
PROTON PUMP INHIBITORS
Rx LANSOPRAZOLE
Oral: 15 mg and 30 mg capsule
15 mg and 30 mg MR tablet
A substituted benzimidazole, which acts as a proton pump
inhibitor (PPI), by blocking the final step of acid
production. It acts by inhibiting the H+/K+–ATPase
system at the parietal cells of the stomach, suppressing
both basal and stimulated gastric acid secretion.
Indications: Management of acid-related dyspepsia, erosive
esophagitis, Gastroesophageal Reflux Disease (GERD),
peptic ulcer, Helicobacter pylori infection, NSAID-
associated ulcer, Zollinger-Ellison syndrome.
Contraindication: Known severe hypersensitivity to
lansoprazole or any ingredient in the formulation
Dose:
Acid-related dyspepsia, by mouth, ADULT, 15–30 mg once
daily in the morning for 2–4 weeks.
GERD, acute therapy, by mouth, ADULT, 15–30 mg once
daily in the morning for 4–8 weeks.
GERD, maintenance therapy, by mouth, ADULT,
maintenance therapy, 15–30 mg once daily (adjust
dosing according to response); CHILD 12–17 years, 15
mg once daily for up to 8 weeks; CHILD 1–11 years (≤30
kg), 15 mg once daily in the morning for up to 12 weeks;
CHILD >30 kg, 30 mg once daily in the morning for up to
12 weeks (may increase doses up to 30 mg twice daily if
patient is still symptomatic after 2 or more weeks of
treatment).
Erosive esophagitis, acute therapy, by mouth, ADULT, 30 mg
once in the morning for up to 8 weeks; by IV injection,
ADULT, 30 mg over 30 minutes for up to 7 days; CHILD
12–17 years, 30 mg once daily for up to 8 weeks; CHILD
1–11 years (≤30 kg), 15 mg once daily in the morning for
up to 12 weeks; CHILD >30 kg, 30 mg once daily in the
morning for up to 12 weeks (may increase doses up to
30 mg twice daily if patient is still symptomatic after 2 or
more weeks of treatment).
Erosive esophagitis, maintenance therapy, by mouth,
ADULT, 15 mg once daily.
Peptic ulcer, acute therapy, by mouth, ADULT, 15 mg once
daily.
Peptic ulcer, maintenance therapy, by mouth, ADULT, 30 mg
once daily in the morning for up to 4 weeks (for duodenal
ulcer) or up to 8 weeks (for gastric ulcer).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-48-320.jpg)






![A
ALIMENTARY TRACT AND METABOLISM
12
irradiation, then 8 m every 8 hours after first dose for 1–
2 days after completion of radiotherapy.
Prevention of radiation therapy-induced nausea and
vomiting, daily fractionated radiotherapy to abdomen, by
mouth, ADULT, 8 mg 1–2 hours before irradiation, then
8 mg every 8 hours after first dose for each day of
radiotherapy.
Prevention of postoperative nausea and vomiting, by IM or
IV injection, ADULT, 4 mg as a single dose (over 2–5
minutes if by IV), administered approximately 30 minutes
before the end of anesthesia or as treatment if vomiting
occurs after surgery, repeat doses are generally
ineffective;
by IV injection, CHILD >40 kg, 4 mg as a single dose over
2–5 minutes; CHILD ≤40 kg, 0.1 mg/kg as a single dose
over 2–5 minutes.
NOTE: Single IV doses >16 mg is not recommended due to
the potential for QT prolongation.
Dose Adjustment:
Hepatic Impairment:
For severe hepatic impairment, maximum daily dose for oral
and parenteral administration is 8 mg.
Precautions:
QT prolongation (e.g., torsade de pointes); ileus or gastric
distention.
Adverse Drug Reactions:
Common: Headache, fatigue, malaise, constipation,
drowsiness, sedation, dizziness, agitation, anxiety,
paresthesia, sensation of cold, pruritus, skin rash,
diarrhea, urinary retention, elevated ALT and AST,
injection site reaction, hypoxia, fever.
Less Common: Abdominal pain, accommodation
disturbance, anaphylaxis, angina pectoris, angioedema,
atrial fibrillation, anaphylactoid reaction, bradycardia,
bronchospasm, cardiac arrhythmia, cardiorespiratory
arrest, bullous skin disease, chest pain, chills,
depression of ST segment on ECG, dyspnea, dystonic
reaction, ECG changes, extrapyramidal reaction,
hypersensitivity reaction, hypokalemia, hepatic failure,
hypotension, ischemic heart disease, laryngeal edema,
laryngospasm, mucosal tissue reaction, myocardial
infarction, neuroleptic malignant syndrome, oculogyric
crisis, palpitations, positive lymphocyte transformation
test, prolonged QT interval on ECG, second-degree
atrioventricular block, serotonin syndrome, shock,
Stevens-Johnson syndrome, stridor, supraventricular
tachycardia, syncope, tachycardia, tonic-clonic seizures,
torsade de pointes, toxic epidermal necrolysis, transient
blindness (≤48 hours), transient blurred vision (following
infusion), urticaria, vascular occlusive events, ventricular
premature contractions, ventricular tachycardia,
weakness, xerostomia.
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of the following drugs:
QTc-prolonging agents, Serotonin Modulators
(serotonergic effect)
Increases risk of adverse or toxic effects of Serotonin
Modulators
Reduces therapeutic effect of the following drugs:
Tapentadol (analgesic effect), Tramadol (analgesic
effect)
Avoid concomitant use with:
Decreases serum concentration of Ondansetron:
CYP3A4 Inducers, Dabrafenib, Mitotane
Increases risk of adverse or toxic effects of the following
drugs:
Apomorphine (hypotensive effect), Ivabradine,
Mifepristone, QTc-prolonging agents (QTc-prolonging
effect)
Increases serum concentration of the following drugs:
Tizanidine [if concomitant use cannot be avoided, initiate
tizanidine at 2 mg and increase in 2–4 mg increments
based on patient response]
Administration:
For oral administration, administer 30 minutes prior to
chemotherapy, 1–2 hours before radiotherapy, or 1 hour
prior to induction of anesthesia.
For IM injection, administer undiluted.
For IVPB, infuse diluted solution over 15–30 minutes.
For IV push, single doses may be administered by IV
injection as undiluted solution over 2–5 minutes.
For IV infusion, dilute in 50 mL D5W or NS.
Pregnancy Category: B
ATC Code: A04AA01
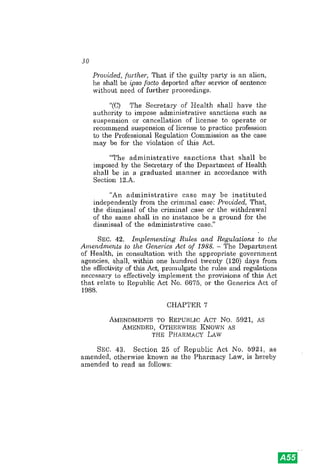
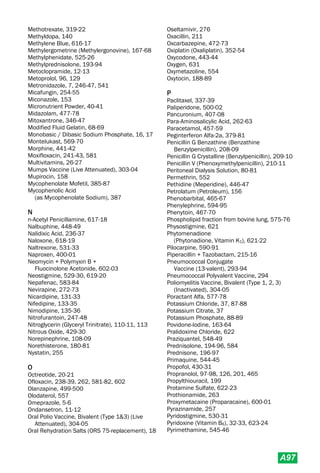
Rx METOCLOPRAMIDE
Oral: 10 mg tablet (as hydrochloride)
5 mg/5 mL syrup (as base and as hydrochloride), 60
mL
Inj.: 5 mg/mL (as base and as hydrochloride), 2 mL
ampule (IM, IV)
A dopamine (D2) antagonist that blocks receptors in the
chemoreceptor trigger zone of the medulla, resulting in
potent anti-nausea and antiemetic action; also blocks
receptors in the GI tract, stimulating gastric emptying
and small intestinal transit.
Indications: Management of nausea and vomiting in GI
disorders, in migraine, and in chemotherapy and
radiotherapy; disorders of decreased gastrointestinal
motility such as gastroparesis or ileus; Gastroesophageal
Reflux Disease (GERD).
NOTE: In children and adolescents <20 years, use is
restricted to treatment of severe intractable vomiting of
known etiology, as an aid to GI intubation, management
of radiotherapy and chemotherapy-induced nausea and
vomiting, and as premedication.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-56-320.jpg)

![A
ALIMENTARY TRACT AND METABOLISM
14
malaise, metallic taste, myalgia, peripheral edema,
pruritus, urticaria, weakness.
Drug Interactions:
Monitor closely with:
Reduces therapeutic effect of Ursodeoxycholic Acid:
Estrogen Derivatives e.g. estriol, Fibric Acid Derivatives
e.g. clofibrate
Avoid concomitant use with:
Decreases absorption of Nitrendipine
Decreases serum concentration of Ursodeoxycholic Acid:
Aluminum Hydroxide [administer Ursodeoxycholic Acid 2
hours before or 6 hours after Aluminum-containing
Antacid products], Bile Acid Sequestrants [administer
Ursodeoxycholic Acid at least 5 hours after Bile Acid
Sequestrants]
Administration: To be taken with food.
Pregnancy Category: B
ATC Code: A05AA02
DRUGS FOR CONSTIPATION
LAXATIVES
OTC BISACODYL
Oral: 5 mg tablet
5 mg MR tablet
Rectal: 5 mg suppository (for children)
10 mg suppository (for adults)
A diphenylmethane stimulant laxative that acts by
stimulating peristalsis by directly irritating the smooth
muscle of the large intestine. It also alters water and
electrolyte secretion, producing net interstitial fluid
accumulation and laxation.
Indications: Bowel evacuation before investigational
procedures or surgery; management of constipation.
Contraindications: Acute abdominal conditions (e.g.
appendicitis, intestinal inflammatory bowel disease);
intestinal obstruction; ileus; severe dehydration; severe
abdominal pain associated w/ nausea and vomiting;
anal fissures or ulcerative colitis w/ mucosal damage
(rectal).
Dose:
Bowel evacuation, by mouth, ADULT, initially 10–20 mg the
night before the procedure followed by 10 mg rectal
suppository the next morning (or 10 mg on each of the 2
nights before the procedure); CHILD 4–10 years, 5 mg
the night before the procedure and 5 mg rectal
suppository the following morning.
Constipation, by mouth, ADULT, 5–10 mg at night, up to 20
mg may be given as necessary; CHILD 4 to 10 years, 5
mg at night;
by rectum, ADULT, 10 mg in the morning; CHILD ≤10
years, 5 mg in the morning.
Precautions:
Intestinal obstruction or acute abdominal conditions such
as appendicitis; inflammatory bowel disease; severe
dehydration; anal fissures, proctitis, ulcerated
hemorrhoids (avoid use of suppositories).
Adverse Drug Reactions:
Common: Abdominal discomfort, diarrhea, electrolyte
disturbance, nausea, vertigo, vomiting, hematochezia.
Less Common: Irritation, proctitis (rectal)
Rare: Hypersensitivity reactions
Drug Interactions: No information found
Administration: To be taken on an empty stomach.
For tablets, administer the evening before if a morning
bowel movement is desired. MR tablets must be
swallowed whole and not crushed or chewed. Do NOT
take within 1 hour of antacids or milk.
For suppositories, administer at the time a bowel
movement is desired.
Pregnancy Category: C
ATC Code: A06AB02
OTC CASTOR OIL
Oral: USP grade
A fixed oil obtained from the seeds of Ricinus communis
that is used as a stimulant laxative. It is hydrolyzed to
ricinoleic acid in the small intestine, which reduces net
absorption of fluid and electrolytes and stimulates
peristalsis.
Indication: Temporary relief of occasional constipation;
bowel evacuation.
Contraindications: Abdominal pain, nausea, vomiting
Dose:
Bowel evacuation / constipation, by mouth, ADULT, 15 to 60
mL as a single dose; CHILD 2–11 years, 5 to 15 mL as a
single dose.
Precautions:
WARNING: Do NOT use for >1 week or when
abdominal pain, nausea, vomiting, or rectal
bleeding are present unless directed by health care
provider.
Elderly (e.g., severe fluid and electrolyte loss, which may
affect mental function);
Pregnancy (associated with induction of labor).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-58-320.jpg)




![A
ALIMENTARY TRACT AND METABOLISM
20
Dose Adjustment:
Renal Impairment:
Dose adjustment may be necessary because mesalazine is
renally eliminated. Use with caution.
If GFR <20 mL/min, use is contraindicated.
Hepatic Impairment:
Use with caution.
Precautions:
Elderly (may have difficulty administering and retaining
rectal suppositories).
Adverse Drug Reactions:
Common: Headache, abdominal pain, eructation, nausea,
exacerbation of ulcerative colitis, nasopharyngitis,
pharyngitis, chest pain, peripheral edema, vasodilation,
hypertension, dizziness, chills, fatigue, vertigo, anxiety,
migraine, nervousness, paresthesia, insomnia, malaise,
skin rash, diaphoresis, pruritus, alopecia, acne vulgaris,
weight loss, diarrhea, dyspepsia, flatulence,
constipation, vomiting, intolerance syndrome, abnormal
stools, gastroenteritis, gastrointestinal hemorrhage,
rectal hemorrhage, tenesmus, bloody diarrhea,
pancreatitis, rectal pain, sclerosing cholangitis,
abdominal distention, anorectal pain (on insertion of
enema tip), hemorrhoids, polyuria, decreased hematocrit
and hemoglobin, abnormal hepatic function tests,
infection, back pain, hypertonia, arthralgia, myalgia,
weakness, arthritis, musculoskeletal pain, visual
disturbance, conjunctivitis, tinnitus, otalgia, hematuria,
decreased creatinine clearance, sinusitis, rhinitis, cough,
flu-like symptoms, dyspnea, bronchitis.
Drug Interactions:
Monitor closely with:
Decreases metabolism of Thiopurine Analogues e.g.,
azathioprine
Decreases serum concentration of Cardiac Glycosides e.g.,
Digoxin
Increases risk of adverse or toxic effects of Mesalazine:
NSAIDs (nephrotoxic effect)
Increases risk of adverse or toxic effects of Heparin (risk for
bleeding / bruising)
Avoid concomitant use with:
Increases risk of adverse or toxic effects of Varicella virus-
containing Vaccines (potential development of Reye’s
Syndrome)
Reduces therapeutic effect of Mesalazine
Antacids (separate administration and/or lower antacid
doses to prevent interaction)
H2-Antagonists, Proton Pump Inhibitors
Administration:
For tablets, swallow whole. Do NOT break, chew, or
crush. Do NOT administer with antacids.
For suppositories, remove foil wrapper prior to
administration. Avoid excessive handling. Retain for at
least 1–3 hours to achieve maximum benefit.
Pregnancy Category: B / C (product specific)
ATC Code: A07EC02
HORMONAL DRUGS USED FOR ESOPHAGEAL
VARICES
HYPOTHALAMIC HORMONES
Rx OCTREOTIDE
Inj.: 100 micrograms/mL and 500 micrograms/mL (as
acetate), 1 mL ampule (IV infusion) wort
Octreotide is a synthetic polypeptide related to
somatostatin, a. growth hormone inhibiting factor.
Indication: For hemostasis for esophageal varices
Dose:
For esophageal varices bleeding, by IV injection, ADULT, IV
bolus of 25–100 micrograms (usual bolus dose, 50
micrograms) followed by continuous IV infusion of 25–
50 micrograms per hour for 2–5 days; may repeat bolus
in first hour if hemorrhage is not controlled. [NOTE:
Withdraw yearly for a 4-week interval (8 for depot
injection) in patients who have received irradiation.
Resume if levels increase and signs or symptoms recur].
For vasoactive intestinal peptide tumors (VIPomas), by IV
injection, ADULT, 200–300 micrograms daily in 2–4
divided doses for the first 2 weeks; titrate dose based on
response or tolerance (range, 150–750 micrograms
daily; doses >450 micrograms daily are rarely required).
Dose Adjustment:
Geriatric:
Dose adjustment may be required. Begin dosing at the lower
end of dosing range. Elimination half-life is increased by
46% and clearance is decreased by 26%.
Renal Impairment:
If dialysis-dependent, no specific dose adjustments
indicated. However, dose adjustment may be needed
since clearance is reduced by ~50%.
Precautions:
Cholelithiasis; Glucose regulation; Hypothyroidism;
Pancreatitis; Cardiovascular disease; Excessive fluid
loss.
Prophylactic cholecystectomy is recommended in patients
with gastrointestinal or pancreatic neuroendocrine
tumors undergoing abdominal surgery if octreotide
treatment is planned
Patients on TPN (periodically monitor for elevations in zinc
levels).
TEST INTERACTION. Chronic treatment has been associated
with abnormal Schillings test.
Adverse Drug Reactions:
Common: Sinus bradycardia, fatigue, headache, malaise,
dizziness, pruritus, hyperglycemia, fever, abdominal
pain, loose stools, nausea, diarrhea, flatulence,](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-64-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
21
cholelithiasis, biliary sludge, constipation, vomiting,
biliary duct dilatation, injection site pain, back pain,
arthropathy, myalgia, upper respiratory tract infection,
dyspnea, antibodies to octreotide, flu symptoms
Less Common: Hypertension, conduction abnormalities,
arrhythmia, palpitation, peripheral edema, pain, anxiety,
confusion, hypoesthesia, insomnia, rash, alopecia,
dyspepsia, steatorrhea, tenesmus, anorexia, cramping,
arthralgia, myalgia, paresthesia, anemia, weakness,
earache, renal calculus, cough, pharyngitis, rhinitis,
sinusitis, allergy, diaphoresis, angina, cardiac failure,
edema, flushing, hematoma, phlebitis, abnormal gait,
amnesia, depression, dysphonia, hallucinations,
nervousness, neuralgia, somnolence, vertigo, acne,
rigors, bruising, cellulitis, hypoglycaemia, hypokalemia,
gout, cachexia, breast pain, impotence, colitis,
diverticulitis, dysphagia, gastritis, gastroenteritis,
gingivitis, glossitis, melena, stomatitis, taste perversion,
xerostomia, incontinence, urinary tract infection,
injection site hematoma, fat malabsorption,
hyperkinesia, hypertonia, joint pain, neuropathy, tremor,
blurred vision, visual disturbance, tinnitus, renal
abscess, bronchitis, epistaxis, bacterial infection,
moniliasis
Rare: Amenorrhea, anaphylactic shock, anaphylactoid
reactions, aneurysm, aphasia, appendicitis, arthritis,
ascending cholangitis, ascites, atrial fibrillation, basal
cell carcinoma, Bell's palsy, biliary obstruction, breast
carcinoma, cardiac arrest, cerebral vascular disorder,
CHF, cholecystitis, cholestatic hepatitis, CK increased,
creatinine increased, deafness, diabetes insipidus,
diabetes mellitus, facial edema, fatty liver, galactorrhea,
GI bleeding, GI hemorrhage, GI ulcer, glaucoma,
gynecomastia, gallbladder polyp, hematuria,
hemiparesis, hemorrhoids, hearing impairment,
hepatitis, hyperesthesia, hypertensive reaction,
hypoadrenalism, hypoxia (children), intestinal
obstruction, intracranial hemorrhage, intraocular
pressure increased, iron deficiency, ischemia, jaundice,
joint effusion, increased LFTs, decreased libido,
malignant hyperpyrexia, MI, necrotizing enterocolitis
(neonates), migraine, nephrolithiasis, neuritis,
oligomenorrhea, pancreatitis, orthostatic hypotension,
pancytopenia, paranoia, paresis, petechiae, pituitary
apoplexy, pleural effusion, pneumonia, pneumothorax,
polymenorrhea, pulmonary embolism, pulmonary
hypertension, pulmonary nodule, QT prolongation,
Raynaud’s syndrome, rectal bleeding, renal failure, renal
insufficiency, retinal vein thrombosis, scotoma, seizures,
status asthmaticus, suicide attempt, syncope,
tachycardia, thrombocytopenia, thrombophlebitis,
thrombosis, urticaria, vaginitis, visual field defect,
vitamin B12 deficiency, weight loss, wheal or erythema
Drug Interactions:
Monitor closely with:
Decreases metabolism of Codeine [impairs formation of two
major metabolites, morphine and norcodeine]
Enhances therapeutic effect of the following drugs:
Antidiabetic Agents, Bradycardia-causing Agents,
Ivabradine (bradycardic effect)
Increases risk of adverse or toxic effects of Octreotide:
Androgens [except Danazol] (hypoglycemic effect),
Bretylium (bradycardic effect; AV blockade), Herbs with
Hypoglycemic Properties (hypoglycemic effect), MAO
Inhibitors (hypoglycemic effect), Other Hypoglycemia-
associated Agents (hypoglycemic effect), Pegvisomant
(hypoglycemic effect), Quinolone Antibiotics
(hypoglycemic effect), Ruxolitinib (bradycardic effect),
Salicylates (hypoglycemic effect), Selective Serotonin
Reuptake Inhibitors e.g. fluoxetine (hypoglycemic effect),
Tofacitinib (bradycardic effect)
Increases risk of adverse or toxic effects of the following
drugs:
Lacosamide (AV-blocking effect), Moderate Risk QTc-
Prolonging Agents (QTc-prolonging effect), Pegvisomant
(significant elevations of liver enzymes)
Reduces therapeutic effect of Octreotide:
Quinolone Antibiotics e.g. Levofloxacin
Reduces therapeutic effect of Antidiabetic Agents
Avoid concomitant use with:
Decreases serum concentration of Cyclosporine (Systemic)
Increases risk of adverse or toxic effects of the following
drugs:
Ceritinib (bradycardic effect), Highest-Risk QTc-
Prolonging Agent (QTc-prolonging effect), Mifepristone
(QTc-prolonging effect)
Administration: Administer IV injections between meals to
decrease GI effects. May alter absorption of dietary fats.
Pregnancy Category: B
ATC Code: H01CB02
Rx SOMATOSTATIN
Inj.: 250 micrograms and 3 mg ampule / vial (IV, IV
infusion)
A cyclic tetradecapeptide that inhibits the release of human
growth hormone
Indication: Hemostatic medicines for esophageal varices
Contraindications: Pregnancy or breastfeeding (consult
specific product labeling)
Dose:
For esophageal varices bleeding, by IV bolus, ADULT, initially
250 micrograms over at least 1 minute, followed by
maintenance dose as continuous IV infusion at 250
micrograms/hour for 2–5 days, may repeat initial bolus
in first hour if hemorrhage is not controlled.
Dose Adjustment:
Renal Impairment:
For CrCl ≤30 mL/minute, administer 50% of the usual dose.
Precautions:
Glucose regulation; Insulin-dependent diabetes; Oliguria;
Cardiovascular disease (monitor vital functions closely,
especially following initial bolus injection).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-65-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
22
Adverse Drug Reactions: AV block, bradycardia,
hypertension, hypotension, hyperglycemia,
hypoglycemia, vertigo, flushing (rapid administration),
abdominal discomfort, diarrhea, nausea, vomiting
(infusion greater than 50 micrograms/minute),
bronchospasm, allergic reaction, severe water retention,
hyponatremia
Drug Interactions:
Monitor closely with:
Decreases metabolism of the following drugs:
Codeine [impairs formation of 2 major codeine
metabolites, morphine and norcodeine]
Increases risk of adverse or toxic effects of Somatostatin,
specifically, those associated with its hypoglycemic
effect:
Androgens [except Danazol], Antidiabetic Agents, Herbs
with Hypoglycemic Properties, MAO Inhibitors, Other
Hypoglycemia-associated Agents, Pegvisomant,
Quinolone Antibiotics Levofloxacin, Salicylates, Selective
Serotonin Reuptake Inhibitors
Increases serum concentration of the following drugs:
Bromocriptine (delays Bromocriptine absorption and
time to maximum plasma concentrations)
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Pegvisomant (significant elevations
of liver enzymes)
Avoid concomitant use with:
Decreases metabolism of Cyclosporine (Systemic)
Increases risk of adverse or toxic effects of Barbiturates e.g.
Phenobarbital (sedative effects)
Administration: Administer IV bolus slowly over at least 1
minute, followed immediately by continuous infusion. If
infusion is interrupted for more than 3–5 minutes, re-
administer initial bolus dose to maintain continuous
treatment.
NOTE: Avoid abrupt discontinuation of therapy; decrease
infusion gradually for 24 hours before discontinuing.
Pregnancy Category: B
ATC Code: H01CB01
DRUGS USED IN DIABETES
INSULIN
GENERAL INFORMATION
Insulin is a polypeptide hormone of complex structure
produced by the pancreas that plays a key role in the
metabolism of carbohydrate, fat, and protein. All insulins
are developed by recombinant DNA technology but the
amino acid sequence of human and analogue insulins
differ. These explain the differences in pharmacokinetics
between human and analogue insulins.
Mode of Action: Increase or restore ability to metabolize
glucose by enhancing cellular glucose uptake; inhibit
endogenous glucose output and lipolysis.
Types of Insulin: The various formulations of insulin are
classified according to their duration of action after
subcutaneous injection, as: short-acting and rapid-acting
insulins, intermediate-acting insulins, and long-acting
insulins and ultra- long acting insulins. The intermediate-
acting and long-acting insulins are given for the basal
requirements, while the short-acting and rapid-actin
insulins are given before meals to control post-prandial
hyperglycemia.
Indications:
Management of type 1 diabetes mellitus; type 2 diabetes
mellitus inadequately controlled with diet, exercise, and
oral antidiabetic medications, and where oral therapy
cannot be used (e.g., during surgery, or in pregnant
women with Type 2 DM when diet alone fails to control
the diabetes), children with diabetes; diabetic
emergencies (e.g. diabetic ketoacidosis and
hyperosmolar hyperglycemic states).
Contraindications: Hypoglycemia
Dose:
Dose of insulin and regimen depend on the individual
treatment endpoints and are adjusted according to
(capillary) blood glucose monitoring.
Dose of human insulin is always expressed in units. Do NOT
abbreviate the word “unit.” One unit of human insulin,
which is contained in 0.03846 mg of the first
International Standard (1986) is equivalent to the
amount of insulin required to reduce the concentration
of blood glucose to 45 mg/dL in a fasting rabbit.
NOTE: Diabetes self-management education (DSME) is
essential to maximize the effectiveness of therapy.
Dose Adjustment:
Renal Impairment:
In mild-to-moderate impairment, reduce dose.
In severe impairment, refer to a specialist.
CrCl 10–50
mL/minute
Administer at 75% of normal dose
and monitor glucose closely
CrCl <10
mL/minute
Administer at 25% to 50% of normal
dose and monitor glucose closely](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-66-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
23
Hepatic Impairment:
Insulin requirements may be decreased in patients with
hepatic impairment.
Precautions:
Acute illness or conditions, e.g., trauma,
Myocardial Infarction;
Infections;
Stroke;
Coma;
Infections;
Diabetic ketoacidosis
Surgery;
Renal impairment;
Exercise;
Pregnancy
SKILLED TASKS. Driving may be hazardous when
hypoglycemic since awareness is impaired. Check blood
glucose concentration before driving, and at intervals of
approximately 2 hours when on long journeys.
MONITORING: The facility should have monitoring at the
point of care. Blood glucose concentration varies
throughout the day. Diabetes patients should aim to
maintain their blood glucose concentration between 4–
9 mmol/L for most of the time [ideally, 80-130 mg/dL
(4–7 mmol/L before meals and <180 mg/dL (<9
mmol/L) after meals]. Prevent blood glucose
concentration from falling below 72mg/dL (4 mmol/L)
because of the risk of hypoglycemia. Glycated
hemoglobin concentration (HbA1c) should be <7% (53
mmol/L).
STABILITY and STORAGE: Insulin preparations should be
stored in a refrigerator at 2–8oC, protected from light and
not allowed to freeze. Patients should be advised not to
expose their vials or cartridges to excessive heat or
sunlight.
Adverse Drug Reactions:
Common: Hypoglycemia
Less Common: Edema, lipodystrophy (either as lipoatrophy
or lipohypertrophy) at the site of injection, weight gain.
Rare: Localized reactions (e.g., redness, swelling, itching),
generalized hypersensitivity reactions (including rash
over the whole body, shortness of breath, wheezing,
hypotension, tachycardia, sweating, or very rarely,
anaphylactic reactions).
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Insulin:
ACE Inhibitors, e.g., Enalapril, Beta Blockers, e.g.,
Atenolol, Propranolol (hypoglycemic effect), Alcohol
(inhibits hepatic glucose output; decreases blood
glucose concentratin)
Increases risk of adverse effects of Insulin:
Alcohol (hypoglycemia; masks warning symptoms), Beta
Blockers, e.g., Atenolol, Propranolol (masks warning
signs of hypoglycemia), Drugs increasing blood glucose
concentration, e.g., Glucocorticoids, Antipsychotics,
Calcineurin Inhibitors, High-dose Thiazide Diuretics
(alters diabetes control of insulin)
Nifedipine (impairs glucose tolerance),
Thiazolidinediones (increases risk of edema and heart
failure)
Reduces therapeutic effect of Insulin:
Drugs increasing blood glucose concentration, e.g.,
Glucocorticoids, Antipsychotics, Calcineurin Inhibitors,
High-dose Thiazide Diuretics
Avoid concomitant use with:
Reduces therapeutic effect of Insulin:
Contraceptives, Oral, e.g., Levonorgestrel,
Medroxyprogesterone (Corticosteroids, e.g.,
Dexamethasone, Hydrocortisone, Prednisolone;
Diuretics, e.g., Furosemide, Hydrochlorothiazide)
Administration: Administered via injection because it is
easily inactivated by the body enzymes.
The SC route is ideal in most situations, usually injected
in the upper arms, thighs, buttocks, or abdomen. The
rate of absorption from different sites may vary
depending on local blood flow (absorption in the arm is
faster than in the buttock or thigh).
Do NOT administer mixtures of insulin formulations
intravenously.
Rx
REGULAR INSULIN
(RECOMBINANT DNA, HUMAN)
Inj.: 100 IU/mL, 3 mL pre-filled syringe (SC, IV/IM)
100 IU/mL, 5 mL and 10 mL vial (SC, IV/IM)
A short-acting, regular crystalline zinc insulin, which is
prepared as a sterile, clear aqueous solution. It contains
a polypeptide hormone structurally identical to the
human insulin synthesized through rDNA technology for
treatment of diabetes.
Regular or soluble insulin is the most appropriate form of
insulin for use in diabetic emergencies and during
surgery, and in these cases, are typically given in an
intravenous infusion (insulin drip). When injected IV, it
has a very short half-life of only about 5 minutes and its
effect disappears within 30 minutes.
Indications: Management of diabetes mellitus; diabetic
ketoacidosis.
Dose:
Diabetes mellitus, by SC, IM, IV injection or IV infusion (IV
route is reserved for urgent treatment, e.g., DKA and for
fine control in serious illness and peri-operatively),
according to requirements. [see under Insulin and
Analogues].
Administration: Shake the suspension gently before
withdrawing a dose. Do NOT use if solution is viscous or
cloudy. Use only if clear and colorless. Follow
manufacturer’s instructions.
See General Information on Insulin and Analogues listed
above for further information.
Pregnancy Category: B](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-67-320.jpg)


![A
ALIMENTARY TRACT AND METABOLISM
26
Drug Interactions:
Monitor closely with:
Enhances adverse effect of the following drugs:
Alcohol (flushing reaction; decreases blood glucose
concentration), Beta Blockers [except Levobunolol,
Metipranolol] (may mask symptoms of hypoglycemia),
Carbocisteine (may enhance adverse effects of alcohol
present in liquid formulations), Porfimer, Verteporfin
(photosensitizing effect)
Enhances hypoglycemic effect of Gliclazide:
Alcohol (masks warning symptoms, Alpha-Lipoic Acid;
Androgens [except Danazol]; Antidiabetic Agents; Beta
Blockers [except Levobunolol, Metipranolol]; Cyclic
Antidepressants; Fibric Acid Derivatives
Hypoglycemia-associated Agents; MAO Inhibitors;
Miconazole; Pegvisomant
Quinolone Antibiotics; Salicylates; SSRIs; Sulfonamide
Derivatives; Vitamin K Antagonists, e.g., Warfarin
Enhances therapeutic effect Vitamin K Antagonists, e.g.,
Warfarin (anticoagulant effect)
Increases risk of adverse or toxic effects of Gliclazide:
Dexketoprofen
Reduces therapeutic effect of Gliclazide:
Corticosteroids, systemic, Hyperglycemia-associated
Agents, Loop Diuretics (hypoglycemic effect), Quinolone
Antibiotics (loss of blood sugar control may occur),
Thiazide Diuretics
Avoid concomitant use with:
Decreases serum concentration of Gliclazide:
CYP2C9 Inducers, Dabrafenib, Rifampin
Enhances hypoglycemic effect of Gliclazide:
DPP-IV Inhibitors, Glucagon-like Peptide-1 Agonists /
GLP1 Agonists, Sodium Glucose Cotransporter Inhibitors
/ SGLT2 Inhibitors (consider dose reduction of
gliclazide), Thiazolidinedione
Increases risk of adverse or toxic effects of Gliclazide:
CYP2C9 Inhibitors, Fluconazole, (hypoglycemia)
Increases risk of adverse or toxic effects of Mecamylamine
Increases serum concentration of Gliclazide:
CYP2C9 Inhibitors, Fluconazole, Mifepristone (monitor
closely for adverse effects, during and in the 2 weeks
following mifepristone treatment)
Reduces therapeutic effect of Gliclazide:
Dabrafenib, Rifampin
Administration:
Take immediate-release tablets before meals.
Take MR tablets with food to minimize the risk of
hypoglycemia.
Pregnancy Category: C
ATC Code: A10BB09
VITAMINS
MULTIVITAMINS, PLAIN
OTC MULTIVITAMINS
Oral:
For infants, drops, per 1 mL contains:
Vitamin A 325–380 micrograms RE
Vitamin B1 0.2–0.4 mg
Vitamin B2 0.3–0.4 mg
Vitamin B6 0.3–0.6 mg
Vitamin B12 0.3–0.4 micrograms
Vitamin C 30 mg
Vitamin D 200 – 400 IU (5 - 10 micrograms)
Vitamin E 3–4 mg
Folic Acid 20–65 micrograms
Niacin 1–5 mg
For children, syrup, per 5 mL contains:
Vitamin A 350–400 micrograms RE
Vitamin B1 0.5–1.0 mg
Vitamin B2 0.7–0.9 mg
Vitamin B6 0.9–1.6 mg
Vitamin B12 0.9–3.0 micrograms
Vitamin C 35–55 mg
Vitamin D 200 – 400 IU (5 - 10 micrograms)
Vitamin E 5–7 mg
Folic Acid 40–300 micrograms
Niacin 5–18 mg
For adults, tablet or capsule, each tablet / capsule contains:
Vitamin A 600–700 micrograms RE
(2000 – 2500 IU)
Vitamin B1 1.3–1.7 mg
Vitamin B2 0.7–1.3 mg
Vitamin B6 1.6–2 mg
Vitamin B12 2–6 micrograms
Vitamin C 60–80 mg
Vitamin D 400 IU (10 micrograms)
Vitamin E 6–10 mg (15 – 30 IU)
Folic Acid 400 micrograms
Niacin 13–23 mg
A dietary supplement containing essential multivitamins
and minerals that are needed for good health, growth,
and development.
Indications: Dietary supplementation, management of
vitamin deficiencies
Contraindications: Known hypersensitivity to any
component of the preparations
Dose:
Prevention or treatment of vitamin deficiencies, by mouth,
ADULT, 1 tablet or capsule daily.
Precautions:
Avoid taking similar vitamin products.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-70-320.jpg)

![A
ALIMENTARY TRACT AND METABOLISM
28
Calcitriol is readily absorbed from the intestine.
Absorption can be delayed in patients with hepatic,
biliary, or GI disease.
Pregnancy Category: C
ATC Code: A11CC04
Rx RETINOL (VITAMIN A)
Oral: 10,000 IU, 25,000 IU, and 50,000 IU soft gel capsule
(as palmitate)
100,000 IU and 200,000 IU soft gel capsule with
nipple (as palmitate) [only for DOH program]
A fat-soluble vitamin and dietary supplement that is
required by the eyes for the transduction of light into
neural signs necessary for vision.
Indications: For the prevention and treatment of vitamin A
deficiency states (e.g., xerophthalmia and night
blindness); prevention of complications of measles.
Contraindications: Hypervitaminosis A; known
hypersensitivity to vitamin A, or any component of the
formulation; dosages exceeding the Recommended
Energy and Nutrient Intake (RENI); women who are, or
may become, pregnant.
Dose:
Prevention of vitamin A deficiency (universal or targeted
distribution programs), by mouth, ADULT, 200,000 IU
every 6 months; ADULT (pregnant woman), maximum of
10,000 IU daily or maximum 25,000 IU weekly; ADULT
(woman of childbearing age), 200,000 IU at delivery or
within 8 weeks of delivery; CHILD >1 year (preschool),
200,000 IU every 4–6 months; INFANT 6–12 months,
100,000 IU every 4–6 months, preferably at measles
vaccination; INFANT <6 months, 50,000 IU. [NOTE:
Administer an additional dose the next day in
hospitalized children with measles infection.]
Treatment of xerophthalmia, by mouth, ADULT (except
woman of childbearing age) and CHILD >1 year, 200,000
IU on diagnosis, repeated the next day and again after 2
weeks; ADULT (woman of childbearing age with severe
signs of xerophthalmia), as for other adults; ADULT
(woman of childbearing age with less severe symptoms,
e.g., night blindness), either 5,000 to 10,000 IU daily for
at least 4 weeks or up to 25,000 IU weekly; INFANT 6–
12 months, 100,000 IU immediately on diagnosis,
repeated the next day and again after 2 weeks; INFANT
under 6 months, 50,000 IU on dis, repeat the next day
and again after 2 weeks. [NOTE: Oral vitamin A
preparations are preferred for the prevention and
treatment of vitamin A deficiency.]
Dose Adjustment:
Pregnant women susceptible to vitamin A deficiency during
the third trimester:
Should be given low dose vitamin A supplements on a daily
or weekly basis.
Precautions:
WARNING: Severe congenital malformations may occur
in infants of mothers consuming large amounts of
oral retinoids for acne treatment.
Patients on prolonged daily administration over 25,000 IU
should be under close supervision;
Chronic intake of vitamin A at levels 10–20 times the RDA
can lead to hypervitaminosis A;
Pregnancy (excessive doses during the first trimester may
be teratogenic);
Breastfeeding (there is theoretical risk of toxicity in infants
of mothers taking large doses).
NOTE: Dietary reference intakes (DRIs): Tolerable upper
intake level (UL) for adults is 3,000 micrograms daily of
preformed vitamin A, based on teratogenicity as the
critical adverse effect for women of childbearing age and
liver pathology for all other adults.
Adverse Drug Reactions:
Less Common: Diplopia, headache, nausea, symmetric
papilledema, vomiting
Rare: Birth defects (e.g., tense and bulging fontanelle in
infants), dry hair, enlarged liver, increased intracranial
pressure
Drug Interactions:
Monitor closely with:
Increases therapeutic effect of Warfarin (anticoagulant
effect)
Avoid concomitant use with:
Decreases absorption of Retinol:
Bile Acid–binding Resins, e.g., Cholestyramine,
Colestipol
Increases risk of adverse or toxic effects of the following
drugs:
Retinoid Drugs, e.g., Acitretin, All-trans-retinoic Acid,
Isotretinoin (hypervitaminosis A); Tetracyclines (benign
intracranial hypertension)
Administration: This vitamin is absorbed along with fat in the
diet. Take it with food.
Pregnancy Category: A; X if dose is greater than RENI
ATC Code: A11CA01](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-72-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
29
VITAMIN B1, PLAIN AND IN COMBINATION WITH
VITAMIN B6 AND B12
(Oral) OTC
(Inj.) Rx
THIAMINE (VITAMIN B1)
Oral: 100 mg and 300 mg tablet (as hydrochloride)
Inj.: 100 mg/mL, 1 mL ampule / vial (IV)
100 mg/mL, 10 mL vial (as hydrochloride) (IM, IV)
A water-soluble vitamin found in yeast, cereal grains,
legumes, peas, nuts, pork, and beef. It is used to prevent
peripheral neuritis associated with pellagra (Vitamin B3
deficiency) and pregnancy. It combines with adenosine
triphosphate (ATP) to form thiamine pyrophosphate, an
essential coenzyme in carbohydrate metabolism.
Indications: Management of beriberi (Vitamin B1 deficiency,
maple syrup urine disease (MSUD) and Wernicke /
Korsakoff syndrome; nutritional supplementation.
Contraindications: Breast-feeding; encephalopathy;
pregnancy
Dose:
Nutritional supplementation, by mouth, ADULT and
ADOLESCENT (pregnant or lactating female), 1.4 mg
daily; ADULT and ADOLESCENT (male), 1.2 mg daily;
ADULT (female), 1.1 mg daily; ADOLESCENT (females), 1
mg daily; CHILD 9–13 years, 0.9 mg daily; CHILD 4-8
years, 0.6 mg daily; CHILD 1–3 years, 0.5 mg daily;
INFANT 7–12 months, 0.3 mg daily; INFANT 0–6 months,
0.2 mg daily.
Prevention of thiamine deficiency in patients receiving total
parenteral nutrition (TPN), by IV injection, ADULT, 3 mg
daily admixed with TPN.
Beriberi, by mouth, ADULT, 5–30 mg once daily or in 3
divided doses for 1 month; CHILD and INFANT, 10–50
mg once daily for 2 weeks, then 5-10 mg once daily for 1
month;
by IV or IM injection, ADULT, initially 5–30 mg once daily
or in 3 divided doses, then convert to oral route once
patient is taking PO (total treatment duration, 1 month);
CHILD and INFANT, 10–25 mg daily for 2 weeks, then 5–
10 mg once daily for 1 month. [NOTE: If beriberi occurs
in a breast-fed infant, both lactating mother and infant
should receive treatment.]
Wernicke/Korsakoff Syndrome, by IV or IM injection, ADULT,
initially 100 mg, followed by 50–100 mg daily until
normal dietary intake is established (clinical practice
guidelines recommend 200–500 mg 3 times daily for 5–
7 days or until there is no further improvement in
symptoms).
Metabolic disorders including necrotizing
encephalomyelopathy, maple syrup urine disease
(MSUD), and lactic acidosis associated with pyruvate
carboxylase deficiency, by mouth, ADULT, 10–20 mg
daily as a single dose, up to 4 g daily in divided doses.
Precautions:
WARNING: Serious hypersensitivity or anaphylactic
reactions can occur, especially after repeated
administration.
Hepatic impairment; Lactation (not known if excreted in
breastmilk).
Adverse Drug Reactions:
Common: Sneezing, pruritus (generalized), warmth,
urticaria, weakness, diaphoresis, nausea, restlessness,
tightness of throat, angioedema, cyanosis, pulmonary
edema, GI bleeding, injection site reaction
Rare: Hypersensitivity reactions
Drug Interactions:
Avoid concomitant use with:
Decreases serum concentration of Thiamine:
Ethyl Alcohol, Chronic Consumption (results in deficiency
of several nutrients)
Administration:
For oral administration, may be taken without regards to
meals.
Parenteral administration is reserved for patients for
which oral thiamine is not feasible.
Inspect visually for particulate matter and discoloration
prior to administration.
For slow IV push, no dilution is necessary.
For continuous IV infusion, dilute thiamine in a
compatible infusion solution. Administer at a rate
prescribed by the physician.
Pregnancy Category: A
ATC Code: A11DA01
(Oral) OTC
(Inj.) Rx
VITAMIN B1 B6 B12
Oral: 100 mg B1 + 5 mg B6 + 50 micrograms B12 per tablet
/ capsule
10 mg B1 + 5 mg B6 + 5 micrograms B12 per 0.6 mL
drops, 15 mL
Inj.: 100 mg B1 + 100 mg B6 + 1 mg B12 per 3 mL, ampule
(IV)
100 mg B1 + 100 mg B6 + 1 mg B12 per mL, 10 mL
vial (IV)
A dietary supplement, which contains vitamins B1, B6, and
B12 for nerve cell metabolism, and for vitamin B-complex
deficiencies.
Indications: Prevention and treatment of vitamin B complex
deficiencies; adjunct in the management of
neuromuscular pain responsive to vitamin B1, B6, and
B12, including neuralgia, neuritis and neuropathies.
Contraindications: Leber’s disease or tobacco amblyopia;
known hypersensitivity to any component of the
formulation.
Dose:
Prevention and treatment of vitamin B complex deficiency,
by mouth, ADULT, 1–2 tablets or capsules daily; by slow
IV injection, ADULT, 0.25–2 mL.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-73-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
30
Precautions:
Vitamin B12 >10 micrograms daily may produce
hematological response in folic acid deficiency.
Neurotoxicity (long-term administration of large doses >2 g
daily)
Malabsorption; Anemia; Neuropathy; Undiagnosed vitamin
B12 deficiency.
Adverse Drug Reactions:
Less Common: Headache, peripheral neuropathy (high
doses)
Rare: Hypersensitivity reactions
Drug Interactions:
Avoid concomitant use with:
Decreases therapeutic effect of Levodopa
Administration:
For oral administration, may be taken with or without
food. May be taken with meals to reduce GI discomfort.
High concentration IV solutions may be diluted using
parenteral infusion solutions
Pregnancy Category: A; C (doses greater than RENI)
ATC Code: A11DB
ASCORBIC ACID (VITAMIN C)
OTC ASCORBIC ACID (VITAMIN C)
Oral: 100 mg and 500 mg tablet
100 mg/mL drops, 15 mL and 30 mL
100 mg/5 mL syrup, 60 mL and 120 mL
Inj.: 250 mg/mL, 2 mL ampul (IV)
A water-soluble vitamin that acts as a free radical, an
antioxidant scavenger, and plays a major role in
oxidation-reduction reactions. Ascorbic acid is a cofactor
for enzymes involved in the biosynthesis of collagen,
carnitine, and neurotransmitters.
Indications: Nutritional supplementation; management of
iron toxicity, scurvy and furunculosis
Contraindications: Anemia, breastfeeding, diabetes
mellitus, G6PD deficiency, hemochromatosis,
nephrolithiasis, pregnancy, sideroblastic anemia,
sodium restriction, sulfite hypersensitivity, tartrazine dye
hypersensitivity, thalassemia
Dose:
Nutritional supplementation, by mouth, ADULT (male), 90
mg once daily, or 100 mg once or twice daily; ADULT
(female), 75 mg once daily, or 100 mg once or twice
daily; ADULT and ADOLESCENT (pregnant female), 80-85
mg once daily; ADULT and ADOLESCENT (lactating
female), 115–120 mg once daily; ADULT (male
smokers), 125 mg once daily; ADULT (female smokers),
110 mg once daily; ADOLESCENT (male), 75 mg once
daily; ADOLESCENT (female), 65 mg once daily; CHILD 9–
13 years, 45 mg once daily; CHILD 4–8 years, 25 mg
once daily; CHILD 1–3 years, 15 mg once daily; INFANT,
40–50 mg once daily.
Scurvy, by mouth, ADULT, 100–250 mg 1–2 times daily;
CHILD, 100–300 mg daily in divided doses; INFANT, 50–
100 mg daily in divided doses.
Adjunct to deferoxamine therapy in the treatment of chronic,
iron toxicity, by mouth, ADULT, 100–200 mg once daily
initiated 1–2 hours after deferoxamine infusion is
started.
Chronic recurrent furunculosis in patients with neutrophil
dysfunction, by mouth, ADULT, 1,000 mg daily for 4–6
weeks [NOTE: Studies show that ascorbic acid does not
alter the course of furunculosis in patients without
neutrophil dysfunction].
Dose Adjustment:
Renal Impairment:
Removed by hemodialysis. Adjust dosing accordingly.
For patients receiving intermittent hemodialysis, doses
greater than 200 mg daily are not recommended.
Precautions:
Heart failure (do not administer concurrently with
deferoxamine without approval of their health care
professional);
Hyperoxaluria;
Renal impairment;
Lactation
Adverse Drug Reactions:
Common: Renal tubular obstruction (oxalate, urate, or
cystine renal stones), lower back pain (costovertebral),
hyperoxaluria, flushing, headache, nausea, vomiting,
abdominal cramps, diarrhea, flatulence, heartburn,
dental caries (chewable tablets), fatigue, insomnia,
sleepiness
Less Common: Hemolytic anemia
Rare: Sickle-cell crisis
Drug Interactions:
NOTE: Decreases urine pH, which may cause an increase in
the excretion of alkaline drugs and an increase in renal
tubular reabsorption of acidic compounds.
Monitor closely with:
Decreases therapeutic effect of the following drugs:
Mexiletine;
Propranolol [take ascorbic acid at least 1 hour prior to
propranolol] (bradycardic effect)
Increase absorption of the following drugs:
Iron Salts, Polysaccharide-Iron Complex
Avoid concomitant use with:
Decreases therapeutic effect of the following drugs:
Disulfiram; Warfarin (anticoagulation effects)
Increases risk of adverse or toxic effects of the following
drugs:
Deferoxamine (e.g., impairment of cardiac function,
causing cardiac decompensation)
Administration: May be taken without regard to meals.
Administer with a full glass of water.
Pregnancy Category: C](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-74-320.jpg)


![A
ALIMENTARY TRACT AND METABOLISM
33
Vitamin B6 deficiency including neuritis (not drug-induced),
by mouth, ADULT (without neuritis), 2.5-10 mg daily; may
be adjusted to 2-5 mg daily once deficiency has been
corrected; ADULT (with neuritis), 100-200 mg daily for 3
weeks, then 25-100 mg daily thereafter; CHILD (without
neuritis), 5-25 mg daily for 3 weeks, then 1.5-2.5 mg
daily (may be supplemented in a multivitamin product);
CHILD (with neuritis), 10-50 mg daily for 3 weeks, then
1-2 mg daily (may be supplemented in a multivitamin
product.
Sideroblastic anemia, by mouth, ADULT, 200-600 mg daily;
following an adequate response, 30-50 g daily may be
used.
Selected metabolic disorders, including primary
cystathioniuria, primary homocystinuria, or xanthurenic
aciduria, by mouth, ADULT, 100 to 500 mg daily or more,
adjusted to clinical response; CHILD, 200-1000 mg daily,
adjusted to clinical response.
Primary hyperoxaluria, in combination with oral
orthophosphate therapy, by mouth, ADULT and CHILD,
initially 1.8-7 mg/kg daily with a final dose of 1-7 mg/kg
daily.
Premenstrual syndrome (PMS), by mouth, ADULT, 80-500
mg daily.
Pregnancy-induced nausea / vomiting, by mouth, ADULT,
10-25 mg 3 times daily; ADOLESCENT, 25-100 mg daily;
CHILD, 1-2 mg daily.
Pyridoxine-dependent seizures, maintenance, by mouth,
CHILD, INFANT, and NEONATE, initially 5 mg/kg once or
divided twice daily; titrate as needed to suppress
seizures.
Precautions:
Seizures (associated with high-dose administration).
Adverse Drug Reactions:
Common: Nausea, vomiting, headache, paresthesia,
hyperesthesia, somnolence, low serum folic acid levels,
peripheral neuropathy.
Less Common: Neuronopathy syndrome, unstable gait,
perioral numbness, “stocking-globe” sensory loss,
seizures, metabolic acidosis.
Drug Interactions:
Monitor closely with:
Decreases therapeutic effect of Pyridoxine:
Cycloserine (secondary niacin deficiency)
Decreases therapeutic effect of Levodopa
Avoid concomitant use with:
Not to be administered concomitantly without consent of
healthcare provider:
Altretamine, Cisplatin
Administration: Administer whole. Do not crush, break, or
chew.
Pregnancy Category: A
ATC Code: A11HA02
MINERAL SUPPLEMENTS
CALCIUM
GENERAL INFORMATION
An essential cation for the maintenance of the nervous,
muscular, and skeletal systems, as well as for cell
membrane and capillary permeability. It is the primary
component of skeletal tissue, providing structural
integrity and support for individual growth.
Indications: Cardiac arrest; cardiopulmonary resuscitation;
exchange transfusion-induced hypocalcemia
prophylaxis; hyperkalemia; hypermagnesemia;
hyperphosphatemia; hypocalcemia; nutritional
supplementation; osteoporosis prophylaxis.
Contraindications: Breastfeeding; cardiac arrhythmias;
dehydration; digitalis toxicity; extravasation;
hypercalcemia; hypercalciuria; necrotizing enterocolitis;
hyperphosphatemia; hypoparathyroidism; pregnancy;
sarcoidosis; ventricular fibrillation; diarrhea; vitamin D
toxicity.
Dose Adjustment:
Renal Impairment:
In end-stage renal disease, administer with meals (e.g., 10–
15 minutes before or during).
Adverse Drug Reactions:
Common: Mild to severe local irritation, chalky taste,
flushing, tingling sensation, hypotension (dizziness,
syncope), sinus bradycardia, cardiac arrhythmias,
cardiac arrest, diarrhea, gastric irritation.
Less Common: Milk-alkali syndrome, muscle cramps
Drug Interactions:
Monitor closely with:
Decreases absorption of Calcium:
Corticosteroids
Decreases absorption of the following drugs:
Dibasic Sodium Phosphate, Anhydrous, Monobasic
Sodium Phosphate, Monohydrate, Phenytoin (forms non-
absorbable complexes), Phosphorus Salts, Strontium-89
Chloride
Decreases therapeutic effect of Magnesium Salts
(neutralized by Calcium)
Increases risk of adverse or toxic effects of the following
drugs:
Calcitriol (hypercalcemia), Vitamin D Analogs (Vitamin D-
induced hypercalcemia)
Avoid concomitant use with:
Decreases absorption of Bisphosphonates e.g. Alendronate
(administer at least 2 hours apart)
Decreases bioavailability of the following drugs:
Fluoroquinolones e.g., Levofloxacin, Quinolones
[administer at least 2 hours before or 6 hours after
Calcium Salts], Tetracyclines [administer at least 1 hour](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-77-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
34
before Calcium Salts], Thyroid Hormones [administer at
least 4 hours before or after Calcium Salts] (forms non-
absorbable complexes)
Decreases therapeutic effect of Calcium:
Vitamin A
Decreases therapeutic effect of the following drugs:
Calcitonin, Nondepolarizing Neuromuscular Blockers,
Sucralfate [stagger doses], Thyroid Hormones
(hypothyroidism)
Increases risk of adverse effects of Calcium:
Vitamin A (bone loss)
Increases risk of adverse effects of the following drugs:
Cardiac Glycosides e.g., digoxin (arrhythmias),
Ceftriaxone (fatal reactions involving ceftriaxone-
calcium precipitates in the lungs and kidneys), Sodium
Bicarbonate, Thiazide Diuretics (milk-alkali syndrome),
Pregnancy Category: C
OTC CALCIUM CARBONATE
Oral: tablet or chewable tablet (equivalent to 500 mg and
600 mg elemental calcium)
An inorganic Calcium salt useful in the treatment of
hyperphosphatemia secondary to chronic renal failure.
Indications: Management of hyperphosphatemia,
hypocalcemia, and premenstrual syndrome (PMS);
nutritional supplementation; prevention of osteoporosis.
Contraindications: Breastfeeding; constipation;
dehydration; GI bleeding; GI obstruction; hypercalcemia;
hyperparathyroidism; ileus; hypercalciuria; necrotizing
enterocolitis; neoplastic disease; nephrolithiasis; peptic
ulcer disease; pregnancy; renal disease; sarcoidosis.
Dose:
Oral hypocalcemia, by mouth, ADULT, 5–10 g daily
(equivalent to 2–4 g elemental calcium), given in 3–4
divided doses; CHILD, 112.5–162.5 mg/kg daily
(equivalent to 45–65 mg/kg), given in 4 divided doses;
NEONATE, 125–375 mg/kg daily (equivalent to 50–150
mg/kg), given in 4–6 divided doses (maximum dose, 1 g
daily).
Nutritional supplementation and prevention of
osteoporosis, by mouth, ADULT ≥51 years, 2,500–3,750
mg daily (equivalent to 1,000 to 1,500 mg elemental
calcium); ADULT 19–50 years, 2,500 mg daily
(equivalent to 1,000 mg elemental calcium);
ADOLESCENT and CHILD 9–18 years, 3,250 mg daily
(equivalent to 1,300 mg elemental calcium); CHILD 4–8
years, 2,000 mg daily (equivalent to 800 mg elemental
calcium); CHILD 1–3 years, 1,250 mg daily (equivalent
to 500 mg elemental calcium); INFANT 6–12 months,
equivalent to 270 mg elemental calcium, based on total
intake; INFANT <6 months and NEONATE, equivalent to
210 mg elemental calcium, based on total intake.
Dose Adjustment:
Renal Impairment:
In CrCl <30 mL/min, use with caution.
Precautions:
Renal impairment;
Hypoparathyroid disease;
Hypercalcemia-associated diseases;
Achlorhydria;
History of kidney stones.
Adverse Drug Reactions:
Common: Gastric hypersecretion, acid rebound, flatulence,
gastric distention, constipation, eructation
Less Common: Hypercalcemia, nephrolithiasis, milk-alkali
syndrome, renal failure
Rare: Hypophosphatemia
Drug Interactions:
Monitor closely with:
Decreases absorption of Calcium:
Corticosteroids, systemic
Increases risk of adverse effects of the following drugs:
Calcipotriene, Calcitriol (hypercalcemia), Mefloquine,
Thiazide Diuretics (hypercalcemia), Vitamin D Analogues
(Vitamin D-induced hypercalcemia)
Avoid concomitant use with:
Decreases absorption of the following drugs:
Bisacodyl [administer at least 1 hour apart]
Bisphosphonates e.g., Alendronate [administer at least 2
hours apart]
Decreases absorption of the following drugs:
Cefuroxime, oral [administer at least 1 hour before or 2
hours after Calcium Carbonate]
Delavirdine [administer at least 1 hour apart]
Ethotoin [administer Calcium Carbonate at least 1 hour
before or 6 hours after Ethotoin]
Itraconazole [administer at least 2 hours after
Itraconazole]
Ketoconazole, Oral [administer at least 2 hours after
Ketoconazole]
Phenytoin, oral [administer Calcium Carbonate at least 1
hour before or 6 hours after Phenytoin]
Rifampin [administer at least 1 hour apart]
Decreases bioavailability of the following drugs:
Fluoroquinolones e.g., Levofloxacin [administer at least
2 hours before or 6 hours after Calcium Salts],
Quinolones [administer at least 2 hours before or 6 hours
after Calcium Salts], Tetracyclines [administer at least 1
hour before Calcium Salts], Thyroid Hormones
[administer at least 4 hours before or after Calcium
Salts] (forms non-absorbable complexes)
Decreases serum concentration of the following drugs:
Ezetimibe and Rosuvastatin [administer at least 1 hour
before or 2 hours after Calcium Carbonate]
Gefitinib [administer at least 6 hours apart]
Decreases therapeutic effect of Calcium:
Vitamin A](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-78-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
35
Decreases therapeutic effect of the following drugs:
Calcitonin, Cefuroxime (decrease antibiotic efficacy),
Methenamine, Sucralfate [stagger doses], Thyroid
Hormones (leads to hypothyroidism)
Decreases urinary excretion of Quinidine
Increases risk of adverse effects of Calcium:
Vitamin A (bone loss)
Increases risk of adverse effects of the following drugs:
Cysteamine [administer at least 1 hour apart] (increased
WBC cystine concentration)
Sodium Bicarbonate (milk-alkali syndrome)
Not to be use concomitantly with Calcium Carbonate:
Ammonium Chloride
Administration: Administer with meals to improve
absorption. Follow each dose with appropriate fluid
intake.
Separate administration with other medicines to prevent
interactions.
Pregnancy Category: C
ATC Code: A12AA04
Rx CALCIUM GLUCONATE (IV)
Inj.: 10% solution, 10 mL ampule (IV)
10% solution, 20 mL and 25 mL bottle (IV)
An organic Calcium salt used to prevent or treat negative
calcium balance. It also helps facilitate nerve and muscle
performance as well as normal cardiac function.
Indications: Hypocalcemia; hyperkalemia;
hypermagnesemia; nutritional supplementation.
Dose:
Hypocalcemia, by IV infusion, ADULT, 2-3 g slowly at a rate
not exceeding 5 mL/minute, repeat every 6 hours, as
needed (maximum dose, 15 g daily); alternatively, 15
mg/kg elemental calcium over 4–6 hours if symptoms
recur after initial IV calcium replacement; CHILD and
INFANT, 200 to 500 mg/kg daily as continuous IV
infusion or in 4 divided doses at a rate not exceeding 5
mL/minute; may be repeated after 6 hours or followed
by 500 mg/kg daily as continuous IV infusion or in 3–4
divided doses; NEONATE, 200–800 mg/kg daily as
continuous IV infusion or in 3–4 divided doses, followed
by 500 mg/kg daily as continuous IV infusion or in 3–4
divided doses.
Hyperkalemia, hypermagnesemia, and ionized
hypocalcemia, including life-threatening cardiac
arrhythmias, or during cardiopulmonary resuscitation
(CPR) associated with suspected or documented
hypermagnesemia, hyperkalemia, or ionized
hypocalcemia, by IV injection, ADULT, 500–800 mg of
10% solution (maximum dose, 3 g); CHILD and INFANT,
60–100 mg/kg (maximum dose, 3 g).
CNS depression due to hypermagnesemia, by slow IV
infusion, ADULT, 500–2,000 mg at a rate not exceeding
200 mg/minute (2 mL/minute of a 10% solution).
Nutritional supplementation to prevent hypocalcemia in
patients receiving total parenteral nutrition (TPN), by IV
injection, ADULT, 10–15 mEq daily admixed with TPN.
Exchange transfusion-induced hypocalcemia, prophylaxis,
by IV injection, NEONATE, 97 mg after each 100 mL of
citrated blood exchanged.
Precautions:
Impaired renal function; cardiac disease; hypercalcemia-
associated diseases, e.g., sarcoidosis.
Lactation (excreted in breastmilk; use with caution).
Administration: Administer by slow IV injection as a 10%
solution slowly through a small needle into a large vein
to avoid too rapid increase in serum calcium and
extravasation of calcium solution into the surrounding
tissue that may lead to tissue necrosis. Following IV
injection, the patient should remain recumbent for a
short time.
Visually inspect parenteral products for particulate
matter and discoloration prior to administration.
Close monitoring of serum calcium concentrations is
essential during IV administration of calcium.
Oral administration of calcium supplements or calcium-
rich foods should replace IV calcium therapy as soon as
possible.
NOTE: Do NOT administer by IM or SC route.
Closely monitor serum calcium concentrations during IV
administration of calcium.
Oral administration of calcium supplements or calcium-
rich foods should replace IV calcium therapy as soon as
possible.
See General Information on Calcium listed above for other
information.
ATC Code: A12AA03
OTC CALCIUM LACTATE
Oral: tablet (equivalent to 500 mg elemental calcium)
An organic Calcium salt used to prevent or treat negative
calcium balance. It also helps to prevent or reduce the
rate of bone loss, moderate nerve and muscle
performance and allow normal cardiac function.
Indications: Management of hypocalcemia; nutritional
supplementation
Dose:
Hypocalcemia, by mouth, ADULT, 15.4–30 g daily divided
every 8 hours; CHILD, 345–500 mg/kg daily in divided
doses every 6–8 hours (maximum dose, 9 g daily);](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-79-320.jpg)


![A
ALIMENTARY TRACT AND METABOLISM
38
ZINC
GENERAL INFORMATION
An essential, mineral supplement in the diet, which is used
as an adjunct to oral rehydration in the treatment of
acute and persistent diarrhea.
Indication: Adjunct to oral rehydration therapy in acute and
persistent diarrhea
Contraindication: Severe renal impairment
Precaution:
Acute renal failure (may accumulate).
Adverse Drug Reactions:
Common: Diarrhea, dry mouth, dyspepsia, GI upset, mouth
irritation, nausea, regurgitation and vomiting (in
children), unpleasant taste
Less Common: Gastritis, headache, irritability, lethargy,
copper deficiency (with prolonged use)
Drug Interactions:
Avoid concomitant use with:
Decreases absorption of Zinc:
Calcium Salts [separate doses by 2–3 hours],
Ethambutol, Ferrous Salts, Food, e.g., milk, phytates
present in cereals, rice, corn, or legumes
Decreases absorption of the following drugs:
Bisphosphonates e.g., Alendronate; Ferrous Salts e.g.,
Ferrous sulfate; Quinolones, e.g., Ofloxacin, Ciprofloxacin
[separate doses by at least 2 hours]; Tetracyclines
[separate administration by at least 2 hours]
Decreases therapeutic effect of the following drugs:
Tetracyclines (anti-infective activity)
Administration: Tablets may be dispersed in breastmilk, oral
rehydration solution, or water on a small spoon. Older
children may chew the tablets or swallow them with
water.
Pregnancy Category: C
OTC ZINC GLUCONATE
Oral: tablet (equivalent to 30 mg elemental zinc) (as
trihydrate)
chewable tablet (equivalent to 10 mg elemental zinc)
70 mg/5 mL syrup (equivalent to 10 mg elemental
zinc), 60 mL and 120 mL
Zinc gluconate is commonly used to treat and to prevent
zinc deficiency, as well as for other purposes.
Indication: Adjunct to oral rehydration therapy in acute and
persistent diarrhea
Dose:
Oral rehydration therapy in acute and persistent diarrhea
(adjunct), by mouth, CHILD 6 months to 5 years, 20 mg
(elemental zinc) daily for 10-14 days; INFANT <6 months,
10 mg (elemental zinc) daily for 10-14 days.
See General Information on Zinc listed above for other
information.
Pregnancy Category: C
ATC Code: A12CB02
OTC ZINC SULFATE
Oral: 88 mg dispersible tablet (equivalent to 20 mg zinc)
solution (equivalent to 10 mg elemental zinc/mL)
drops (as monohydrate), 15 mL
solution (equivalent to 20 mg elemental zinc/5 mL)
syrup (as monohydrate), 60 mL
Zinc sulfate is widely distributed in the body but is
concentrated in the muscle, bone, skin, and prostatic
fluids.
Indication: Adjunct to oral rehydration therapy in acute and
persistent diarrhea
Dose:
Oral rehydration therapy in acute and persistent diarrhea
(adjunct), by mouth, CHILD 6 months to 5 years, 20 mg
(elemental zinc) daily for 10-14 days; INFANT <6 months,
10 mg (elemental zinc) daily for 10-14 days.
See General Information on Zinc listed above for other
information.
Pregnancy Category: C
ATC Code: A12CB01
OTHER MINERAL PRODUCTS
OTC FERROUS SALT
Oral: tablet (equivalent to 60 mg elemental iron)
solution (equivalent to 15 mg elemental iron/0.6 mL)
drops, 15 mL and 30 mL
solution (equivalent to 30 mg elemental iron/5 mL)
syrup, 60 mL
NOTE: The elemental iron content of a ferrous salt depends on
the type of preparation as follows:
Ferrous fumarate 33%
Ferrous gluconate 12%
Ferrous lactate 19%
Ferrous sulfate, hydrated 20%
Ferrous sulfate, desiccated 32%
An essential trace element required for the formation of
hemoglobin and for the efficient oxygen transport in the
blood.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-82-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
39
Indications: Treatment of iron-deficiency anemia and
supplement and prophylaxis in people on hemodialysis
receiving erythropoietin.
Contraindications: Anemia not due to iron deficiency;
parenteral iron therapy; in patients receiving repeated
blood transfusions; hemochromatosis; hemosiderosis
Dose:
Iron-deficiency anemia, by mouth, ADULT, elemental iron,
100–200 mg daily in divided doses.
Prevention of iron-deficiency anemia (in those at risk), by
mouth, ADULT (woman), elemental iron 60 mg daily;
CHILD >5 years, elemental iron 30 mg daily; CHILD <5
years, elemental iron 2 mg/kg daily (maximum, 30 mg).
NOTE: For women and children >5 years, folic acid may also
be given.
Precautions:
WARNING: May exacerbate GI bleeding. Use with
caution in patients with GI disorders.
Not to be administered for longer than 6 months (monitor
closely for potential complications);
Transfusion-dependent anemia;
Peptic ulcer;
Regional enteritis;
Ulcerative colitis;
Intestinal strictures;
Diverticula;
Pregnancy (avoid use in the first trimester; administer only
in women with low-normal hemoglobin).
NOTE: In cases of overdose, initiate therapy with
deferoxamine. Before administration of deferoxamine,
the stomach should be emptied by gastric lavage (with a
wide-bore tube), preferable within one hour of ingesting
a significant quantity of iron or if radiography reveals
tablets in the stomach.
Adverse Drug Reactions:
Common: Abdominal pain, black discoloration of feces,
constipation, diarrhea, nausea, vomiting
Less Common: Black discoloration of teeth
Rare: Anaphylaxis, GI erosion and perforation,
hemosiderosis
Drug Interactions:
Monitor closely with:
Decreases bioavailability of Methyldopa (interferes with
blood pressure control)
Avoid concomitant use with:
Decreases absorption of Iron:
Antacids, e.g., Aluminum or Magnesium Hydroxide,
Calcium, Doxycycline, Food, e.g., eggs, milk,
Tetracyclines, Zinc Salts
Decreases absorption of the following drugs:
Bisphosphonates e.g., Alendronate, Doxycycline,
Levothyroxine [administer at least 2 hours apart],
Quinolones, e.g., Ciprofloxacin, Tetracyclines, Zinc Salts
Decreases therapeutic effect of the following drugs:
Bisphosphonates e.g., Alendronate, Quinolones, e.g.,
Ciprofloxacin, Tetracyclines (anti-infective activity)
Administration: Best absorbed on an empty stomach but
may be taken after food to reduce GI adverse effects.
Dilute with water liquid preparations containing iron
salts, and if possible swallow through a drinking straw to
prevent teeth discoloration.
Pregnancy Category: C
ATC Code: Not available
Rx FERROUS SALT + FOLIC ACID
Oral: 60 mg elemental iron + 400 micrograms folic acid per
tablet / capsule / film-coated tablet
A two-component, nutritional supplement of iron and folic
acid given during pregnancy.
Indications: Prevention of iron and folic acid deficiencies,
especially in pregnancy; nutritional supplement during
pregnancy.
NOTE: Low doses of folic acid in combination preparations
are inadequate for the treatment of megaloblastic
anemia, overdose, and therapy with deferoxamine.
Contraindications: Hemolytic anemia; hemochromatosis;
hemosiderosis; repeated blood transfusions of
parenteral iron therapy; pernicious anemia
Dose:
Prevention of iron and folate deficiencies in pregnancy, by
mouth, ADULT, elemental iron, 100 mg + folic acid, 350–
400 micrograms daily throughout pregnancy.
Severe anemia, by mouth, ADULT, elemental iron, 120 mg
+ folic acid 400 micrograms daily for 3 months; CHILD
2–12 years, elemental iron 60 mg + folic acid, 400
micrograms daily for 3 months; CHILD <2 years,
elemental iron, 25 mg + folic acid 100–400 micrograms
daily for 3 months.
Dose Adjustment:
Renal Impairment:
Give iron supplementation when the patient is anemic, and
iron saturation is <20%.
Precautions:
WARNING: Iron salts can exacerbate GI bleeding; thus,
it should be used with caution in patients with GI
disorders.
Transfusion-dependent anemia;
Peptic ulcer, regional enteritis, ulcerative colitis, intestinal
strictures, diverticula;
Pernicious anemia;
Elderly and children;
Pregnancy (avoid use in the first trimester; administer only
in women with low-normal hemoglobin).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-83-320.jpg)
![A
ALIMENTARY TRACT AND METABOLISM
40
Adverse Drug Reactions:
Common: Abdominal pain, black discoloration of feces,
constipation, diarrhea, nausea, vomiting
Less Common: Black discoloration of teeth
Rare: Anaphylaxis, bronchospasm, fever, GI erosion and
perforation, hemosiderosis, irritability, rash, sleep
disturbance
Drug Interactions:
Monitor closely with:
Decreases bioavailability of Methyldopa (interferes with
blood pressure control)
Avoid concomitant use with:
Decreases absorption of Iron:
Antacids, e.g., Aluminum or Magnesium Hydroxide
(separate administration times as long as possible),
Calcium, Doxycycline, Food, e.g., eggs, milk,
Tetracyclines e.g., Doxycyline, Zinc Salts
Decreases absorption of the following drugs:
Bisphosphonates e.g., Alendronate, Doxycycline,
Levothyroxine [administer at least 2 hours apart],
Quinolones, e.g., Ciprofloxacin, Levofloxacin,
Tetracyclines, Zinc Salts
Decreases serum concentration of Folic Acid:
Folic Acid Antagonists, e.g., Methotrexate,
Pyrimethamine, Triamterene, Sulfonamides,
Trimethoprim
Decreases therapeutic effect of the following drugs:
Bisphosphonates e.g., Alendronate, Quinolones, e.g.,
Ciprofloxacin, Levofloxacin, Tetracyclines e.g.,
Doxycycline (anti-infective activity)
Administration: To be taken on an empty stomach, at least
1 hour before or 2 hours after meals.
Avoid taking antacids or antibiotics within 2 hours before
or after administration.
Pregnancy Category: A
ATC Code: Not available
OTC MICRONUTRIENT POWDER
Oral: per 1-gram sachet contains:
Vitamin A 400 micrograms RE
Vitamin C 30 mg
Vitamin D 5 micrograms
Vitamin E 5 mg a-TE
Vitamin B1 0.5 mg
Vitamin B2 0.5 mg
Vitamin B6 0.5 mg
Vitamin B12 0.9 micrograms
Folic acid 150 micrograms
Niacin 6 mg
Iron 10 mg
Zinc 4.1 mg
Copper 0.56 mg
Iodine 90 micrograms
Selenium 17 micrograms
Single-dose packets vitamins and minerals, in powder form,
which can be sprinkled onto any ready-to-eat semisolid
food.
Indications: Prevent vitamin and mineral deficiencies;
improve iron status and reduce anemia among infants
and children 6-23 months of age.
Contraindications: Children with specific conditions, such as
HIV infection or TB (effects and safety of the intervention
have not been evaluated).
Dose:
Prevention of vitamin and mineral deficiencies, improving
iron status, and reducing anemia, by mouth, CHILD and
INFANT 6-23 months, 1 sachet daily, add a mixture of
micronutrients in powder form to any semisolid food.
Precautions:
Programs involving the use of multiple micronutrient
powders for fortification at home of foods should be
preceded by an evaluation of the nutritional status
among children <5 years of age, and existing measures
to control anemia and vitamin A deficiency (e.g.,
hookworm control programs, provision of supplements,
and use of other products for home fortification of foods
and fortified complementary foods), to ensure that daily
micronutrient needs are met and not exceeded.
Adverse Drug Reactions:
Common: Diarrhea
Less Common to Rare: Darkening of the stools, staining of
child’s teeth
Drug Interactions: No information found.
Administration: At minimum, for a period of 2 months,
followed by a period of 3–4 months off supplementation
(so that use of the micronutrient powders is started every
6 months.
Pregnancy Category: Not available
ATC Code: Not available](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-84-320.jpg)



![B
BLOOD AND BLOOD FORMING ORGANS
44
diarrhea, flatulence, gastrointestinal bleeding, nausea,
taste disturbance, vomiting, hematuria, anemia,
retroperitoneal hematoma, unrecognized bleeding sites
(e.g., colon cancer), hepatitis (including cholestatic
hepatitis), osteoporosis (potential association with long-
term use), paralysis, paresthesia, weakness, respiratory
tract bleeding, tracheobronchial calcification,
anaphylactic reaction, hypersensitivity / allergic
reactions, skin necrosis, gangrene, “purple toe”
syndrome.
Drug Interactions:
Monitor closely with:
Decreases absorption of Warfarin:
Bile Acid Sequestrants, Lixisenatide
Enhances anticoagulant effect of Warfarin:
Paracetamol, Agents with Antiplatelet Properties, e.g.,
P2Y12 Inhibitors, Amikacin, Amoxicillin, Bupropion.
Cephalosporins e.g., Cefuroxime, Chloramphenicol,
Chondroitin Sulfate, Cloxacillin, Systemic
Corticosteroids, COX-2 Inhibitors e.g., Celecoxib,
Cyclophosphamide, Etoposide, Exenatide, Fibrates e.g.,
Fenofibrate, Gefitinib, Gemcitabine, Glucagon,
Glucosamine, HMG-CoA Reductase Inhibitors [except
Atorvastatin], Ifosfamide, systemic Ivermectin,
Leflunomide, Levocarnitine, Mirtazapine, Multivitamins
with Fluoride with ADE
Enhances anticoagulant effect of Warfarin:
Multivitamins and Minerals with AE, no Iron, Neomycin,
Nonsteroidal Anti-Inflammatory Agents, Omega-3 Fatty
Acids, Orlistat, Other Anticoagulants, Penicillins [except
Dicloxacillin, Nafcillin, Pentoxifylline, Proguanil,
Propacetamol, Quinidine, Quinine, Quinolone Antibiotics
e.g. Levofloxacin, Salicylates, Selective Serotonin
Reuptake Inhibitors e.g. Sertraline, Sugammadex,
Sulfonylureas e.g., Gliclazide, Tetracycline Derivatives
e.g. Clarithromycin, Thrombolytic Agents e.g. Alteplase,
Thyroid Products, Tibolone, Tramadol, Tricyclic
Antidepressants e.g., Amitriptyline, Vitamin E
Enhances therapeutic effect of Sulfonylureas e.g., Gliclazide
(hypoglycemic effect)
Increases metabolism of Warfarin:
Anticholinergic/Sedative combination, Bosentan,
Rifamycin Derivatives
Increases risk of adverse or toxic effects of Warfarin (may
increase INR/ risk of bleeding):
Ampicillin, Clindamycin, Desvenlafaxine, Prostacyclin
Analogues e.g., Quinidine, Venlafaxine, Vitamin E
Increases risk of adverse or toxic effects (bleeding effect) of
the following drugs:
Deferasirox, Deoxycholic Acid, Nintedanib,
Obinutuzumab, Regorafenib, Iodine I131
Reduces anticoagulant effect of Warfarin:
Azathioprine, Cloxacillin, Coenzyme Q-10, Dicloxacillin,
Flucloxacillin, Floxacillin, Mercaptopurine, Multivitamins
and Minerals with ADEK, Folate, Iron
Avoid concomitant use with:
Counteracts anticoagulant effect of Warfarin:
Estrogen Derivatives or Progestins (potential
prothrombotic effects)
Decreases absorption of Warfarin:
Sucralfate [administer Warfarin at least 2 hours before
or 6 hours after Sucralfate]
Decreases metabolism of Warfarin and increases PT/ INR:
Acute alcoholism, strong CYP2C9 Inhibitors, Imatinib,
Sulfinpyrazone
Decreases protein binding of Warfarin:
Sulfinpyrazone
Decreases serum concentration of Warfarin:
Carbamazepine, Dabrafenib, Enzalutamide, Sucralfate
Enhances anticoagulant effect of Warfarin:
Allopurinol, Amiodarone, Androgens, Apixaban,
Cimetidine, Clopidogrel, Dabigatran Etexilate, Fibric Acid
Derivatives, Fosphenytoin, Imatinib, NSAID, Phenytoin,
Salicylates [except Salsalate], Sorafenib, Streptokinase,
Sulfonamide Derivatives
Enhances therapeutic effect of Rivaroxaban (anticoagulant
effect)
Increases metabolism of Warfarin and decreases PT / INR:
Chronic alcoholism, Barbiturates e.g., Phenobarbital,
strong CYP2C9 Inducers
Increases serum concentration of Warfarin:
Amiodarone [reduce Warfarin dose by 30 to 50%],
Capecitabine, Ceritinib, Fluconazole, systemic and
topical Fluorouracil, Fosphenytoin, systemic Fusidic Acid,
systemic Metronidazole, topical Miconazole, Phenytoin,
Sorafenib, Tamoxifen
Reduces anticoagulant effect of Warfarin:
Antithyroid Agents e.g., PTU, Contraceptives, e.g.,
Estrogens, Progestins, Phytonadione, Sucralfate
FOOD/SUPPLEMENT INTERACTIONS.
Cranberry juice, Ginkgo biloba, herbs with anticoagulant or
antiplatelet properties, e.g., alfalfa, anise, bilberry
(bleeding) may increase warfarin effect.
Vitamin K-rich foods, including green tea (Camellia
sinensis), chewing tobacco, a variety of oils (canola, corn,
olive, peanut, safflower, sesame seed, soybean, or
sunflower, may decrease anticoagulant effects of
Warfarin.
Administration: May be taken with or without food. Take at
the same time each day. Maintain a consistent diet.
Avoid drastic changes in diet which decrease efficacy of
warfarin. Consult prescriber before making changes in
diet.
NOTE: Instruct patients to report bleeding, accidents, or falls
as well as any new or discontinued medications, herbal
or alternative products used, or significant changes in
smoking or dietary habits. Unrecognized bleeding sites](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-88-320.jpg)
![B
BLOOD AND BLOOD FORMING ORGANS
46
peripheral artery occlusive disease and thrombosis /
thromboembolism (e.g., deep vein thrombosis (DVT)).
Contraindications: Thrombocytopenia associated with a
positive in vitro test for antiplatelet antibodies in the
presence of enoxaparin; active major bleeding; In
neonates, infants, and pregnant or nursing mothers.
Dose:
NOTE: 1 mg enoxaparin = 100 units anti-Xa activity
Weight-based doses (e.g., 1 mg/kg) are commonly
rounded to the nearest 10 mg.
Deep Vein Thrombosis (DVT) prophylaxis in abdominal
surgery, by SC injection, ADULT, 40 mg once daily, with
initial dose given 2 hours prior to surgery; continue until
risk of DVT has diminished, usually 7–10 days.
DVT prophylaxis in hip replacement surgery, by SC injection,
ADULT, 30 mg twice daily (every 12 hours), with initial
dose within 12–24 hours after surgery, and every 12
hours for at least 10 days or until risk of DVT has
diminished or the patient is adequately anticoagulated
on warfarin; or
40 mg once daily, with initial dose within 9–15 hours
before surgery, and daily for at least 10 days (or up to 35
days postoperatively) or until risk of DVT has diminished
or the patient is adequately anticoagulated on warfarin.
DVT prophylaxis in knee replacement surgery, by SC
injection, ADULT, 30 mg every 12 hours, with initial dose
within 12–24 hours after surgery, and every 12 hours for
at least 10 days or until risk of DVT has diminished or the
patient is adequately anticoagulated on warfarin.
DVT prophylaxis in medical patients with severely restricted
mobility during acute illness, by SC injection, ADULT, 40
mg once daily; continue until risk of DVT has diminished,
usually 6–11 days [NOTE: Start warfarin on the first or
second treatment day and continue enoxaparin until INR
is ≥2 for at least 24 hours (usually 5–7 days)].
DVT, acute treatment in inpatients with or without
pulmonary embolism, by SC injection, ADULT, 1 mg/kg
per dose every 12 hours or 1.5 mg/kg every 24 hours.
DVT, acute treatment in outpatients without pulmonary
embolism, by SC injection, ADULT, 1 mg/kg per dose
every 12 hours.
STEMI, by SC injection, ADULT ≥75 years, initially 0.75
mg/kg every 12 hours, do NOT administer by IV bolus
(maximum dose, 75 mg for first 2 doses), for
maintenance, after the first 2 doses, 0.75 mg/kg every
12 hours;
by IV bolus, ADULT <75 years, initially 30 mg once by IV
bolus plus 1 mg/kg once by SC injection, followed by 1
mg/kg by SC injection, every 12 hours (maximum, 100
mg for the first 2 doses).
STEMI, maintenance, by SC injection,
1 mg/kg every 12 hours (administer the first
maintenance dose 12 hours after the second SC dose)
[NOTE: Therapy may be continued for up to 8 days or until
revascularization. Unless contraindicated, all patients
should receive aspirin (indefinitely) and clopidogrel. In
patients with STEMI receiving thrombolytics, initiate
enoxaparin dosing between 15 minutes before and 30
minutes after fibrinolytic therapy.].
Unstable angina or NSTEMI, by SC injection, ADULT, 1
mg/kg every 12 hours in conjunction with oral aspirin
therapy; continue for the duration of hospitalization, at
least 2 days for up to 8 days.
Dose Adjustment:
Geriatric:
Dose adjustment may be required if renal impairment is
present.
In patients ≥75 years being treated for STEMI, administer a
lower dose of 0.75 mg/kg every 12 hours and omit IV
bolus dose.
Renal Impairment:
Primarily eliminated via the renal route. Reduce doses and
frequently monitor anti-Xa levels as accumulation may
occur with repeated doses.
For patients with CrCl <30 mL/minute, if used for DVT
prophylaxis in abdominal surgery, hip replacement, knee
replacement, or in medical patients during acute illness,
by SC injection, 30 mg once daily.
For patients with CrCl <30 mL/minute, if used for DVT
treatment, for both inpatient or outpatient treatment in
conjunction with warfarin, by SC injection, 1 mg/kg once
daily.
For patients with CrCl <30 mL/minute, if used for STEMI, by
SC injection, ADULT ≥75 years, maintenance, 1 mg/kg
once daily;
by IV bolus, ADULT <75 years, initially 30 mg with the first
dose of the SC maintenance regimen (maintenance, by
SC injection, 1 mg/kg once daily.
For patients with CrCl <30 mL/minute, if used for unstable
angina or NSTEMI, by SC injection, ADULT 1 mg/kg once
daily.
Obesity:
Use actual body weight to calculate dose. Dose capping is
not recommended. Twice daily dosing preferred.
CONVERSION:
Conversion from IV unfractionated heparin (UFH)
infusion to SC enoxaparin: Calculate specific dose for
enoxaparin based on indication. Discontinue UFH and
begin enoxaparin within 1 hour.
Conversion from SC enoxaparin to IV UFH infusion:
Discontinue enoxaparin, calculate specific dose for IV
UFH infusion based on indication. Omit heparin bolus or
loading dose.
Converting from SC enoxaparin dosed every 12 hours:
Start IV UFH infusion 10–11 hours after last enoxaparin
dose.
Converting from SC enoxaparin dosed every 24 hours:
Start IV UFH infusion 22–23 hours after last enoxaparin
dose.
Precautions:
WARNING: NOT to be used interchangeably (unit for
unit) with heparin or any other LMWH.
NOT recommended for use in patients with current
heparin-induced thrombocytopenia (HIT) or HIT with
thrombosis due to high cross-reactivity to heparin-
platelet factor-4 antibody.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-90-320.jpg)
![B
BLOOD AND BLOOD FORMING ORGANS
47
Epidural or spinal hematomas may occur in patients
who are anticoagulated with LMWHs or heparinoids
and are receiving neuraxial anesthesia or
undergoing spinal puncture. May result in long-term
or permanent paralysis.
Renal impairment; Hepatic impairment; Elderly (increased
injection-associated bleeding and serious adverse
reactions; increased incidence of bleeding with doses of
1.5 mg/kg daily or 1 mg/kg every 12 hours).
Adverse Drug Reactions:
Common: Confusion, pain, nausea, diarrhea, major
hemorrhage (intracranial, retroperitoneal, or
intraocular), moderate thrombocytopenia, anemia,
bruise, hematuria, fever, and hematoma, irritation,
bruising, erythema, or pain at injection site,
Less Common: Alopecia, anaphylaxis, anaphylactoid
reaction, eczematous rash (plaques), eosinophilia,
epidural hematoma after spinal puncture, headache,
hepatic injury (hepatocellular and cholestatic),
hyperkalemia, hypersensitivity angiitis, hypersensitivity
reaction, osteoporosis (long-term use), pruritic
erythematous rash (patches), pruritus, purpura,
retroperitoneal hemorrhage, severe anemia
(hemorrhagic), skin necrosis, thrombocythemia,
thrombocytopenia, thrombosis (prosthetic valve;
enoxaparin-induced thrombocytopenia), shock, urticaria,
vesiculobullous rash
Rare: Intracranial hemorrhage
Administration: Administer by deep SC injection alternating
between the left or right anterolateral and left or right
posterolateral abdominal wall.
Do NOT administer intramuscularly.
Do NOT rub injection site to minimize bruising.
Do NOT expel the air bubble from the syringe prior to
injection to avoid loss of drug from the 30 mg and 40 mg
prefilled syringes.
Do NOT mix with other infusions or injections.
See General Information on Heparin Group under
Antithrombotic Agents for further information.
Pregnancy Category: B
ATC Code: B01AB05
Rx
HEPARIN SODIUM
(UNFRACTIONATED,
BOVINE ORIGIN)
Inj.: 1,000 IU/mL and 5,000 IU/mL, 5 mL and 30 mL vial
(IV infusion, SC)
It is a sulfated mucopolysaccharide prepared from the lungs
of oxen or the intestinal mucosa of oxen, pigs, or sheep.
Heparin inhibits clotting of blood by enhancing the action
of antithrombin III, which inhibits the activity of activated
clotting factors including thrombin (factor IIa) and
activated factor X (factor Xa).
Indications: Prophylaxis and treatment of thromboembolic
disorders (e.g, venous thromboembolism, acute arterial
thrombosis); acute coronary syndrome (e.g., unstable
angina, non-ST-elevation myocardial infarction (NSTEMI),
ST-elevation myocardial infarction (STEMI));
anticoagulant for extracorporeal and dialysis
procedures.
Contraindications: Severe thrombocytopenia; uncontrolled
active bleeding except when due to disseminated
intravascular coagulation (DIC); not for use when
appropriate blood coagulation tests cannot be obtained
at appropriate intervals; neonates; infants; pregnant or
nursing mothers
Dose:
STEMI, as adjunct to fibrinolysis with full-dose alteplase,
reteplase, or tenecteplase, by IV infusion, ADULT, initially
60 units/kg (maximum, 4000 units), then 12 units/kg
every hour (maximum, 1000 units/hour) as continuous
IV infusion, check aPTT every 4–6 hours; adjust to target
of 1.5–2 times the upper limit of control (50–70
seconds); continue for a minimum of 48 hours,
preferably for the duration of hospitalization (up to 8
days) or until revascularization.
Unstable angina or NSTEMI, by IV bolus, ADULT, initially 60
units/kg (maximum, 4000 units) followed by an initial IV
infusion of 12 units/kg every hour (maximum, 1000
units/hour); check aPTT every 4–6 hours; adjust to target
of 1.5–2 times the upper limit of control (50–70
seconds); recommended duration is 48 hours or until
percutaneous coronary intervention is performed
Anticoagulation, intermittent administration, by IV infusion,
ADULT, initially 10,000 units, then 50 to 70 units/kg
(5,000–10,000 units) every 4–6 hours.
Maintenance of line patency or line flushing, by IV infusion,
ADULT and CHILD, 100 units/mL; INFANT, 10 units/mL
[NOTE: Capped PVC catheters and peripheral heparin
locks require flushing more frequently (e.g., every 6–8
hours). The volume of heparin flush is similar or slightly
greater than the volume of catheter. Additional flushes
should be given when stagnant blood is observed in
catheter, after catheter is used for drug or blood
administration, and after blood withdrawal from
catheter.].
Thromboprophylaxis for venous thromboembolism
prevention, by SC injection, ADULT, 5,000 units every 8–
12 hours; in acutely ill hospitalized medical patients at
increased risk of thrombosis and selected surgical
patients; and for a minimum of 10–14 days is
recommended for patients undergoing total hip
arthroplasty, total knee arthroplasty, or hip fracture
surgery.
Treatment in venous thromboembolism (VTE), by IV or SC
injection, ADULT, For patients starting intravenous
unfractionated heparin (UFH), the initial bolus and initial
rate of the continuous infusion should be weight-
adjusted (bolus 80 units/kg, immediately followed by 18
units/kg/hour for venous thromboembolism (VTE); bolus
70 units/kg immediately followed by 15 units/kg/hour
for cardiac or stroke patients). Subsequent dose
adjustment should be guided by monitoring with
activated partial thromboplastin time (aPTT) testing 6
hours after UFH bolus/infusion is started with
therapeutic aPTT range of 1.5 – 2.5 times control. For
outpatients with VTE treated with subcutaneous UFH,](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-91-320.jpg)

![B
BLOOD AND BLOOD FORMING ORGANS
49
venous thromboembolism and to prevent clotting during
extracorporeal circulation.
Indications: Treatment of deep vein thrombosis (DVT)
and/or pulmonary embolism (PE) (except in patients with
severe hemodynamic instability) ; prevention of venous
thromboembolism (VTE) following orthopedic surgery or
following general surgery in patients at high risk of VTE;
prevention of clotting in indwelling intravenous lines and
extracorporeal circuit during hemodialysis (in patients
without high bleeding risk).
Contraindications: Active bleeding; history of confirmed or
suspected immunologically mediated heparin-induced
thrombocytopenia (HIT) or positive in vitro platelet
aggregation test in the presence of tinzaparin; acute or
subacute endocarditis; generalized hemorrhage
tendency and other conditions involving increased risks
of hemorrhage (e.g., severe hepatic insufficiency,
imminent abortion); hemophilia or major blood clotting
disorders; acute cerebral insult or hemorrhagic
cerebrovascular accidents without systemic emboli;
uncontrolled severe hypertension; diabetic or
hemorrhagic retinopathy; injury or surgery involving the
brain, spinal cord, eyes or ears; spinal / epidural
anesthesia in patients requiring treatment dosages of
tinzaparin; use of multi-dose vials containing benzyl
alcohol in children <2 years of age, premature infants,
and neonates; pregnant or nursing mothers
Dose:
NOTE: 1 mg of tinzaparin equals 70120 units of anti-Xa
activity.
DVT and/or PE, treatment, by SC injection, ADULT, 175 anti-
Xa units/kg once daily (maximum, 18,000 anti-Xa
units/day), start warfarin on the first or second treatment
day and continue tinzaparin until INR is ≥2 for at least 24
hours, usually 5–7 days [NOTE: May use body weight dosing
using prefilled syringes].
DVT, prophylaxis in hip replacement surgery, by SC injection,
ADULT, preoperative regimen, 50 anti-Xa units/kg given
2 hours preoperatively followed by 50 anti-Xa units/kg
once daily for 7–10 days;
postoperative regimen, 75 anti-Xa units/kg once daily,
with initial dose given postoperatively and continued for
7–10 days [NOTE: Initiate of LMWH ≥12 hours preoperatively or
≥12 hours postoperatively, may extend duration up to 35 days].
DVT, prophylaxis in knee replacement surgery, by SC
injection, ADULT, 75 anti-Xa units/kg once daily, with
initial dose given postoperatively and continued for 7–10
days [NOTE: Initiate of LMWH ≥12 hours preoperatively or ≥12
hours postoperatively, may extend duration up to 35 days; may
use body weight dosing using prefilled syringes].
DVT, prophylaxis in general surgery, by SC injection, ADULT,
3,500 anti-Xa units once daily, with initial dose given 2
hours prior to surgery and then continued
postoperatively for 7–10 days.
Anticoagulant in extracorporeal circuit during hemodialysis,
for stable patients with chronic renal failure, by IV bolus,
ADULT, for dialysis session ≤4 hours and no hemorrhage
risk, initially 4,500 anti-Xa units at beginning of dialysis,
typically achieves plasma concentrations of 0.5–1 anti-
Xa units/mL, may give larger bolus for dialysis sessions
>4 hours; [NOTE: For subsequent dialysis sessions, may adjust
dose as necessary in increments of 500 anti-Xa units based on
previous outcome];
For dialysis sessions ≤4 hours with hemorrhage risk,
initially 2,250 anti-Xa units at beginning of dialysis [NOTE:
Do NOT add to dialysis circuit. For subsequent dialysis sessions,
adjust dose as necessary to achieve plasma concentrations of
0.20.4 anti-Xa units/mL].
Dose Adjustment:
Geriatric:
Use is not recommended in patients >70 years of age with
renal impairment.
Renal Impairment:
For patients with CrCl ≥30 mL/minute, no dose adjustment
needed provided it primarily undergoes renal
elimination.
For patients with CrCl <30 mL/minute, consider dose
reduction.
Hepatic Impairment:
No dosage adjustment needed provided it does not undergo
hepatic metabolism.
Precautions:
WARNING: Contraindicated in patients with HIT or HIT with
thrombosis due to high cross-reactivity to heparin-platelet
factor4 antibody.
Hepatic impairment (use with caution); Renal impairment
(use with caution); Elderly (increased sensitivity may be
possible due to a decline in renal function).
Adverse Drug Reactions:
Common: chest pain, angina pectoris, arrhythmia, coronary
thrombosis or MI, dependent edema, thromboembolism,
fever, headache, pain, bullous eruption, erythematous
rash, maculopapular rash, skin necrosis, nausea,
abdominal pain, constipation, diarrhea, vomiting, urinary
tract infection, bleeding events, granulocytopenia,
thrombocytopenia, injection site hematoma or cellulitis,
back pain, epistaxis, dyspnea, allergic reaction,
neoplasm.
Less Common: Agranulocytosis, angioedema,
anaphylactoid reaction, hemoptysis, hypoaldosteronism,
hyperkalemia, metabolic acidosis, ocular hemorrhage,
osteopenia, osteoporosis, priapism, pruritus, rash, spinal
epidural hematoma, Stevens-Johnson syndrome,
thrombocytosis, toxic epidermal necrolysis, urticaria.
Administration: For SC use only.
Administer by deep SC injection into the lower abdomen,
outer thigh, lower back, or upper arm. Patient should be
lying down or sitting. Vary injection site daily.
Do NOT rub the injection site to minimize bruising.
May be administered by IV injection in hemodialysis
patients.
Do NOT administer by IM route and avoid IM
administration of other medications due to the risk of
hematoma formation.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-93-320.jpg)

![B
BLOOD AND BLOOD FORMING ORGANS
52
Increases risk of adverse or toxic effects of Apixaban
(bleeding)
Increases serum concentration of Cilostazol:
Fusidic Acid (systemic), Grapefruit Juice
Increases serum concentration of Dabigatran Etexilate
FOOD INTERACTION. A high-fat meal may increase peak concentration
by 90% and increase AUC by 25%
Administration: Administer 30 minutes before or 2 hours
after meals (breakfast and dinner).
Pregnancy Category: C
ATC Code: B01AC23
Rx CLOPIDOGREL
Oral: 75 mg tablet
A thienopyridine-derived, platelet aggregation inhibitor that
has no effect on prostaglandin metabolism unlike
aspirin. It is used as an alternative for patients who are
unable to take aspirin in the treatment of thrombosis.
Indications: Prevention of atherothrombotic events in:
peripheral arterial disease, or within 35 days of MI, or
within 6 months of ischemic stroke; in acute coronary
syndrome without ST-segment elevation (unstable
angina or non-Q wave MI), including patients undergoing
stent placement following percutaneous coronary
intervention (in combination with aspirin); in acute MI
with ST-segment elevation, and in combination with ASA
in medically-treated patients eligible for thrombolytic
therapy; in patients with atrial fibrillation where oral
anticoagulation is unsuitable; neurologic indications;
transient ischemic attack and acute ischemic cerebral
infarction (for early specific treatment or secondary
prevention of ischemic stroke).
Contraindications: Severe liver impairment; intracranial
hemorrhage, peptic ulcer or other pathological bleeding;
breastfeeding.
Dose:
Acute coronary syndrome, unstable angina or NSTEMI, by
mouth, ADULT, 300 mg loading dose, then 75 mg daily
in combination with aspirin 75–100 mg daily.
Acute coronary syndrome, STEMI, by mouth, ADULT, 75 mg
daily (in combination with aspirin 162–325 mg daily,
then 81–162 mg daily).
Acute ischemic infarction and secondary prevention of
acute ischemic stroke, by mouth, ADULT, 75 mg once
daily.
Coronary artery disease, by mouth, ADULT, 75 mg once
daily.
Recent MI, stroke, or established peripheral arterial
disease, by mouth, ADULT, 75 mg daily [NOTE:
Recommended as alternative to aspirin, or
concomitantly with aspirin if patient is not at increased
risk for bleeding but at high risk for cardiovascular
disease].
Transient ischemic attack, early specific treatment), by
mouth, ADULT, 75 mg once daily.
Dose Adjustment:
Renal Impairment:
For mild-to-moderate impairment, dose adjustment is not
required.
For severe impairment, refer patient to a specialist.
Precautions:
WARNING: CYP2C19 Inhibition and Poor Metabolizers:
Effectiveness depends on activation to active
metabolite by cytochrome P450 system, principally
CYP2C19. May be less effective in poor metabolizers
lacking CYP2C19. Poor metabolizers exhibit higher
cardiovascular event rates after acute coronary
syndrome or percutaneous coronary intervention at
recommended doses. >50% of Asians have CYP2C19
genetic variants that inhibit Clopidogrel metabolism.
Use of CYP2C19 inhibitors (Proton Pump Inhibitors)
or use in poor metabolizers may decrease
antiplatelet effect.
Patients at risk of increased bleeding from trauma,
surgery, or other pathological conditions;
patients taking medications that increase
risk of bleeding; patients allergic to aspirin
who are undergoing PCI; History of bleeding or
hemostatic disorders; bleeding diathesis; ulcers; renal
impairment; hepatic impairment; Surgery (may need to
discontinue 5-10 days before surgical procedure);
Pregnancy (avoid use if possible).
Adverse Drug Reactions:
Common: Abdominal pain, bleeding, chest pain,
depression, diarrhea, dyspepsia, flu-like syndrome,
hemorrhage, rhinitis, upper respiratory tract infection,
urinary tract infection, urticaria.
Less Common: Constipation, dizziness, flatulence, gastritis,
GI ulcer, headache, leukopenia, nausea, paresthesia,
pruritus, rash, vomiting
Rare: Acute liver failure, agranulocytosis, angioedema,
aplastic anemia, bronchospasm, colitis, confusion,
exfoliative dermatitis, hallucinations, hepatitis,
hypersensitivity-like reactions, hypotension, interstitial
pneumonitis, lichen, myalgia, neutropenia, pancreatitis,
Stevens-Johnson syndrome (SJS), stomatitis,
thrombocytopenia, thrombotic thrombocytopenic
purpura, vasculitis
Drug Interactions:
NOTE: CYP2C19 enzyme metabolizes Clopidogrel to its
active metabolite. Combining Clopidogrel with CYP2C19
Inhibitors (e.g. Omeprazole) of may decrease its efficacy.
Monitor closely with:
Enhances therapeutic effect of Clopidogrel:
Carbamazepine. Rifampin
Increases risk of adverse or toxic effects when used in
combination with the following drugs:
Anticoagulants, e.g., Warfarin (bleeding); Aspirin
(unusual bleeding, severe abdominal pain, weakness,
black stools); drugs which can affect the clotting process,
e.g. NSAIDs, other Antiplatelets (bleeding; inhibits
platelet aggregation)](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-96-320.jpg)
![B
BLOOD AND BLOOD FORMING ORGANS
53
Reduces therapeutic effect of Clopidogrel:
Atorvastatin (blood clotting), Clarithromycin,
Erythromycin, Isoniazid
Avoid concomitant use with:
Reduces antiplatelet effect of Clopidogrel by reducing
formation of its active metabolite:
Proton Pump Inhibitors, e.g., Omeprazole, Esomeprazole
Administration: May be taken with or without food.
Pregnancy Category: B
ATC Code: B01AC04
Rx DIPYRIDAMOLE
Oral: 25 mg tablet
A non-nitrate coronary vasodilator that inhibits platelet
aggregation. It inhibits phosphodiesterase and
adenosine reuptake.
Indications: Secondary prevention of stroke in patients with
a history of non-cardioembolic ischemic stroke or TIA
(preferably with aspirin); to decrease thrombosis after
artificial heart valve replacement (with warfarin).
Dose:
Adjunctive therapy for prophylaxis of thromboembolism with
cardiac valve replacement, by mouth, ADULT, 75–200
mg 4 times daily.
Dose Adjustment:
Geriatric:
Avoid use due to risk of orthostatic hypotension.
Precautions:
Cardiovascular disease (use with caution in patients with
hypotension, unstable angina, and/or recent MI); hepatic
impairment; Elderly (use with caution); Lactation (use
with caution).
Adverse Drug Reactions:
Common: Dizziness, headache, skin rash, pruritus,
abdominal distress, diarrhea, vomiting, hepatic
insufficiency.
Less Common: Alopecia, arthritis, cholelithiasis, dyspepsia,
fatigue, hepatitis, hypersensitivity reaction, hypotension,
laryngeal edema, malaise, myalgia, nausea, palpitations,
paresthesia, tachycardia, thrombocytopenia.
Drug Interactions:
Monitor closely with:
Enhances anticoagulant effect of Dipyridamole:
Other Anticoagulants e.g., Warfarin, Heparin;
Thrombolytic Agents e.g., Streptokinase
Enhances antiplatelet effect of Dipyridamole:
Agents with Antiplatelet Properties, e.g., P2Y12
Inhibitors, NSAIDs, SSRIs; Glucosamine; Multivitamins/
Fluoride with Vitamins ADE; Multivitamins/ Minerals with
Vitamins ADEK, Folate, Iron; Multivitamins/ Minerals
with Vitamins AE, no Iron; Omega3 Fatty Acids;
Pentoxifylline; Prostacyclin Analogues; Vitamin E
Enhances therapeutic effect of Dipyridamole:
Hypotensive effect: Barbiturates e.g., Phenobarbital;
Nicorandil; Risperidone
Enhances therapeutic effect of Beta Blockers (bradycardic
effect) [except Levobunolol, Metipranolol]
Increases risk of adverse or toxic effects of Dipyridamole:
Ibrutinib; Other Hypotensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Bleeding: Deoxycholic Acid; Obinutuzumab; Salicylates
e.g. Aspirin; Iodine 131; Ibritumab
Orthostatic hypotensive effect: Duloxetine
Levodopa
Reduces therapeutic effect of Acetylcholinesterase
Inhibitors e.g. Physiostigmine
Avoid concomitant use with:
Enhances therapeutic effect of Rivaroxaban (anticoagulant
effect)
Increases risk of adverse or toxic effects of Adenosine
(cardiovascular effects; Apixaban (bleeding)
Increases risk of adverse or toxic effects of Dipyridamole:
Herbs with anticoagulant or antiplatelet properties, e.g.,
Alfalfa, Anise, Bilberry (bleeding)
Increases serum concentration of the following drugs:
Afatinib (reduce Afatinib by 10mg if not tolerated);
Colchicine (increase distribution into certain tissues,
e.g., brain); Dabigatran Etexilate [active metabolites];
Doxorubicin (conventional); Everolimus [reduce doses if
used for subependymal giant cell astrocytoma or renal
cell carcinoma]; Pazopanib; Silodosin; Topotecan;
Vincristine (liposomal)
Administration: Administer with water 1 hour before meals.
NOTE: Preferably used in combination with aspirin. When
used concomitantly with aspirin, consider the cautions,
precautions, and contraindications associated with
aspirin.
Pregnancy Category: B
ATC Code: B01AC07](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-97-320.jpg)

![B
BLOOD AND BLOOD FORMING ORGANS
56
OTHER ANTITHROMBOTIC AGENTS
Rx FONDAPARINUX
Inj.: 2.5 mg/0.5 mL solution (as sodium salt)
A synthetic activated factor X (Xa) inhibitor used as an
anticoagulant. It increases the affinity of antithrombin III
for factor Xa, a key enzyme in the coagulation cascade.
Indications: Management of unstable angina (UA) or non-ST
segment elevation myocardial infarction (NSTEMI);
management of ST segment elevation myocardial
infarction (STEMI).
Contraindications: Severe renal impairment; body weight
<50 kg; active major bleeding; bacterial endocarditis;
Thrombocytopenia associated with a positive in vitro test
for antiplatelet antibodies in the presence of
Fondaparinux.
Dose:
NOTE: PT and aPTT are insensitive measures of
Fondaparinux activity. If unexpected changes in
coagulation parameters or major bleeding occur,
discontinue fondaparinux.
UA or NSTEMI, by SC injection, ADULT, 2.5 mg once daily for
the duration of hospitalization or up to 8 days, initiate as
soon as possible after presentation.
STEMI, by IV injection, ADULT, 2.5 mg once;
for subsequent doses, starting the following day, by SC
injection, 2.5 mg once daily for the duration of the
hospitalization up to 8 days, or until revascularization
[NOTE: Discontinue Fondaparinux 24 hours prior to
CABG surgery and administer UFH instead, as per
institutional practice].
Dose Adjustment:
Renal Impairment:
For CrCl >50 mL/minute, no dose adjustment is necessary,
however, total clearance is reduced ~25%.
For CrCl of 30–50 mL/minute, use with caution. Total
clearance ~40% lower compared to normal renal
function. When used for thromboprophylaxis, reduce
dose 50% or use low-dose heparin.
For CrCl <30 mL/minute, use is contraindicated.
Hepatic Impairment:
For severe impairment, use with caution. Monitor closely for
signs of bleeding.
Precautions:
WARNING: Epidural or spinal hematomas may occur in
patients who are anticoagulated with low molecular
weight heparins, heparinoids, or fondaparinux and
are receiving neuraxial anesthesia or undergoing
spinal puncture. This may result in longterm or
permanent paralysis. Monitor patients frequently for
signs and symptoms of neurologic impairment. If
neurologic compromise is noted, urgent treatment is
necessary.
Hemorrhage may occur at any site. Risk appears
increased by several factors including renal
dysfunction, age (>75 years), and weight (<50 kg).
Bleeding; thrombocytopenia; Hepatic impairment; Renal
impairment; Patients <50 kg (use with caution; dose
reduction recommended); Elderly (use with caution ;
increased risk of bleeding in patients >75 years of age);
Lactation (use with caution).
Adverse Drug Reactions:
Common: Anemia, hypotension, insomnia, dizziness,
confusion, increased wound secretion, skin blister,
hypokalemia, thrombocytopenia, purpura, hematoma,
minor or major hemorrhage, postoperative hemorrhage,
postoperative wound infection, epistaxis.
Less Common: Anaphylactoid reaction, anaphylaxis,
angioedema, catheter site thrombosis, elevated aPTT
associated with bleeding, epidural hematoma,
hemorrhagic death, injection site reaction (bleeding, skin
rash, pruritus), intracranial hemorrhage, reoperation due
to bleeding, spinal hematoma, thrombocytopenia,
severe thrombocytopenia (<50,000/mm3).
Drug Interactions:
Monitor closely with:
Enhances anticoagulant effect of Fondaparinux:
Agents with Antiplatelet Properties, e.g., P2Y12
Inhibitors, NSAIDs, SSRIs; Omega-3 Fatty Acids; Other
Anticoagulants; Salicylates e.g. Aspirin; Sugammadex;
Thrombolytic Agents; Tibolone; Vitamin E (increases
overall risk for bleeding)
Increases risk of adverse or toxic effects of Fondaparinux:
Ibrutinib; Prostacyclin Analogues
Increases risk of adverse or toxic effects of the following
drugs:
Deferasirox (GI ulceration or irritation; GI bleeding;);
Deoxycholic Acid (bleeding or bruising in the treatment
area)
Increases risk of adverse or toxic effects of the following
drugs:
Bleeding: Nintedanib; Obinutuzumab; Iodine I131
Avoid concomitant use with:
Enhances anticoagulant effect of the following drugs:
Apixaban; Dabigatran Etexilate; Rivaroxaban
Increases risk of bleeding of Fondaparinux:
Herbs with anticoagulant or antiplatelet properties, e.g.,
Alfalfa, Anise, Bilberry;
Reduces anticoagulant effect of Fondaparinux:
Estrogen Derivatives, Progestins [except Tibolone]
Administration: Initiate therapy 6–8 hours following surgery.
When used for DVT prophylaxis, early initiation (before 6
hours after orthopedic surgery) has been associated with
increased bleeding.
For STEMI, administer via IV route. Administer initial dose
as IV push or mix in NS and infuse over 1–2 minutes.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-100-320.jpg)

![B
BLOOD AND BLOOD FORMING ORGANS
59
Indication Bebulin Profilnine
Dental surgery,
single tooth
Usually 50–75
units/kg as a
single infusion
1 hour prior to
surgery [raise
factor IX level
to 40–60% of
normal on day
of surgery]
Maintenance
dose, 30–50
units/kg every
16–24 hours
for 7–10 days
following
surgery or until
healing has
been achieved
[raise factor IX
level to 50% of
normal
immediately
prior to
procedure;
maintain factor
IX levels at 30
to 50% of
normal]
Dental surgery,
multiple teeth
Replacement
therapy may be
required for up
to 1 week
[raise factor IX
level to 40–
60% of normal
on day of
surgery]
Indication Bebulin Profilnine
Minor
bleeding, e.g.,
early
hemarthrosis,
minor
epistaxis,
gingival
bleeding, mild
hematuria
Initially 25–35
units/kg for 1
day [raise
factor IX level
to 20% of
normal]
[NOTE: A single
dose is usually
sufficient, but
a second dose
may be given
after 24 hours]
Initially 20–30
units/kg every
16–24 hours
for 1–2 days
for minor
hemorrhage or
until
hemorrhage
stops and
healing has
been achieved
[raise factor IX
level to 20–
30% of normal]
Moderate
bleeding, e.g.,
severe joint
bleeding, early
hematoma,
major open
bleeding,
minor trauma,
minor
hemoptysis,
hematemesis,
melena, major
hematuria
Initially 50–65
units/kg for 2
days, or until
adequate
wound healing
[raise factor IX
level to 40% of
normal]
Initially, 20–30
units/kg every
16–24 hours
for 2–7 days
for moderate
hemorrhage,
or until
hemorrhage
stops and
healing has
been achieved
[raise factor IX
level to 20–
30% of normal]
Major
bleeding, e.g.,
severe
hematoma,
major trauma,
severe
hemoptysis,
hematemesis,
melena
Initially 75–90
units/kg for 2–
3 days or until
adequate
wound healing
[raise factor IX
level to ≥60%
of normal]
Initially 30–50
units/kg every
16–24 hours
(maintenance
dose, 20
units/kg) [raise
factor IX level
to 30–50% of
normal]
Following this
treatment
period,
maintain factor
IX levels at
20% of normal
for 3–10 days,
or until healing
has been
achieved
Minor surgical
procedures
Typical dose,
50–75
units/kg [raise
factor IX level
to 40–60% of
normal on day
of surgery]
Then lower
dose to usually
26–65
units/kg for 1–
2 weeks or
until adequate
wound healing
[decrease
factor IX level
to 20 to 40% of
normal during
initial postop
period]
Give preop
dose 1 hour
prior to
surgery,
initially every
12 hours, then
every 24 hours
postop
Initially 30–50
units/kg prior
to surgery
[raise factor IX
level to 30–
50% of normal]
Maintenance
dose, 30–50
units/kg every
16–24 hours
for 7–10 days
following
surgery or until
healing is
achieved
[maintain
factor IX levels
at 30 to 50% of
normal]](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-103-320.jpg)
![B
BLOOD AND BLOOD FORMING ORGANS
60
Formula for units required to raise blood level %:
NOTE: Larger doses may be required, especially if treatment
is delayed.
[Bebulin] factor IX 1 unit/kg will increase the plasma factor
IX level by 0.8%
Number of Factor IX units required =
body weight (kg) x desired factor IX increase (as % of
normal) x 1.2 units/kg
[Profilnine] factor IX 1 unit/kg will increase the plasma
factor IX level by 1%
Number of factor IX units required =
bodyweight (kg) x desired factor IX increase (as % of
normal) x 1 unit/kg
Dose Adjustment:
Hepatic Impairment:
No dose adjustment required. Monitor factor IX levels.
Precautions:
WARNING: Factor IX complex (factors II, IX, X) contains
low or nontherapeutic levels of factor VII component.
Do NOT confuse with prothrombin complex
concentrate (factors II, VII, IX, X, protein C, protein S),
which contains therapeutic levels of factor VII.
Antibody formation; Thrombotic events; Hepatic impairment
(use with caution)
Adverse Drug Reactions:
Common: Flushing, thrombosis, chills, fever, headache,
lethargy, somnolence, rash, urticaria, nausea, vomiting,
disseminated intravascular coagulation, paresthesia,
dyspnea, anaphylactic shock, development of clotting
factor antibodies, heparin-induced thrombocytopenia.
Administration: Administer by IV infusion. Infuse solution at
room temperature at 2 mL/minute for Bebulin or 10
mL/minute for Profilnine.
Prior to reconstitution, bring diluent (SWFI) and Factor IX
Concentrate to room temperature. Do NOT exceed 37°C
[98.6°F]. Gently rotate or agitate to dissolve. Do NOT
shake. Use reconstituted solution within 3 hours. Do NOT
refrigerate. Vials are intended for single use. Discard
unused portion.
Do NOT mix with other drugs or solvents.
Do NOT exceed the recommended infusion rates to
prevent vasomotor reactions due to rapid administration.
Slowing the rate of infusion, changing the lot of
medication, or administering antihistamines may relieve
some adverse reactions.
NOTE: [Bebulin] Reconstituted product should be a
colorless to slightly yellowish and clear to slightly turbid
solution.
[Profilnine] A few particles may remain in solution
following reconstitution. The Mix2Vial set will remove the
particles and the labeled potency will not be reduced.
Pregnancy Category: C
ATC Code: B02BD04
Indication Bebulin Profilnine
Major surgical
procedures
Typical initial
dose, 75–90
units/kg [raise
factor IX level
to ≥60% of
normal on day
of surgery]
Adjust dose to
typically 25–
75 units/kg for
1–2 weeks
[decrease
factor IX level
to 20–60% of
normal during
initial postop
period]
Adjust dose to
typically 25–
35 units/kg
during late
postop period
(≥3 weeks) and
continue until
adequate
wound healing
is achieved
[further
decrease to
maintain a
factor IX level
of 20% of
normal]
Give preop
dose 1 hour
prior to
surgery,
initially every
12 hours, then
every 24 hours
postop
Initially 30–50
units/kg prior
to surgery
[raise factor IX
level to 30–
50% of normal]
Maintenance
dose, 30–50
units/kg every
16–24 hours
for 7–10 days
following
surgery or until
healing is
achieved
[maintain
factor IX levels
at 30–50% of
normal]](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-104-320.jpg)





![B
BLOOD AND BLOOD FORMING ORGANS
66
Thrombogenic effect: Lenalidomide Thalidomide
(thrombogenic effect)
Administration: May be administered by IV or SC route.
Dissolve powder with full contents in accompanying
solvent ampule. Swirl vial gently until dissolved. Do NOT
shake. Solution should be clear, colorless, and
practically free of particles. Use a 26-gauge needle to
withdraw appropriate amount for a single injection.
Replace needle before injection. Use appropriate size for
injection.
SC route is the preferred route of administration except
in patients with CRF on hemodialysis.
For IV route, administer over a period of 2 minutes. IV is
the preferred route in CRF patients on hemodialysis. May
be injected into the venous line at the end of the dialysis
procedure. In patients treated for increasing autologous
blood, administer after blood is donated.
NOTE: Multi-dose vials contain preservative.
Pregnancy Category: Not available
ATC Code: B03XA01
BLOOD SUBSTITUTES AND PERFUSION
SOLUTIONS
NOTE: All plasma fractions should comply with the WHO
requirements for the Collection, Processing and
Quality Control of Human Blood and Blood Products)
BLOOD AND RELATED PRODUCTS
Rx ALBUMIN, HUMAN
Inj.: 20%, 50 mL and 100 mL bottle (IV, IV infusion)
25%, 50 mL and 100 mL bottle (IV, IV infusion)
25%, 50 mL plastic bag (IV, IV infusion)
A protein colloid prepared as a sterile solution of serum
albumin by fractionating pooled plasma from healthy
human donors. Albumin is the major protein involved in
maintaining colloid osmotic pressure in the blood. It is
used to restore effective plasma circulating volume and
colloid osmotic pressure.
Indication: Management of neonatal hyperbilirubinemia
associated with hemolytic disease of the newborn.
Contraindications: Patients at risk of volume overload (e.g.,
patients with renal impairment, severe anemia, heart
failure); dilution with sterile water for injection.
Dose:
NOTE: Dose depends on the size of the patient, the severity
of trauma or illness, and on continuing fluid and protein
losses. Determine dose required based on measures of
adequacy of circulating volume and NOT plasma albumin
levels.
Hemolytic disease of the newborn, by IV infusion, INFANT, 1
g/kg per dose of 25% albumin prior to or during
exchange transfusion.
Dose Adjustment:
Renal Impairment:
In chronic renal insufficiency, receiving albumin solution
may be at risk for accumulation of aluminum and
potential toxicities.
Precautions:
WARNING: Parenteral product may contain aluminum.
Toxic aluminum concentrations may be seen with
high doses, prolonged use, or renal dysfunction.
Monitor for adequate hydration electrolytes level in patients
receiving hyperosmotic solutions of albumin; Anaphylaxis
(discontinue immediately if allergic or anaphylactic
reactions are suspected); Hemodynamic effects (closely
monitor hemodynamic parameters); Hypervolemia or
hemodilution (use with caution; adjust rate of
administration per hemodynamic status and solution
concentration; observe for signs of hypervolemia, such
as pulmonary edema); Cardiovascular disease (avoid
rapid infusions; may cause circulatory overload and
pulmonary edema; discontinue at first signs of
cardiovascular overload); Hepatic impairment; Renal
impairment; Critical illness; sodium restricted patients
(use with caution); Premature neonates; Lactation (use
with caution).
Adverse Drug Reactions:
Common: Anaphylactoid reactions, fever, chills, rash,
nausea, vomiting, tachycardia, hypotension.
Less Common: Anaphylaxis, urticaria, pruritus,
angioneurotic edema, erythema or flushing, dysguesia,
increased salivation, hyperhidrosis, headache,
confusion, loss of consciousness, pulmonary edema,
dyspnea, bronchospasm.
Rare: Hemolysis
Drug Interactions:
Monitor closely with:
Increase risk of adverse or toxic reactions of the following
drugs:
ACE Inhibitors (flushing, hypotension) [for patients
undergoing therapeutic plasma exchange with human
albumin replacement, withhold ACE inhibitors at least 24
hours prior to plasma exchange]
Administration: For IV administration only. Use within 4
hours after entering package. Discard unused portion. In
emergencies, may administer as rapidly as necessary to
improve clinical condition.
Do NOT use sterile water to dilute albumin solutions, as
this has been associated with hypotonic-associated
hemolysis. Do NOT use with ethanol or protein
hydrolysates as precipitation may form.
Do NOT use solution if it is turbid or contains a deposit.
Use within 4 hours after opening vial. Discard unused
portion.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-110-320.jpg)


![B
BLOOD AND BLOOD FORMING ORGANS
69
Pregnancy Category: No information available
ATC Code: B05AA06
I.V. SOLUTIONS FOR PARENTERAL NUTRITION
Rx
ALL-IN-ONE ADMIXTURES
(3 IN 1 SOLUTIONS /
DUAL ENERGY SOLUTIONS)
Solution: Volume 400 – 2500 mL
Concentration Variable
Protein 3-6 g/100 mL
Carbohydrates 6–15 g/100 mL
Lipid 2–5 g/100 mL
Calories Variable
Electrolytes Variable
A sterile, nonpyrogenic emulsion of essential amino acids,
electrolytes, dextrose, and lipid for central venous
administration, in a three-chamber bag.
Indications: Supply of water, proteins, electrolytes, essential
amino acids & calories to patients by TPN when oral or
enteral nutrition is unfeasible, insufficient, or
contraindicated; prevention of essential fatty acid
deficiency; treatment of negative nitrogen balance in
adult patients.
Contraindications: Hypersensitivity to eggs, soy protein, fat
emulsion, amino acids, or glucose; hyperlipemia; severe
liver insufficiency; blood coagulation disorders;
congenital disorder of amino acid metabolism; severe
renal insufficiency without hemofiltration or dialysis;
acute shock; hyperglycemia requiring insulin over 6 units
hourly; elevated serum levels including electrolytes.
Dose:
NOTE: Individualize dose and infusion rate based on the
ability to eliminate fat and metabolize glucose.
Determine bag size with regard to the clinical condition
of the patient, the body weight and the nutritional
requirements.
Normal nutritional state or under mild catabolic stresses, by
IV drip infusion, ADULT, 0.7–1 g/kg (nitrogen 0.1–0.15
g/kg) daily of amino acids.
Moderate to high catabolic stresses, by IV drip infusion,
ADULT, 1–2 g/kg (nitrogen 0.15–0.3 g/kg); generally,
0.7–1 g/kg daily of total amino acid (nitrogen 0.1–0.15
g/kg) into peripheral or central veins; do not exceed a
rate of 3.7 mL/kg per hour (equivalent to 0.25 g glucose,
0.09 g amino acids, and 0.13 g lipids per kg);
recommended infusion period is 12–24 hours or as
prescribed by the physician.
Dose Adjustment:
Geriatric:
Administer more slowly or at reduced dose.
Precautions:
WARNING: Preterm infants and low birth weight
infants have poor clearance of IV lipid emulsion
and increased free fatty acid plasma levels
following lipid emulsion infusion. Deaths in preterm
infants after infusion of IV lipid emulsions have
been reported.
Special clinical monitoring is required at the beginning of IV
infusion (serum triglyceride level should not exceed 2
mmoL/L in 5–6 hours after the administration). Carefully
monitor serum glucose level, electrolytes, osmolarity,
fluid balance, acid-base status, liver enzyme level
[alkaline phosphatase, alanine aminotransferase (ALT),
and aspartate aminotransferase (AST) during
administration. Should any abnormal sign occur, the
infusion must be stopped.
For long-term administration, consider additional
administration of trace elements (e.g., copper, zinc) due
to increased urinary excretion accompanying IV
administration of amino acids. Monitor blood cell count
and coagulation during long-term administration.
Disorders of lipid metabolism (induced by renal failure,
pancreatitis, impaired liver function, hypothyroidism
accompanied by hypertriglyceridemia); sepsis; lactic
acidosis, insufficient cellular oxygen supply, increased
serum osmolarity; patients who need a fluid
resuscitation; patients with a tendency toward electrolyte
retention.
Renal failure (carefully monitor phosphate and potassium
intake to prevent hyperphosphatemia or hyperkalemia).
Patients under malnutrition state (monitor patients carefully
and fine tune of the amount of additional solutions,
electrolytes, vitamins, and minerals required).
Elderly (adjust dose; reduced physiological activities).
Adverse Drug Reactions:
Common: Transient increase in body temperature.
Less Common: Shivering, chillness, nausea, vomiting.
Rare: Thrombophlebitis, hypersensitivity reactions (e.g.,
anaphylactic reaction, rash, urticaria), respiratory
symptoms (hyperventilation), hypertension or
hypotension, hemolysis, increased reticulocytes,
abdominal pain, headache, fatigue, penile stiffness.
Drug Interactions:
Monitor closely with:
Interferes with lipase system:
Heparin (increases plasma lipolysis due to transient
release of lipoprotein lipase; transient decrease of
triglyceride clearance rate at initial administration),
Insulin
General incompatibilities:
Glucose in solution (may form precipitates)
Reduces therapeutic effect of Coumarin Derivatives:
Vitamin K1 [in soybean oil]
Administration: The solution is for IV infusion ONLY into a
central vein.
Correct any state of electrolyte imbalance prior to initial
administration. Observe strict aseptic procedures during
insertion and manipulation to catheters to avoid
contamination.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-113-320.jpg)









![B
BLOOD AND BLOOD FORMING ORGANS
79
Drugs that can cause hyperkalemia (e.g., suxamethonium,
potassium-sparing diuretics or tacrolimus) - increased
risk of hyperkalemia.
Vitamin D- may induce hypercalcemia.
Administration: The solution is administered IV; do not
administer unless the solution is clear and container is
undamaged.
Pregnancy Category: C
ATC Code:B05BB01
I.V. SOLUTIONS PRODUCING OSMOTIC DIURESIS
Rx MANNITOL
Inj.: 20%, 250 mL and 500 mL bottle (IV)
A hexahydric alcohol related to mannose that acts as an
osmotic agent with little energy value. When given
parenterally, it raises the osmotic pressure of the
plasma, thus drawing water out of body tissues and
producing an osmotic diuresis.
Indications: To reduce cerebral edema; to reduce increased
intraocular pressure; to promote urinary excretion of
toxic substances.
NOTE: NOT recommended to be used for the prevention of
acute renal failure and/or promotion of diuresis.
Contraindications: Hypersensitivity to mannitol or any
component of the formulation; severe renal disease
(anuria); severe dehydration; active intracranial bleeding
except during craniotomy; progressive heart failure,
pulmonary congestion, or renal dysfunction after
administration; severe pulmonary edema or congestion.
Dose:
Increased intracranial pressure, cerebral edema, by IV
injection, ADULT, 0.25–2 g/kg per dose, may repeat
every 6–8 hours, as needed to maintain a serum
osmolality <300-320 mOsm/kg; CHILD, 0.25–1 g/kg per
dose administered over 30–60 minutes, repeat as
needed to maintain a serum osmolality <300–320
mOsm/kg.
Reduction of intraocular pressure, by IV injection, ADULT,
0.25–2 g/kg administered over 30–60 minutes 1–1.5
hours prior to surgery; CHILD, 1 to 2 g/kg or 30–60 g/m2
administered over 30–60 minutes 1–1.5 hours prior to
surgery.
Reduction of intraocular pressure, traumatic hyphema, by IV
injection, ADULT, 1.5 g/kg administered over 45 minutes
twice daily for IOP >35 mmHg; may administer every 8
hours; CHILD, 1.5 g/kg administered over 45 minutes
twice daily for IOP >35 mmHg; may administer every 8
hours in patients with extremely high pressure.
Dose Adjustment:
Geriatric:
Consider initiation at lower end of dosing range.
Small and/ or debilitated patients:
Consider giving 500 mg/kg.
Precautions:
WARNING: Use caution in patients with underlying
renal disease. May be used to reduce the incidence
of acute tubular necrosis when administered prior
to revascularization during kidney transplantation.
Carefully monitor fluid balance, electrolytes, renal function,
and vital signs during infusion to prevent fluid and
electrolyte imbalance, including circulatory overload and
tissue dehydration; Extravasation (vesicant at
concentrations >5%; ensure proper catheter or needle
position prior to and during IV infusion); fluid or
electrolyte loss (close medical supervision and dose
evaluation are required; adjust dose to avoid
dehydration); Nephrotoxicity (use caution in patients
taking other nephrotoxic agents, with sepsis or
preexisting renal disease; maintain serum osmolality
less than 320 mOsm/L to minimize adverse effects;
discontinue if evidence of acute tubular necrosis occurs);
Cerebral edema; cardiovascular status should also be
evaluated; Lactation (use with caution).
Adverse Drug Reactions:
Common: Fluid and electrolyte imbalance including
circulatory overload and acidosis (large doses), nausea,
vomiting, thirst, headache, dizziness, chills, fever,
tachycardia, chest pain, hyponatremia, dehydration,
blurred vision, urticaria, hypotension or hypertension,
hypersensitivity reactions, extravasation (leading to
edema and skin necrosis), thrombophlebitis.
Rare: Acute renal failure (large doses)
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Mannitol:
Barbiturates (hypotensive effect)
Brimonidine, topical (hypotensive effect)
MAO Inhibitors (hypotensive effect)
Nicorandil (hypotensive effect)
Pentoxifylline (antihypertensive effect)
Phosphodiesterase-5 Inhibitors (antihypertensive effect)
Prostacyclin Analogues (hypotensive effect)
Enhances therapeutic effect of the following drugs:
Alfuzosin (hypotensive effect), Other Antihypertensives
(hypotensive effect), Herbs with hypertensive properties
(hypotensive effect), Risperidone (hypotensive effect)
Increases risk of adverse or toxic effects of Mannitol:
Opioid Analgesics, Other Hypotensive Agents, MAO
Inhibitors [except Linezolid, Tedizolid] (orthostatic
hypotensive effect)
Increases risk of adverse or toxic effects of the following
drugs:
Duloxetine (orthostatic hypotensive effect)
Levodopa (orthostatic hypotensive effect)
Reduces therapeutic effect of Mannitol:
Herbs with hypertensive properties (antihypertensive
effect)
Methylphenidate (antihypertensive effect)](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-123-320.jpg)
![B
BLOOD AND BLOOD FORMING ORGANS
80
Avoid concomitant use with:
Increases risk of adverse or toxic effects of the following
drugs:
Aminoglycosides (nephrotoxic effect)
Obinutuzumab [withhold Mannitol 12 hours prior to
Obinutuzumab infusion until 1 hour after the end of the
infusion] (hypotensive effect)
Rituximab (hypotensive effect)
Sodium Phosphates (nephrotoxic effect; risk of acute
phosphate nephropathy)
Administration: For IV administration. Determine
concentration and rate of administration based on
indication or severity or adjust to urine flow.
Inspect for crystals prior to administration. If crystals are
present, re-dissolve by warming solution. Use filter type
administration set for infusion solutions containing
≥20% Mannitol.
Do NOT administer until adequacy of renal function and
urine flow is established. Use 1–2 test doses to assess
renal response.
Do NOT administer electrolyte-free mannitol solutions
with blood. NEVER add to whole blood for transfusion or
administer through the same set by which blood is being
infused to prevent crenation and agglutination of RBC.
Pregnancy Category: C
ATC Code: B05BC01
IRRIGATING SOLUTIONS
Rx
INTRAOCULAR IRRIGATING
SOLUTION
(BALANCED SALT SOLUTION)
Solution: 15 mL, 250 mL, and 500 mL bottle
Composition:
Sodium chloride 0.64%
Potassium chloride 0.075%
Calcium chloride 0.048%
Magnesium chloride
(hexahydrate) 0.03%
Sodium acetate 0.39%
Sodium citrate 0.17%
Water for injection to make 100%
A sterile, isotonic, balanced salt solution for use in irrigating
tissues of the eyes.
Indications: Extraocular and intraocular irrigating solution
during ocular surgical procedure involving the anterior
chamber (e.g., cataract and glaucoma surgeries) and
vitreous cavity (e.g., vitrectomy); for perfusion of the eye
with an expected maximum duration of <60 minutes.
Contraindications: No information available
Dose: For use as an irrigant during ocular surgery, consult
specialized references for proper use during various
ocular surgery types.
Precautions:
WARNING: Open under aseptic conditions only.
Corneal clouding and edema; Diabetes (use with caution in
patients undergoing vitrectomy).
Adverse Drug Reactions: Corneal swelling or bullous
keratopathy (prolonged procedures), inflammatory
reactions (post-operative), corneal edema (post-
operative), corneal decompensation (post-operative)
NOTE: Use proper solution in accordance to the surgical
procedure to prevent cytotoxic effects.
Drug Interactions: No information found
Administration: Use according to standard format for each
surgical procedure. For single patient use only. This
solution contains no preservative. Discard unused
portion.
Use an administration set with an air-inlet in the plastic
spike since the bottle does not contain a separate airway
tube. Follow directions of the administration set to be
used. Remove blue flip-off cap. Clean and disinfect the
rubber stopper using a sterile alcohol wipe. Insert the
spike aseptically into the bottle through the target area
of the rubber stopper. Allow the fluid to flow and remove
air from the tubing before irrigation.
Do NOT use unless product is clear, seal is intact,
vacuum is present, and container is undamaged. Do NOT
use if product is discolored or contains a precipitate.
Pregnancy Category: C
ATC Code: B05CX10
PERITONEAL DIALYTICS
Rx PERITONEAL DIALYSIS SOLUTION
Solution: Sterile with 1.5%, 2.3%, 2.5% and 4.25%
dextrose, 2 L and 5 L bottle/bag
Content per liter:
Glucose monohydrate 16.5 g
(equivalent to 15.0 g glucose)
Fructose up to 0.75 g
Sodium chloride 5.786 g
Sodium (S) – lactate solution 7.85 g
(equivalent to 3.925 g sodium (S) – lactate)
Calcium chloride dihydrate 183.8 mg
Magnesium chloride hexahydrate 101.7 mg
A sterile, nonpyrogenic solution containing electrolytes at a
concentration close to the electrolytic composition of
plasma and glucose in varying concentrations or other
suitable osmotic agents. It is used for peritoneal dialysis,](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-124-320.jpg)

![B
BLOOD AND BLOOD FORMING ORGANS
83
Rx 10% DEXTROSE IN WATER
Inj.: 250 mL, 500 mL, and 1 L bottle / bag (IV infusion)
3 mL ampule (as solvent)
A sterile, non-pyrogenic, hypertonic solution of Dextrose,
USP in water for injection for intravenous administration
after appropriate admixture or dilution.
Indications: Source of water and calories; parenteral
nutrient, indicated as a caloric component in a
parenteral nutrition regimen; used with an appropriate
protein (nitrogen) source in the prevention of nitrogen
loss or in the treatment of negative nitrogen balance in
patients where:
(1) alimentary tract cannot or should not be used,
(2) GI absorption of protein is impaired, or
(3) metabolic requirements for protein are substantially
increased, as with extensive burns.
Contraindications: Intracranial or intraspinal hemorrhage;
severe dehydration; anuric; hepatic coma.
Dose: Dose is usually dependent upon the age, weight, and
clinical condition of the patient, as well as laboratory
determinations.
NOTE: Use with caution in infants of diabetic mothers,
except as may be indicated in hypoglycemic neonates.
Precautions:
WARNING: Contains aluminum that may be toxic. May
reach toxic aluminum levels with prolonged use if
kidney function is impaired.
Administration by central venous catheter should
be used only by those familiar with this technique
and its complications.
Overt or subclinical diabetes mellitus or carbohydrate
intolerance (use with caution); hyperglycemia and
glycosuria (slow the infusion rate to minimize these
conditions; monitor blood and urine glucose); vitamin B-
complex deficiency; Acute ischemic stroke (do not use
after acute ischemic strokes); cardiac insufficiency (use
with caution to avoid circulatory overload); Hypokalemia;
IV injections can cause fluid and/or solute overload
resulting in dilution of serum electrolyte concentrations,
overhydration, congested states, or pulmonary edema;
Clinical evaluation and periodic laboratory
determinations are necessary to monitor changes in fluid
balance, electrolyte concentrations, and acid-base
balance during prolonged parenteral therapy, or
whenever the condition of the patient warrants such
evaluation; Elderly and children (administer with
caution); premature neonates.
Adverse Drug Reactions: Febrile response, infection at the
site of injection, venous thrombosis or phlebitis
extending from the site of injection, extravasation,
hypervolemia [NOTE: May occur because of the solution or the
technique of administration].
Hyperosmolar syndrome (excessively rapid
administration), hypovolemia, dehydration, mental
confusion, and/or loss of consciousness, diuresis (too
rapid infusion), hyperglycemia (too rapid infusion),
glycosuria (too rapid infusion), hyperosmolar coma (too
rapid infusion)
NOTE: If an adverse reaction occurs, discontinue the
infusion, evaluate the patient, institute appropriate
therapeutic countermeasures and save the remainder of
the fluid for examination, if deemed necessary.
Drug Interactions:
Monitor closely with:
Increases risk of hypertension and edema of the following
drugs due to sodium and water retention:
Corticosteroids
NOTE: Additives may be incompatible. Consult a pharmacist.
If additives are to be introduced, use aseptic technique.
Administration: For IV administration only. Contains no
bacteriostat, antimicrobial agent or added buffer. For
use only as a single-dose injection following admixture or
dilution.
Inspect visually for particulate matter and discoloration
prior to administration. Do NOT administer unless
solution is clear and seal is intact.
Prior to administration, dilute to a concentration which,
when administered with an amino acid (nitrogen) source,
will result in an appropriate calorie-to-gram nitrogen
ratio, and which has an osmolarity consistent with the
route of administration.
NOTE: Unless appropriately diluted, hypertonic dextrose
infusion into a peripheral vein may result in vein
irritation, vein damage, and thrombosis. Strongly
hypertonic nutrient solutions should be administered
through an indwelling IV catheter with the tip located in
a large central vein such as the superior vena cava.
Use a final filter during administration. Slowly inject the
solution at a rate not exceeding 0.5 g/kg body weight per
hour.
NOTE: About 95% of the dextrose is retained when infused
at a rate of 0.8 g/kg/hour.
Do NOT administer by SC or IM route.
Do NOT administer simultaneously with blood through
the same administration set because of the possibility of
pseudo-agglutination or hemolysis.
NOTE: All injections in plastic containers are intended for IV
administration using sterile equipment. Replace IV
administration apparatus at least once every 24 hours.
Interruption or rapid cessation of hypertonic dextrose
therapy may result in a hypoglycemic reaction. Titrate
with a dilute dextrose solution until the patient has
reached glucose equilibrium.
Pregnancy Category: C](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-127-320.jpg)


![B
BLOOD AND BLOOD FORMING ORGANS
87
Hypomagnesemia seizures, mild, by IV or IM injection,
ADULT, 1 g every 6 hours for 4 doses.
Hypomagnesemia seizures, mild, by IV or IM injection,
ADULT, 250 mg/kg infused over 4 hours.
Hypomagnesemia seizures, by IV injection, CHILD, 20–100
mg/kg every 4–6 hours, or as needed.
Hypomagnesemia seizures, severe, by IV or IM injection,
ADULT, 1–2 g/hour for 3–6 hours, then 0.5–1 g/hour as
needed based on serum magnesium levels.
Dose Adjustment:
Geriatric and Renal Impairment:
Reduce dose. Up to 50% of an IV dose may be eliminated in
the urine.
For patients with renal disease, Do NOT exceed 20 g every
48 hours for patients with renal disease.
Precautions:
WARNING: Toxicity causes loss of deep tendon
reflexes, followed by respiratory depression and
ultimately respiratory arrest. If deep tendon
reflexes are absent, withhold further doses until
reflexes return. Toxicity can be reversed with
calcium gluconate.
Magnesium is excreted by the kidney. Monitor
regularly serum levels in women with oliguria (urine
output <100 mL/4 hours). If repeated seizures
occur despite magnesium, other pre-hospital
options include administering diazepam.
Myasthenia gravis or other neuromuscular disease (use
with extreme caution); Renal impairment (use with
caution); Electrolyte abnormalities; Magnesium toxicity;
Pregnancy (monitor mother and fetus closely; do not use
for longer than 5–7 days to prevent adverse fetal
events).
Adverse Drug Reactions:
Common: Flushing, nausea, vomiting
Less Common: Dizziness, drowsiness, headache, thirst
Rare: Arrhythmias, cardiac arrest, coma, confusion,
loss of tendon reflexes, muscle weakness,
respiratory depression
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Magnesium Sulfate:
Aminoglycosides (additive neuromuscular blocking
effect)
Enhances therapeutic effect of the following drugs:
Calcium Channel Blockers (hypotensive effect)
CNS Depressants, e.g., Barbiturates, Opiates, General
Aesthetics (CNS depressant effects)
Neuromuscular Blocking Agents, e.g., Tubocurarine,
Vecuronium, Succinylcholine (neuromuscular blocking
effect)
Increases risk of adverse or toxic effects of Magnesium
Sulfate:
Calcium Channel Blockers
Avoid concomitant use with:
Decreases absorption of Magnesium Sulfate:
Alpha-Lipoic Acid
Decreases absorption of the following drugs:
Alpha-Lipoic Acid, Multivitamins / Fluoride with ADE
(fluoride absorption) [separate administration by at least
1 hour]
Decreases serum concentration of the following drugs:
Bisphosphonate Derivatives [except Pamidronate,
Zoledronic Acid], Deferiprone, Dolutegravir,
Eltrombopag, Gabapentin, Levothyroxine, Multivitamins
/ Fluoride with ADE, Quinolone Antibiotics, Raltegravir
Enhances therapeutic effect of the following drugs:
Gabapentin (CNS depressant effect)
Increases serum concentration of Magnesium Sulfate:
Alfacalcidol, Calcitriol (systemic)
Administration: Administer at a concentration not exceeding
20%. Dilute according to manufacturer’s instructions.
For IM route, solutions may need dilution prior to
administration. 25% or 50% for adults or ≤20% for
children.
For IV route, solutions must be diluted to ≤20% for IV
infusion and may be administered by IV push, IVPB, or
continuous IV infusion.
For IV push, dilute first and do not administer faster than
150 mg/minute.
May be administered over 1–2 minutes in patients with
persistent pulseless VT or VF with known
hypomagnesemia. Administer over 15 minutes in
patients with torsade de pointes.
Maximum rate of infusion is 1 g/hour in asymptomatic
patients. For doses <6 g, infuse over 8–12 hours. For
larger doses, infuse over 24 hours.
If patient is severely symptomatic or has conditions such
as preeclampsia or eclampsia, more aggressive therapy
(≤4 g over 4-5 minutes) may be required.
Pregnancy Category: A
ATC Code: B05XA05
Rx POTASSIUM CHLORIDE
Oral: 600 mg tablet
750 mg durules (equiv. to approximately 10 mEq
potassium)
1 mmol/mL syrup, 30 mL and 60 mL
Inj.: 2 mEq/mL, 2 mL and 5 mL ampule (IV infusion)
2 mEq/mL, 10 mL and 20 mL vial (IV infusion)
A sterile preparation that contains potassium chloride,
utilized for the treatment of hypokalemia.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-131-320.jpg)


![B
BLOOD AND BLOOD FORMING ORGANS
90
Do not exceed 50 mEq/hour. Stop infusion immediately
if extravasation occurs. Flush IV line thoroughly before
and after administration.
WARNING: Rapid or excessive administration may
produce alkalosis, hypokalemia, and hypocalcemia.
Cardiac arrhythmias may result from an intracellular
shift of potassium. Many other complications may
arise from electrolyte imbalance.
See Sodium Bicarbonate under Antacids in Chapter 1:
Alimentary Tract and Metabolism for other information.
Pregnancy Category: C
ATC Code: B05XA02
Rx SODIUM CHLORIDE
Inj.: 2.5 mEq/mL, 20 mL and 50 mL vial
A sterile, non-pyrogenic, concentrated solution of
sodium chloride administered to replenish electrolytes.
Indication: Hyponatremia with overt manifestations.
Contraindications: Where the administration of
sodium or chloride could be clinically detrimental (e.g.,
hypernatremia); fluid retention; hypertension; CHF.
Dose: Dose is dependent on degree of sodium depletion
(i.e., moderately severe hyponatremia where serum
sodium is between 125–129 mmol/L or profound
hyponatremia where serum sodium is <125 mmol/L); on
severity of symptoms (i.e., moderately or severely
symptomatic); and on time of development of
hyponatremia (acute, where hyponatremia is
documented to exist <48hrs).
IMPORTANT NOTE: Sodium deficit must be corrected
gradually in stages. Avoid overtly rapid correction to
prevent development of Osmotic Demyelination
Syndrome (previously named Central Pontine
Myelinosis). The rate of correction of hyponatremia
should not be more than 10 mmol/L (or 10 mEq/L) in 24
hours, or 18 mmol/L (or 10 mEq/L) in 48 hours.
Dose Adjustment:
Renal Impairment:
Select doses with caution due to potential to
result in sodium retention and increased risk
of adverse effects.
Precautions:
WARNING: Contains aluminum, which may be toxic. May
reach toxic aluminum levels with prolonged use,
especially if kidney function is impaired.
Monitor fluid balance, electrolyte concentration, and
acid-base balance; observe for hypernatremia, water
retention and pulmonary edema; restrict in patients with
renal insufficiency or failure, cardiac failure,
hypertension, peripheral and pulmonary edema, or
toxemia of pregnancy; Seizures or neurologic deficit
(requires aggressive therapy); IV administration can
cause fluid and/ or solute overloading resulting in
dilution of other electrolyte concentration, overhydration,
congested states or pulmonary edema; excessive
administration of potassium-free solutions may result in
significant hypokalemia; Premature neonates.
Adverse Drug Reactions: Air embolization, febrile response,
local tenderness, tissue necrosis or infection at the site
of injection, venous thrombosis or phlebitis extending
from the site of injection, extravasation [NOTE: May occur
because of the solution, added drugs or the technique of
reconstitution or administration].
Rare: Edema, sodium accumulation
Drug Interactions:
Monitor closely with:
Increases risk of hypertension and edema of the following
drugs due to sodium and water retention:
Corticosteroids e.g. Prednisone
Administration: Administer based on calculated dose
requirements for each patient. Must be diluted before
infusion to avoid a sudden increase in the plasma-
sodium level. Too rapid administration should be avoided
[see Important Note under Dose].
Inspect visually for particulate matter and discoloration
prior to administration. Do NOT use unless the solution
is clear, and seal is intact. Discard unused portion.
Pregnancy Category: C
ATC Code: B05XA03
Rx STERILE WATER FOR INJECTION
Inj.: 2 mL, 5 mL, 10 mL, and 20 mL ampule
50 mL, 100 mL, 500 mL, and 1 L bottle / bag (no
preservative)
A sterile, nonpyrogenic water for injection that does
not contain any antimicrobial agent or other
added substances, such as buffer, and is
supplied in single-dose containers to dilute or
dissolve drugs for injection.
Indication: For dissolving or diluting medicines that are
intended for parenteral injection.
NOTE: Use in accordance with the instructions set by the
manufacturer of the drug.
Contraindications: No information found
Dose: Volume to be used for any drug for injection is based
on the vehicle concentration, dose, and route of
administration as recommended by the drug
manufacturer.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-134-320.jpg)






![C
CARDIOVASCULAR SYSTEM
98
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Propranolol:
Bradycardic effect: Acetylcholinesterase Inhibitors e.g.
Neostigmine, Amiodarone (may induce cardiac arrest),
Bretylium, Dipyridamole, Disopyramide, Regorafenib,
Reserpine, Ruxolitinib, Tofacitinib, Other Bradycardia-
causing Agents
Antihypertensive effect: Phenothiazine Antipsychotic
Agents, Barbiturates e.g Phenobarbital, Brimonidine
(topical), Calcium Channel Blockers (Non-
Dihydropyridine e.g. Verapamil), Diazoxide, Lacidipine,
Molsidomine, Nicorandil, Nifedipine (also negative
inotropic effect), Pentoxifylline, Phosphodiesterase-5
Inhibitors, Prostacyclin Analogues e.g., Epoprostenol,
Propafenone (possesses independent beta-blocking
activity), Anilidopiperidine Opioids e.g., Fentanyl
(bradycardic and hypotensive effects),
Enhances therapeutic effect of the following drugs:
Bretylium (AV blockade), Cardiac Glycosides (bradycardic
effect), Disopyramide (negative inotropic effect),
Fingolimod (bradycardic effect), Insulin (hypoglycemic
effect), Ivabradine (bradycardic effect), Lacosamide (AV
blocking effect), Midodrine (bradycardic effect), Other
Antihypertensives (antihypertensive effect),
Sulfonylureas (hypoglycemic effect)
Increases metabolism of Propranolol:
CYP1A2 Inducers, CYP2D6 Inducers
Increases risk of adverse or toxic effects of Propranolol:
MAO Inhibitors (orthostatic hypotensive effect)
Increases risk of adverse or toxic effects of the following
drugs:
Cholinergic Agonists (potential for cardiac conduction
abnormalities and bronchoconstriction), Duloxetine
(orthostatic hypotensive effect), Levodopa (orthostatic
hypotensive effect), MAO Inhibitors [except Linezolid,
Tedizolid] (orthostatic hypotensive effect), Other
Antihypertensive Agents
Reduces therapeutic effect (anti-hypertensive effect) of
Propranolol:
Methylphenidate (antihypertensive effect), NSAIDS
(antihypertensive effect)
Avoid concomitant use with:
Enhances therapeutic effect of Propranolol:
Alpha2agonists [except Apraclonidine] (AV blocking
effect), Dronedarone (bradycardic effect), Rivastigmine
(bradycardic effect)
Enhances therapeutic effect of the following drugs:
Alpha / Beta-Agonists, Direct-Acting (vasopressor effect)
Ceritinib (bradycardic effect), Ergot Derivatives e.g.,
Ergotamine (vasoconstricting effect)
Increases metabolism of Propranolol:
CYP1A2 Inducers, CYP2D6 Inducers
Increases risk of adverse or toxic effects of the following
drugs:
Alpha / Beta-Agonists, Direct-Acting (reduced beta-
adrenoceptor-mediated effects, including anaphylactic
effects of epinephrine), Alpha1 Blocker e.g. Tamsulosin
(orthostatic hypotensive effect), Alpha2agonists [except
Apraclonidine] (rebound hypertension; may enhance
sinus node dysfunction), Amifostine (hypotensive
effect), Grass Pollen Allergen Extract / 5 Grass Extract
(may inhibit the ability to effectively treat severe allergic
reactions with epinephrine), Methacholine,
Obinutuzumab (hypotensive effect), Rituximab
(hypotensive effect)
Increases serum concentration of Propranolol:
Abiratone Acetate, Dronedarone, Fluvoxamine,
Panobinostat
Increases serum concentration of the following drugs:
Afatinib, Bosutinib, Colchicine (may increase distribution
to certain tissues, e.g., brain), Dabagitran Etexilate
[active metabolites], Doxorubicin (Conventional),
Edoxaban, Everolimus, Pazopanib, Rizatriptan [reduce
dose to 5 mg when used concomitantly], Silodosin,
Tizanidine, Topotecan, Vemurafenib, Vincristine
(Liposomal)
Reduces therapeutic effect of the following drugs:
Beta2agonists e.g Salbutamol (bronchodilatory effect),
Theophylline Derivatives e.g., Aminophylline
(bronchodilatory effect)
Administration: To be taken on an empty stomach.
NOTE: Do NOT withdraw abruptly, particularly in patients
with CAD. Gradually taper dose to avoid acute
tachycardia, hypertension, and/or ischemia.
Pregnancy Category: C
ATC Code: C07AA05
CLASS III ANTIARRHYTHMICS
Rx AMIODARONE
Oral: 200 mg tablet (as hydrochloride)
Inj.: 50 mg/mL (as hydrochloride), 3 mL ampule (IV)
A class III antiarrhythmic agent with alpha- and beta-
blocking properties, that acts by inhibiting adrenergic
stimulation. Amiodarone affects sodium, potassium, and
calcium channels and prolongs the action potential
duration and refractory period in myocardial tissue. It
also decreases AV conduction and sinus node function.
Indications: Management of life-threatening recurrent
ventricular fibrillation (VF) or recurrent hemodynamically-
unstable ventricular tachycardia (VT); supraventricular
arrhythmias
Contraindications: Severe sinus-node dysfunction causing
marked sinus bradycardia; second- and third-degree
heart block; bradycardia causing syncope; cardiogenic
shock](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-142-320.jpg)
![C
CARDIOVASCULAR SYSTEM
99
Dose:
Recurrent life-threatening ventricular arrhythmias,
prevention, by mouth, ADULT, 800–1,600 mg daily in 1–
2 doses for 1–3 weeks; when adequate arrhythmia
control is achieved, decrease to 600–800 mg daily in 1–
2 doses for 1 month (maintenance, 300 mg daily).
Pulseless VT or VF, by IV push, I.O., ADULT, initially 300 mg
rapid bolus; if condition continues or recurs, administer
supplemental dose of 150 mg, preferably undiluted
(maximum recommended total daily dose, 2.2 g); once
spontaneous circulation returns, administer by IV
infusion of 1 mg/minute for 6 hours, then 0.5 mg/minute
for 18 hours); CHILD, 5 mg/kg rapid bolus (maximum,
300 mg per dose); may repeat twice up to a maximum
total dose of 15 mg/kg during acute treatment.
Stable VT, by IV infusion, ADULT, 150 mg over 10 minutes,
then 1 mg/minute for 6 hours, followed by 0.5
mg/minute; continue this rate for at least 18 hours or
until complete transition to oral (total infusion duration,
24 hours).
Breakthrough stable VT, by IV infusion, ADULT, 150 mg
supplemental doses in 100 mL D5W or NS over 10
minutes [NOTE: Mean daily doses >2.1 g/day have been
associated with hypotension.]
Atrial fibrillation, pharmacologic cardioversion, by mouth,
ADULT, 600–800 mg daily in divided doses to a total of
10 g, then 200 mg daily as maintenance dose (usual
maintenance dose, 100 mg daily); or
800 mg daily for 14 days, followed by 600 mg daily for
the next 14 days, then 300 mg daily for the remainder of
the first year, then 200 mg daily thereafter; or
10 mg/kg daily for 14 days, followed by 300 mg daily for
4 weeks, then 200 mg daily as maintenance dose;
by IV infusion, ADULT, 150 mg over 10 minutes, then 1
mg/minute for 6 hours, then 0.5 mg/minute for 18
hours, or change to oral dosing.
Maintenance of sinus rhythm, by mouth, ADULT, 400 to 600
mg daily in divided doses for 2–4 weeks followed by a
maintenance dose of 100–200 mg once daily.
Prevention of postoperative atrial fibrillation and atrial
flutter associated with cardiothoracic surgery, by mouth,
ADULT, 200 mg 3 times daily for 7 days prior to surgery,
followed by 200 mg daily until hospital discharge;
by IV injection, ADULT, 150 mg loading dose, followed by
0.4 mg/kg per hour for 3 days prior to surgery and for 5
days postoperative; after surgery, infuse 1,000 mg over
24 hours for 2 days.
Supraventricular tachycardia, pharmacologic cardioversion,
by mouth, ADULT, 600–800 mg daily in divided doses to
a total of 10 g, then 200 mg daily as maintenance;
by IV infusion, ADULT, 150 mg over 10 minutes, then 1
mg/minute for 6 hours, then 0.5 mg/minute for 18
hours, or change to oral dosing.
Dose Adjustment:
Geriatric:
Select doses with caution. Begin at low end of dosage range
and titrate slowly to evaluate response.
A maintenance dose of 100 mg daily is commonly used
especially for the elderly or patients with low body mass.
Hepatic Impairment:
Dose adjustment may be necessary. Decrease dose or
discontinue Amiodarone once hepatic enzymes exceed 3
times the normal or double in a patient with an elevated
baseline.
Precautions:
WARNING: For use only in patients with indicated life-
threatening arrhythmias due to the risk for
substantial, potentially fatal toxicity (e.g.,
pulmonary toxicity, overt liver disease).
Bradycardia or hypotension (infusion-rate related);
Proarrhythmic effects
Arrhythmias (hospitalize patients when amiodarone is
initiated), Wolff-Parkinson-White (WPW) syndrome
Cardiac devices, e.g., implantable defibrillators (chronic
therapy may increase defibrillation threshold)
Myocardial infarction
Dermatologic toxicity (may cause life-threatening or fatal
cutaneous reactions, including SJS and TEN)
photosensitivity (blue-gray discoloration of exposed skin
may occur during long-term treatment)
Hepatotoxicity
Neurotoxicity (peripheral neuropathy has been reported);
ocular effects (may cause optic neuropathy and/or optic
neuritis resulting in visual impairment; permanent
blindness has occurred; corneal microdeposits
commonly occur and may cause reversible visual
disturbances)
Pulmonary toxicity (hypersensitivity pneumonitis, or
interstitial or alveolar pneumonitis, and abnormal
diffusion capacity without symptoms may occur; acute-
onset pulmonary injury has occurred; most fatalities due
to sudden cardiac death occurred when amiodarone was
discontinued)
Thyroid effects (may cause hyper or hypothyroidism;
myxedema has been reported and may be fatal; thyroid
nodules and thyroid cancer have been reported)
Electrolyte imbalance (correct hypokalemia,
hypomagnesemia, or hypocalcemia prior to use and
throughout therapy)
Surgical patients (may enhance myocardial depressant and
conduction effects of halogenated inhalational
anesthetics; adult respiratory distress syndrome (ARDS)
has been reported postoperatively)
Elderly (use is associated with thyroid disease, pulmonary
abnormalities, and QT-interval prolongation)
Lactation (excreted in breastmilk; not recommended for
nursing mothers).
Adverse Drug Reactions:
Common: Hypotension, bradycardia, AV block, cardiac
arrest, cardiac arrhythmia, cardiac failure, ventricular
tachycardia, asystole, atrial fibrillation, cardiogenic
shock, torsade de pointes, ventricular fibrillation,
atrioventricular dissociation, cardiac conduction
disturbance, edema, flushing, peripheral
thrombophlebitis, pulseless electrical activity (PEA),
abnormal gait, ataxia, dizziness, fatigue, involuntary
body movements, malaise, peripheral neuropathy,
memory impairment, paresthesia, altered sense of
smell, headache, insomnia, sleep disorder, blue-gray
skin pigmentation, skin photosensitivity, hypothyroidism,
decreased libido, hyperthyroidism nausea, vomiting,
anorexia, constipation, altered salivation, dysgeusia,
abdominal pain, diarrhea, blood coagulation disorder,
hepatic disease, tremor, corneal deposits, visual halos,
visual disturbance, optic neuritis, photophobia,
pulmonary toxicity, pulmonary edema, hypersensitivity](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-143-320.jpg)
![C
CARDIOVASCULAR SYSTEM
100
pneumonitis, interstitial pneumonitis, pulmonary
fibrosis, fever
Less Common: Acute renal failure, adult respiratory distress
syndrome, agranulocytosis, alopecia, anaphylactic
shock, anaphylactoid reaction, anaphylaxis,
angioedema, aplastic anemia, back pain, bronchiolitis
obliterans organizing pneumonia, bronchospasm,
bullous dermatitis, cholestasis, cholestatic hepatitis,
confusion, cough, delirium, demyelinating
polyneuropathy, disorientation, DRESS syndrome, drug-
induced Parkinson disease, dyspnea, eczema,
eosinophilic pneumonia, epididymitis, erythema
multiforme, exfoliation of skin, exfoliative dermatitis,
fever, hallucination, hemolytic anemia, hemoptysis,
hepatic cirrhosis, hepatic failure, hepatitis,
hepatotoxicity (idiosyncratic), hypoesthesia,
hypotension, hypoxia, impotence, increased intracranial
pressure, injection site reaction, jaundice,
leukocytoclastic vasculitis, malignant neoplasm of skin,
pulmonary mass, myasthenia, myopathy, neutropenia,
optic neuropathy, pancreatitis, pancytopenia, pleural
effusion, pleurisy, prolonged QT interval, pruritus,
pseudotumor cerebri, pulmonary alveolar hemorrhage,
pulmonary infiltrates, pulmonary phospholipidosis, renal
insufficiency, respiratory arrest, respiratory distress
syndrome, respiratory failure, rhabdomyolysis, SIADH,
sinoatrial arrest, sinus node dysfunction, skin carcinoma,
skin granuloma, skin rash, skin sclerosis, spontaneous
ecchymoses, Stevens-Johnson syndrome, superior vena
cava syndrome, thrombocytopenia, thyroid cancer,
thyroid nodule, thyrotoxicosis, tissue necrosis at injection
site, toxic epidermal necrolysis, urticaria, vasculitis,
vortex keratopathy, wheezing, xerostomia
Drug Interactions:
Monitor closely with:
Decreases absorption of Amiodarone:
Orlistat
Decreases metabolism of Tramadol
Enhances therapeutic effect of Amiodarone:
Bretylium (bradycardic and AV blocking effects),
Lidocaine (arrhythmogenic effect), Ruxolitinib
(bradycardic effect)
Tofacitinib (bradycardic effect)
Enhances therapeutic effect of the following drugs:
Beta Blockers [except Levobunolol, Metipranolol]
(bradycardic effect), Bradycardia-causing Agents
(bradycardic effect), Lacosamide (AV blocking effect)
Increases risk of adverse or toxic effects of Amiodarone:
Cyclophosphamide (pulmonary toxicity), Porfimer
(photosensitizing effect), Telaprevir, Verteporfin
(photosensitizing effect)
Reduces therapeutic effect of the following drugs:
Codeine, Tramadol (opioid-like effects)
Avoid concomitant use with:
Decreases bioavailability of Amiodarone:
Bile acid sequestrants
Decreases metabolism of Amiodarone:
Grapefruit Juice
Decreases metabolism of the following drugs:
Cyclosporine (Systemic), HMG-CoA Reductase Inhibitors
[except Pitavastatin, Pravastatin; limit Simvastatin adult
maximum dose to 20 mg daily; limit Lovastatin adult
maximum dose to 40 mg daily], Tamoxifen, Tegafur
Decreases serum concentration of Amiodarone:
Dabrafenib, Fosphenytoin, Mitotane, Rifampin [including
its active metabolite, desethylamiodarone],
Decreases serum concentration of the following drugs:
Artesunate, Tamoxifen, Tegafur
Enhances therapeutic effect of Amiodarone:
QTc prolonging effect: Azithromycin (Systemic),
Fosphenytoin
Bradycardic effect: Non-Dihydropyrdine Calcium Channel
Blockers e.g., Diltiazem, Daclatasvir
Arrhythmogenic effect: Fingolimod
Enhances therapeutic effect of Amiodarone:
QTc prolonging effect: Ivabradine, Lopinavir,
Mifepristone, Other QTc-prolonging Agents, Saquinavir,
Bradycardic effect: Sofosbuvir
Enhances therapeutic effect of the following drugs:
Antiarrhythmic Agents, Class Ia (QTc prolonging effect),
Ceritinib (bradycardic effect), Flecainide [when used
concomitantly, decrease Flecainide dose by 50%] (QTc
prolonging effect), Vitamin K Antagonists, e.g., Warfarin
(anticoagulant effect)
Increases bioavailability of Amiodarone:
Grapefruit Juice
Increases risk of adverse or toxic effects of the following
drugs:
Loratadine (QT interval prolongation and torsade de
pointes), Propafenone (cardiac conduction and
repolarization)
Increases serum concentration of Amiodarone:
Cimetidine, Fusidic Acid (Systemic) Idelalisib, Indinavir,
Lopinavir, Nelfinavir, Ritonavir, Saquinavir, Tipranavir
Increases serum concentration of the following drugs:
Afatinib [reduce Afatinib dose by 10 mg if not tolerated],
Antiarrhythmic Agents, Class Ia e.g. Procainamide,
Artesunate, Bosutinib, Cardiac Glycosides e,g, Digoxin
[when used concomitantly, reduce Cardiac Glycosides
dose by 30-50% or reduce frequency of administration],
Colchicine (may increase colchicine distribution into
certain tissues, e.g., brain), Dabigatran Etexilate,
Doxorubicin (Conventional), Everolimus, Flecainide
[when used concomitantly, decrease Flecainide dose by
50%], Lomitapide [limit maximum dose to 30 mg daily],
Loratadine, Metoprolol, Pazopanib, Pimozide,
Propafenone, Silodosin, Thioridazine, Tizanidine [if
concomitant use cannot be avoided, initiate Tizanidine
at an adult dose of 2 mg and increase in 2–4 mg
increments based on patient response], Topotecan,
Vincristine (Liposomal), Vitamin K Antagonists, e.g.,
Warfarin
Reduces therapeutic effect of the following drugs:
Agalsidase Alfa, Agalsidase Beta, Sodium Iodide I131](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-144-320.jpg)
![C
CARDIOVASCULAR SYSTEM
101
Administration:
For oral administration, administer consistently with
meals. Take in divided doses with meals if GI upset
occurs or if taking large daily doses. If GI intolerance
occurs with single-dose therapy, use twice daily dosing.
For IV infusions >1 hour, use concentrations ≤2 mg/mL
unless a central venous catheter is used. Use only
volumetric infusion pump to prevent underdosage.
Administer through an IV line located as centrally as
possible.
For IV infusions >2 hours, administer in a non-PVC
container (e.g., glass, polyolefin). PVC tubing is
recommended for administration regardless of infusion
duration. Flush with saline prior to and following infusion
to prevent incompatibilities with heparin.
For continuous IV infusions, use an inline filter to reduce
the incidence of phlebitis. Adjust administration rate to
urgency. Give more slowly when perfusing arrhythmia is
present. Slow the infusion rate if hypotension or
bradycardia develops.
NOTE: IV administration at lower flow rates, i.e., pediatric
use, and higher concentrations than recommended may
result in leaching of plasticizers (DEHP) from IV tubing.
DEHP may adversely affect male reproductive tract
development.
Pregnancy Category: D
ATC Code: C01BD01
CLASS IV ANTIARRHYTHMICS
Rx VERAPAMIL
Oral: 80 mg tablet (as hydrochloride)
240 mg MR tablet (as hydrochloride) [for
maintenance therapy]
Inj.: 2.5 mg/mL (as hydrochloride), 2 mL ampule (IV)
A non-dihydropyridine calcium channel blocker that acts
during depolarization by inhibiting calcium ions from
entering “slow channels” or select voltage-sensitive
areas of vascular smooth muscle and myocardium.
Verapamil produces relaxation of coronary vascular
smooth muscle and coronary vasodilation, which
increases myocardial oxygen delivery in patients with
vasospastic angina and slows automaticity and
conduction of AV node.
Indications: Paroxysmal supraventricular tachycardia (PSVT)
prophylaxis; atrial fibrillation (rate control); ventricular
tachycardia
Contraindications: Severe left ventricular dysfunction;
hypotension (systolic pressure <90 mm Hg); cardiogenic
shock; sick sinus syndrome; second- or third-degree AV
block without a cardiac pacemaker; atrial flutter or
fibrillation; accessory bypass tract; any supraventricular
tachyarrhythmia conducted across an accessory
pathway (Wolff-Parkinson-White syndrome-associated
tachyarrhythmias including pre-excited atrial
fibrillation/atrial flutter, antidromic atrioventricular
reentrant tachycardia); Lown-Ganong-Levine syndrome);
concurrent use of IV beta-blocking agents; ventricular
tachycardia.
Dose:
PSVT prophylaxis, by mouth, ADULT, 240–480 mg daily in
3–4 divided doses.
Atrial fibrillation (rate control), by IV injection, ADULT, initially
0.075–0.15 mg/kg IV bolus over 2 minutes (usual dose,
5–10 mg) ; if no response, administer an additional 10
mg after 15–30 minutes; if patient responds to the initial
or repeat bolus dose, administer continuous infusion
initially at 5 mg/hour; titrate to goal heart rate;
by mouth, ADULT, as immediate-release tablet, 240-480
mg daily in 3–4 divided doses;
as MR tablet, 180–480 mg once daily.
SVT, by IV injection, ADULT, 2.5–5 mg over 2 minutes; a
second dose of 5–10 mg (approximately 0.15 mg/kg)
may be given 15–30 minutes after the initial dose if
patient tolerates, but does not respond to initial dose
(maximum total dose, 20–30 mg); CHILD 1–15 years,
0.1–0.3 mg/kg per dose over 2 minutes (maximum, 5
mg per dose); may repeat dose in 30 minutes if
inadequate response (maximum for second dose, 10
mg).
NOTE: Verapamil is NOT included in the Pediatric Advanced
Life Support (PALS) tachyarrhythmia algorithm.
Dose Adjustment:
Renal Impairment: Use with caution and monitor ECG.
Reduced renal clearance of verapamil and its
metabolite, norverapamil, in advanced renal failure.
Initiate at 100 mg daily at bedtime.
NOTE: NOT removed by hemodialysis.
Hepatic Impairment:
In patients with liver cirrhosis, administer 20% and 50%
of normal dose for oral and IV administration,
respectively. Initiate at 100 mg daily at bedtime. Monitor
ECG.
For patients with severe impairment, administer 30% of the
normal dose.
Precautions:
Conduction abnormalities (can cause first-degree AV block
or sinus bradycardia); hypotension or syncope
(symptomatic hypotension with or without syncope rarely
occur; blood pressure must be lowered at a rate
appropriate for the patient's clinical condition);
arrhythmia (severe hypotension likely to occur upon
administration); heart failure (avoid use; can exacerbate
condition); hypertrophic cardiomyopathy (use with
caution in patients with outflow tract obstruction)
Attenuated neuromuscular transmission (dose reduction
may be required); gastrointestinal effects (use MR
tablets with caution in patients with severe GI narrowing)
Hepatic impairment (monitor hemodynamics and ECG);
increased hepatic enzymes; renal impairment (monitor
hemodynamics and ECG, particularly if with concomitant
hepatic impairment)
Elderly (may experience a greater hypotensive response;
constipation may be more of a problem in the elderly;](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-145-320.jpg)
![C
CARDIOVASCULAR SYSTEM
102
may not be bioequivalent in the elderly); children (avoid
IV use in neonates and young infants due to severe
apnea, bradycardia, hypotensive reactions, and cardiac
arrest; use with caution in children as myocardial
depression and hypotension may occur)
Pregnancy (may cause adverse effects, including
bradycardia, heart block, and hypotension in fetus, and
maternal toxicity; crosses the placenta; fetal monitoring
is recommended); lactation excreted in breastmilk; not
recommended in nursing mothers)
Adverse Drug Reactions:
Common: Headache, gingival hyperplasia, constipation,
peripheral edema, hypotension, CHF, pulmonary edema,
AV block, bradycardia, flushing, fatigue, dizziness,
lethargy, pain, sleep disturbance, rash, dyspepsia,
nausea, diarrhea, myalgia, paresthesia, dyspnea, flulike
syndrome, abdominal discomfort, alopecia, angina,
arthralgia, atrioventricular dissociation, blurred vision,
bruising, cerebrovascular accident, chest pain,
claudication, confusion, diaphoresis, ECG abnormal,
equilibrium disorders, erythema multiforme, exanthema,
extrapyramidal symptoms, galactorrhea,
hyperprolactinemia, gastrointestinal distress,
gynecomastia, hyperkeratosis, impotence, insomnia,
macules, MI, muscle cramps, palpitation, psychosis,
purpura (vasculitis), shakiness, somnolence, spotty
menstruation, Stevens-Johnson syndrome, syncope,
tinnitus, urination increased, urticaria, weakness,
xerostomia
Less Common: Bronchospasm, laryngeal spasm,
depression, diaphoresis, itching, muscle fatigue,
respiratory failure, rotary nystagmus, seizure, sleepiness,
urticaria, vertigo, asystole, eosinophilia, EPS, exfoliative
dermatitis, GI obstruction, hair color change, paralytic
ileus, Parkinsonian syndrome, pulseless electrical
activity, shock, ventricular fibrillation
Drug Interactions:
NOTE: Verapamil may inhibit CYP1A2 (weak), CYP2C9
(weak), CYP2D6 (weak), CYP3A4 (moderate), and P-
glycoprotein.
Monitor closely with:
Decreases metabolism of the following drugs:
Pimecrolimus, Tacrolimus
Enhances therapeutic effect of Verapamil:
Anti-hypertensive effect: Alpha1 Blockers e.g. Alfuzosin
Anilidopiperidine Opioids e.g., Fentanyl (bradycardic);
Barbiturates e.g. (antihypertensive effect), Bretylium
(bradycardic effect; AV blockade); Brimonidine, Topical
(antihypertensive effect); Clonidine (AV blocking effect);
Magnesium Salts (antihypertensive effect), Molsidomine
(antihypertensive effect); Nicorandil (antihypertensive
effect); Other Antihypertensives (antihypertensive
effect); Other Bradycardia-causing Agents (bradycardic
effect); Other Calcium Channel Blockers
(antihypertensive effect); Pentoxifylline
(antihypertensive effect); Phosphodiesterase-5
Inhibitors (antihypertensive effect); Prostacyclin
Analogues (antihypertensive effect); Quinidine
(antihypertensive effect); Regorafenib (bradycardic
effect); Ruxolitinib (bradycardic effect); Tofacitinib
(bradycardic effect)
Enhances therapeutic effect of the following drugs:
Beta Blockers [except Levobunolol] (antihypertensive
effect); Cardiac Glycosides (AV blocking effect);
Diazoxide (antihypertensive effect); Fingolimod
(bradycardic effect); Herbs with Hypotensive Properties
(antihypertensive effect); Lacosamide (AV blocking
effect); MAO Inhibitors [except Linezolid, Tedizolid]
(antihypertensive effect)
Enhances therapeutic effect of the following drugs:
Midodrine (bradycardic effect); Neuromuscular-blocking
Agents; Nondepolarizing (neuromuscular blocking
effect); Nitroprusside (antihypertensive effect);
Salicylates (anticoagulant effect)
Increases bioavailability of the following drugs:
Fexofenadine
Increases metabolism of Verapamil:
Barbiturates
Increases risk of adverse or toxic effects of Verapamil:
Clonidine (sinus node dysfunction)
Other Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Atosiban (pulmonary edema and/or dyspnea); Beta
Blockers [except Levobunolol] (bradycardia; heart
failure); Duloxetine (orthostatic hypotensive effect);
Flecainide (impairment of myocardial contractility and
AV nodal conduction); Levodopa (orthostatic hypotensive
effect); Lithium (neurotoxic effect); Magnesium Salts;
MAO Inhibitors [except Linezolid, Tedizolid] (orthostatic
hypotensive effect)
Reduces therapeutic effect of Verapamil:
Calcium Salts; Herbs with Hypertensive Properties
(antihypertensive effect); Methylphenidate
(antihypertensive effect)
Reduces therapeutic effect of the following drugs:
Clopidogrel, Metformin
Avoid concomitant use with:
Decreases metabolism of Verapamil:
Cyclosporine, Systemic; Macrolide
Antibiotics [except Azithromycin, Fidaxomicin,
Spiramycin]; Protease Inhibitors; Antifungal Agents,
Systemic Azole Derivatives [except Fluconazole
Decreases metabolism of the following drugs:
Buspirone, Cyclosporine (Systemic)
Decreases serum concentration of Verapamil:
Carbamazepine, Dabrafenib, Mitotane, Phenytoin,
Rifamycin Derivatives, St John’s Wort
Enhances therapeutic effect of Verapamil:
Antifungal Agents, Systemic Azole Derivatives [except
Fluconazole, Isavuconazonium Sulfate] (negative
inotropic effect); Dantrolene (negative inotropic effect);
Ivabradine (QTc-prolonging effect); Telithromycin
(bradycardic and antihypertensive effects)](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-146-320.jpg)
![C
CARDIOVASCULAR SYSTEM
103
Enhances therapeutic effect of the following drugs:
Amiodarone (bradycardic effect); Ceritinib (bradycardic
effect); Dronedarone (AV-blocking and other
electrophysiologic effects); Ivabradine (bradycardic
effect)
Increases metabolism of Verapamil:
Nafcillin
Increases risk of adverse or toxic effects of Verapamil:
Dantrolene (hyperkalemic effect); Protease Inhibitors (AV
nodal blockade)
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine (hypotensive effect); Amiodarone (sinus
arrest); Antifungal Agents, Systemic Azole Derivatives
[except Fluconazole, Isavuconazonium Sulfate];
Disopyramide (potential for profound depression of
myocardial contractility); Obinutuzumab (hypotensive
effect); Oxycodone; Rituximab (hypotensive effect)
Increases serum concentration of Verapamil:
Cimetidine, Conivaptan, CYP3A4 Inducers; Fusidic Acid,
Systemic; Grapefruit Juice; Idelalisib; Mifepristone,
Protease Inhibitors; Stiripentol
Increases serum concentration of the following drugs:
Afatinib [reduce Afatinib by 10 mg if not tolerated];
Avanafil [when used concomitantly, limit Avanafil dose to
50 mg per 24-hour period]; Budesonide (Systemic);
Carbamazepine; Cilostazol [reduce Cilostazol dose to 50
mg twice daily]; Colchicine (may increase colchicine
distribution into certain tissues, e.g., brain); Dabigatran
Etexilate [active metabolites]; Dapoxetine (limit
Dapoxetine dose to 30 mg daily); Dofetilide,
Domperidone; Doxorubicin, Conventional Dronedarone,
Eletriptan, Eplerenone, Everolimus, Fentanyl,
Fosphenytoin, Halofantrine, Ivabradine, Ivacaftor,
Lovastatin [initiate Lovastatin at 10 mg daily; do not
exceed 20 mg daily]; Oxycodone [including active
metabolite, Oxymorphone]; Pazopanib, Phenytoin,
Pimozide; Ranolazine [limit Ranolazine dose to a
maximum of 500 mg twice daily]; Rivaroxaban, Silodosin,
Simeprevir; Simvastatin [if concomitant use cannot be
avoided, limit Simvastatin to 10 mg daily]; Suvorexant,
Tizanidine [if concomitant use cannot be avoided, initiate
Tizanidine at 2 mg and increase in 2–4 mg increments
based on patient response]; Tolvaptan, Topotecan,
Ulipristal, Vindesine; Zopiclone [if concomitant use
cannot be avoided, initiate Zopiclone dose at not more
than 3.75 mg]
Reduces therapeutic effect of Verapamil:
Yohimbine (antihypertensive effect)
Administration:
For IV route, administer for over 2 minutes. Administer
for over 3 minutes in older patients.
For oral route, take with food. Do NOT crush or chew MR
tablets.
Pregnancy Category: C
ATC Code: C08DA01
OTHER ANTIARRHYTHMIC AGENTS
Rx ADENOSINE
Inj.: 3 mg/mL, 2 mL vial (IV)
A class V antiarrhythmic agent that slows conduction time
through the AV node, interrupting the reentry pathways
through the AV node, thus restoring normal sinus rhythm.
Indications: Treatment of paroxysmal supraventricular
tachycardia (PSVT), including accessory bypass tracts
(Wolff-Parkinson-White syndrome); pharmacologic stress
agent in myocardial perfusion thallium201 scintigraphy.
Contraindications: Patients with second- or third-degree AV
block, sick sinus syndrome, and symptomatic
bradycardia but without a cardiac pacemaker; known or
suspected bronchoconstrictive or bronchospastic lung
disease; asthma.
Dose:
PSVT, by rapid IV push, ADULT and CHILD ≥50 kg, initially 6
mg over 1–2 seconds via a peripheral line; if not effective
within 1–2 minutes, administer 12 mg; may repeat 12
mg bolus if needed (maximum single dose, 12 mg);
follow each dose with 20 mL normal saline flush (reduce
initial dose to 3 mg if concomitantly on carbamazepine
or dipyridamole, or has a transplanted heart, or if
administered via central line); INFANT and CHILD
<50 kg, initially 0.05–0.1 mg/kg over 1–2 seconds via a
peripheral line (maximum initial dose, 6 mg); if
conversion of PSVT does not occur within 1–2 minutes,
increase dose by 0.05–0.1 mg/kg; repeat until sinus
rhythm is established or to a maximum single dose of 0.3
mg/kg or 12 mg; follow each dose with 20 mL normal
saline flush.
SVT treatment in pediatric advanced life support, by IV
injection, CHILD, initially 0.1 mg/kg (maximum initial
dose, 6 mg); if not effective within 1–2 minutes,
administer 0.2 mg/kg (maximum single dose, 12 mg);
follow each dose with ≥5 mL normal saline flush.
Pharmacologic stress testing, by continuous IV infusion,
ADULT, 140 micrograms/kg per minute for 6 minutes
using syringe or volumetric infusion pump via peripheral
line (total dose, 840 micrograms/kg); inject thallium–
201 at midpoint of infusion (3 minutes).
Dose Adjustment:
Heart Transplant Recipients:
Reduce dose.
Precautions:
Atrial fibrillation or flutter (especially in patients with PSVT
and underlying Wolff-Parkinson-White syndrome);
Cardiovascular events (e.g. cardiac arrest, fatal and
nonfatal, myocardial infarction, cerebrovascular
accident, hemorrhagic and ischemic, and sustained
ventricular tachycardia requiring resuscitation;
arrhythmia); conduction disturbances (may produce
first-, second-, or third-degree heart block; rare,
prolonged episodes of asystole);
Hypertension; Hypotension; Pulmonary artery hypertension
Respiratory disease (dyspnea, bronchoconstriction, and
respiratory compromise have occurred)](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-147-320.jpg)
![C
CARDIOVASCULAR SYSTEM
105
Reduce dose. Do not exceed 20 g every 48 hours.
Administration: For intravenous use. May be administered
via IV push, IVPB, or continuous IV infusion.
Do NOT administer at doses exceeding 20%.
For IV push, do NOT administer faster than 150
mg/minute. Administer over 1–2 minutes in patients
with persistent pulseless VT or VF with known
hypomagnesemia. Administer over 15 minutes in
patients with torsade de pointes.
If patient is severely symptomatic, or has conditions such
as preeclampsia or eclampsia, more aggressive therapy
(≤4 g over 4–5 minutes) may be required.
See Magnesium Sulfate under I.V. Solutions Additives in
Chapter 2: Blood and Blood Forming Organs for other
information.
Pregnancy Category: D
ATC Code: Not available
CARDIAC STIMULANTS, EXCLUDING
CARDIAC GLYCOSIDES
Rx DOBUTAMINE
Inj.: 50 mg/mL (concentrate, as hydrochloride), 5 mL
ampule (IV infusion)
2 mg/mL (as hydrochloride), 250 mL D5W (pre-mixed)
(IV)
A racemic mixture of dobutamine. It stimulates myocardial
beta1adrenergic receptors and some alpha1-receptors.
This results in increased contractility and heart rate, and
some peripheral vasodilation.
Indications: For management of cardiogenic or vascular
shock; inotropic agent; cardiac decompensation
Contraindications: Hypertrophic cardiomyopathy with
outflow tract obstruction (formerly known as idiopathic
hypertrophic subaortic stenosis [IHSS])
Dose:
Immediate postcardiac arrest care setting, based on Adult
Advanced Cardiovascular Life Support (ACLS) guidelines,
by IV infusion, ADULT, initially 5–10 micrograms/kg per
minute; titrate to effect.
Cardiac output maintenance and post-resuscitation
stabilization, based on Pediatric Advanced Life Support
(PALS) guidelines, by IV injection, CHILD, 2–20
micrograms/kg per minute.
Cardiac decompensation, by IV infusion, ADULT, initially
0.5–1 micrograms/kg per minute; may initiate at higher
doses, e.g., 2.5 micrograms/kg per minute, depending
on severity of decompensation with titration to desired
response (maintenance dose, 2–20 micrograms/kg per
minute; maximum dose, 40 micrograms/kg per minute).
Dose Adjustment:
Heart Failure:
Reduce doses to minimize adverse effects (maximum dose,
20 micrograms/kg per minute).
Precautions:
Arrhythmias (e.g. ventricular arrhythmias and sudden
cardiac death; may increase ventricular response rate)
Blood pressure effects (increase in blood pressure is more
common due to augmented cardiac output; may also
cause hypotension due to peripheral vasodilation)
Heart failure complications (increased risk of hospitalization
and death with prolonged use)
Tachycardia and ventricular ectopy (dose-related)
Aortic stenosis (renders therapy ineffective); electrolyte
imbalance (correct hypokalemia or hypomagnesemia
prior to use and throughout therapy to minimize the risk
of arrhythmias); hypovolemia; active myocardial
ischemia or recent myocardial infarction (can increase
myocardial oxygen demand)
Lactation (not known if excreted in breastmilk; use with
caution in nursing women)
Adverse Drug Reactions:
Common: Ventricular premature contractions, angina
pectoris, chest pain, palpitations, hypotension,
increased blood pressure, increased heart rate, localized
phlebitis, ventricular ectopy (increased), headache,
paresthesia, nausea, local inflammation, local pain (from
infiltration), leg cramps, dyspnea, fever
Rare: Skin necrosis, thrombocytopenia
Drug Interactions:
Monitor closely with:
Decreases metabolism of Dobutamine:
COMT Inhibitors e.g. Entacapone
Enhances therapeutic effect (hypertensive and tachycardic
effects) of Dobutamine:
Atomoxetine, Tedizolid
Increases risk of adverse or toxic effects of the following
drugs:
Doxofylline, Other Sympathomimetics
Reduces therapeutic effect of Dobutamine:
Calcium Salts
Avoid concomitant use with:
Enhances therapeutic effect of Dobutamine:
Linezolid (hypertensive effect)
Administration: For IV administration. Always administer via
infusion device into a large vein.
Pregnancy Category: B
ATC Code: C01CA07](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-149-320.jpg)

![C
CARDIOVASCULAR SYSTEM
107
Rx EPINEPHRINE (ADRENALINE)
Inj.: 1 mg/mL (as hydrochloride), 1 mL ampule (IV, IM, SC)
0.3 mg auto-injector (IM-preload), 0.3 mL preloaded
injection pen
A direct-acting, mixed alpha- and beta-adrenoceptor
agonist; a sympathomimetic catecholamine, which is a
potent cardiac stimulant, peripheral vasoconstrictor and
bronchodilator.
NOTE: Vasodilator at low dose (beta2-receptors).
Vasoconstrictor at high dose (alpha-receptors).
Indications: Management of anaphylactic shock; may be
used in cases of serious and fatal anaphylaxis; cardiac
arrest
Contraindications: Known hypersensitivity to epinephrine or
any of the excipients; pheochromocytoma; use in local
anesthesia of fingers, toes, ears, nose or genitalia;
shock; organic heart disease or cardiac dilatation;
closed-angle glaucoma; labor
NOTE: There are no absolute contraindications to the use of
epinephrine in life-threatening allergic reactions.
Dose:
Anaphylaxis, by IM or SC injection of 1:1,000 injection,
ADULT and ADOLESCENT, 500 micrograms (0.5 mL);
CHILD 6–12 years, 250 micrograms (0.25 mL); CHILD 6
months to 6 years, 120 micrograms (0.12 mL); INFANT
<6 months, 50 micrograms (0.05 mL); by SC injection of
1:1,000 injection, CHILD, 10 micrograms/kg (0.01
mL/kg), repeat if necessary at intervals of 20 minutes to
4 hours depending on the response of the patient and
the severity of the condition (maximum single dose, 500
micrograms).
Dose Adjustment: No information found
Precautions:
Cerebrovascular disease (increased risk of peripheral
ischemia or stroke); hypovolemia (correct before using
epinephrine); acidosis, hypercapnia, or hypoxia (may
reduce effectiveness and increase incidence of adverse
effects); heart diseases, e.g., ischemic heart disease,
heart failure, other arrhythmias (increased risk of
arrhythmias, angina, and myocardial ischemia); aortic
stenosis and hypertrophic cardiomyopathy (may
increase outflow obstruction); arrhythmias; pulmonary
hypertension (may worsen due to pulmonary
vasoconstriction).
Hyperthyroidism or diabetes mellitus (adverse reactions are
more likely to occur)
Elderly; Pregnancy (use with caution during second stage of
labor).
Adverse Drug Reactions:
Common: Anxiety, dizziness, dyspnea, fear, headache,
hyperglycemia, nausea, pallor, palpitations,
restlessness, sweating, tachycardia, tremor, vomiting,
weakness
Less Common: Angina, cerebral hemorrhage, excessive
increase in blood pressure, hypertension, peripheral
ischemia and necrosis (at infusion site), pulmonary
edema, ventricular arrhythmias
Rare: Allergic reactions
Drug Interactions:
NOTE: Alpha-adrenergic blockers antagonize
vasoconstricting and hypertensive effects of
epinephrine.
Monitor closely with:
Increases therapeutic effect of Epinephrine:
Tricyclic Antidepressants (blocks catecholamine uptake)
Increases risk of adverse or toxic effects of Epinephrine:
Drugs causing Potassium loss, [e.g., Corticosteroids,
Potassium-depleting Diuretics, Aminophylline,
Theophylline (hypokalemia)], Oxytocin (hypertension),
Tricyclic Antidepressants (arrhythmia)
Reverses therapeutic effect of Epinephrine:
Ergot Alkaloids (pressor effect)
Avoid concomitant use with:
Increases risk of adverse or toxic effects of Epinephrine:
Beta Blockers (hypertension followed by bradycardia)
Reduces therapeutic effect of Epinephrine:
Alpha Blockers (vasoconstricting and hypertensive
effects), Beta Blockers (prevents receptor activation)
Reduces therapeutic effect of Hypoglycemic Agents (loss of
blood sugar control)
Administration: Best administered by SC or IM injection into
the anterolateral aspect of the middle third of the thigh
for anaphylaxis or by IV injection for cardiac arrest or
emergency situations.
Administer by slow IV injection only in severely ill patients
when there is doubt about the adequacy of circulation
and absorption from the IM site.
Do NOT administer by intracardiac injection.
Do NOT mix with alkaline solutions. Discard after 24
hours or if solution is discolored or contains precipitate.
NOTE: If a central line is used, infusion pump is required. If
given through a peripheral line, each dose should be
followed by a flush of 20 mL of IV fluid to ensure delivery
of the drug to the central compartment.
Pregnancy Category: C
ATC Code: C01CA24](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-151-320.jpg)
![C
CARDIOVASCULAR SYSTEM
108
Rx NOREPINEPHRINE
Inj.: 1 mg/mL (as bitartrate), 2 mL and 4 mL ampule (IV
infusion)
1 mg/mL concentrate solution (as bitartrate), 10 mL
ampule (IV infusion)
2 mg/mL, solution for injection (as bitartrate), 4 mL
ampule
A direct-acting, mixed alpha- and beta-adrenoceptor agonist
that stimulates beta1-adrenergic receptors and alpha-
adrenergic receptors causing increased contractility and
heart rate, as well as peripheral vasoconstriction. This
results in an increased systemic blood pressure and
coronary blood flow. Vasoconstricting effects on alpha-
receptors are greater than the inotropic and chronotropic
effects on beta receptors.
Indications: For cardiogenic or vascular shock, persists after
adequate fluid volume replacement; severe hypotension;
first-choice vasopressor for the treatment of sepsis and
septic shock in adults
Contraindications: Hypotension from hypovolemia except as
an emergency measure to maintain coronary and
cerebral perfusion until volume could be replaced;
mesenteric or peripheral vascular thrombosis (unless
life-saving procedure); during anesthesia with
cyclopropane or halothane (risk of ventricular
arrhythmias)
Dose:
NOTE: Norepinephrine dose is stated in terms of its base
form.
Hypotension or shock, by continuous IV infusion, ADULT,
initially 8-12 micrograms/minute, titrate to desired
response (usual maintenance dose, 2–4
micrograms/minute); dosage range varies greatly
depending on clinical situation; CHILD, initially 0.05–0.1
micrograms/kg per minute; titrate to desired effect
(maximum dose, 2 micrograms/kg per minute) [NOTE: If
patient remains hypotensive despite large doses,
evaluate for occult hypovolemia, and provide fluid
resuscitation as appropriate.]
Post cardiac arrest care, by continuous IV infusion, ADULT,
initially 0.1–0.5 micrograms/kg per minute, titrate to
desired response.
Sepsis and septic shock, by continuous IV infusion, ADULT,
0.01–3 micrograms/kg per minute, titrate to desired
response.
Dose Adjustment: No information found
Precautions:
WARNING: If extravasation occurs, infiltrate the area
with 5–10 mg Phentolamine diluted in 10–15 mL
of saline using a fine hypodermic needle.
Administer Phentolamine within 12 hours after
extravasation is noted to prevent sloughing or
necrosis.
Extravasation (extravasation may cause severe ischemic
necrosis).
Pregnancy (animal reproduction studies have not been
conducted; norepinephrine is an endogenous
catecholamine and crosses the placenta);
Lactation (not known if excreted in breast milk; use with
caution when administering to nursing women).
Adverse Drug Reactions:
Common: Arrhythmias, bradycardia, peripheral ischemia,
anxiety, headache (transient), skin necrosis, dyspnea,
respiratory difficulty
Drug Interactions:
Monitor closely with:
Decreases metabolism of Norepinephrine:
COMT Inhibitors e.g., Entacapone
Enhances therapeutic effect of Norepinephrine:
MAO Inhibitors e.g., Selegeline (hypertensive effect;
tachycardia)
Enhances therapeutic effect of the following drugs:
Atomoxetine (hypertensive and tachycardic effects),
Droxidopa (hypertensive effect)
Increases risk of adverse or toxic effects of the following
drugs:
Doxofylline, Sympathomimetics
Reduces diagnostic effect of Ioflupane I123
Reduces therapeutic effect of Norepinephrine:
Alpha Blockers e.g., Phentolamine (vasodilating effect)],
Spironolactone (vasoconstricting effect)
Reduces therapeutic effect of Alpha Blockers e.g.,
Phentolamine (vasoconstricting effect)
Avoid concomitant use with:
Enhances therapeutic effect of Norepinephrine:
Beta Blockers (vasopressor effect), Ergot Derivatives
[except Ergoloid Mesylates] (hypertensive and
vasoconstricting effects), Hyaluronidase
(vasoconstricting effect), Linezolid (hypertensive effect)
[reduce initial dose], Serotonin / Norepinephrine
Reuptake Inhibitors (tachycardic and vasopressor
effects), Tricyclic Antidepressants e.g., Amitryptilline
(vasopressor effect)
Enhances therapeutic effect of Inhalational Anesthetics
e.g., Sevoflurane (arrhythmogenic effect)
Reduces therapeutic effect of Norepinephrine:
Beta Blockers e.g., Propranolol
Reduces therapeutic effect of Iobenguane I123
Administration: For IV route, administer as a continuous
infusion with the use of an infusion pump. Dilute prior to
use. Administer via a central line.
Do NOT administer alkaline solutions, i.e., sodium
bicarbonate, through the same IV line as norepinephrine.
Inactivation of norepinephrine may occur.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-152-320.jpg)
![C
CARDIOVASCULAR SYSTEM
109
EXTRAVASATION MANAGEMENT: Norepinephrine is a
vesicant. Ensure proper needle or catheter placement
prior to and during infusion. Infuse into a large vein to
prevent extravasation. Avoid infusion into leg veins. If
extravasation occurs, stop infusion immediately and
disconnect. Leave cannula or needle in place then gently
aspirate extravasated solution. Do NOT flush the line.
Remove needle or cannula and elevate extremity. Initiate
phentolamine or alternative antidote. Apply dry warm
compresses.
Pregnancy Category: C
ATC Code: C01CA03
VASODILATORS USED IN
CARDIAC DISEASES
Rx ISOSORBIDE DINITRATE (ISDN)
Oral: 10 mg and 20 mg tablet
20 mg MR tablet / capsule
Sublingual: 5 mg tablet
Inj.: 1 mg/mL, 10 mL ampule (IV)
An organic nitrate vasodilator with better stability in storage
than nitroglycerin. It is useful in patients who require
nitrates infrequently because of its slower onset of action
but longer duration. Commonly used as a PRN drug.
Indication: Prophylaxis and treatment of angina
Contraindications: Hypotension; hypovolemia; hypertrophic
obstructive cardiomyopathy; aortic stenosis; cardiac
tamponade; constrictive pericarditis; mitral stenosis;
marked anemia; head trauma; cerebral hemorrhage;
angle-closure glaucoma; GI hypermotility; malabsorption
syndrome
Dose:
Angina, acute attack, by sublingual route, ADULT, 2.5–5 mg,
repeated every 5–10 minutes as required for 3 doses
[NOTE: Inability to relieve chest pain after 3 doses may signal
acute MI, which will need immediate hospitalization. IV infusion
may be started, while awaiting transfer to the hospital, at 1
mg/hour and titrated upward to 4 mg/hour.]
Angina prophylaxis, by mouth, ADULT,
as regular release tablet, initially 5–20 mg 2–3 times
daily (maintenance dose, 10–40 mg 2–3 times daily;
maximum dose, 240 mg);
as MR tablet, 40–80 mg 1–2 times daily, space twice
daily dose 6 hours apart (maximum dose, 160 mg daily)
[NOTE: Provide nitrate-free interval daily (14 hours for regular
release and 18 hours for extended release) to avoid development
of tolerance.]
Acute angina, prevention before a precipitating activity, by
sublingual route, ADULT, 5–10 mg taken 10 minutes
before activity.
Chronic angina, prevention, by mouth, ADULT, 5-20mg
(maintenance 10–40 mg) up to 3 times daily.
Dose Adjustment:
Renal Impairment:
Consider dose reduction. Significant accumulation of the
active metabolites may occur with chronic use.
Hepatic Impairment:
Consider dose reduction. Partially metabolized by the liver.
Precautions:
Long-term therapy (may develop nitrate tolerance;
administer nitrate-free interval daily to prevent
tolerance).
Severe hepatic impairment; renal impairment;
hypothyroidism; recent history of MI; malnutrition;
hypothermia.
Pregnancy (may cross placenta; avoid medication unless
potential benefit outweighs risk).
Adverse Drug Reactions:
Common: Dizziness, fainting, flushing, hypotension
(including orthostatic hypotension), palpitations,
peripheral edema, tachycardia, throbbing headache
Less Common: Heartburn, hypoxemia, nausea, rash,
rebound angina, syncope, vomiting
Rare: Angle-closure glaucoma
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of ISDN:
Drugs which reduce blood pressure (hypotensive effects)
Reduces therapeutic effect of ISDN:
Atropine (failure to dissolve under the tongue owing to
dry mouth)
Avoid concomitant use with:
Increases risk of adverse or toxic effects of ISDN:
Phosphodiesterase Inhibitors [e.g., Sildenafil
(hypotension; MI)]
Reduces therapeutic effect of ISDN:
Antagonism of hypotensive effect: Dexamethasone,
Hydrocortisone Ibuprofen, Oral Contraceptives,
Prednisolone
Administration:
For oral administration, take on an empty stomach ½
hour before meals.
For sublingual tablets, sit or lie down before use since
the tablet may cause dizziness. Place the appropriate
dose under the tongue. Do NOT swallow. After the pain
has been relieved, the patient may spit out or swallow
what is left of the tablet to avoid adverse effects, such as
headache.
For IV infusion, mix 10 mL (equivalent to 10 mg) in 90
mL NSS.
Pregnancy Category: C
ATC Code: C01DA08](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-153-320.jpg)

![C
CARDIOVASCULAR SYSTEM
112
Contraindications: Parkinson disease; parkinsonian
symptoms; tremors, restless leg syndrome (RLS), or
other movement disorders; severe renal impairment
(CrCl <30 mL/minute)
Dose:
Adjunct in treatment of symptomatic stable angina, by
mouth, ADULT, initially 20 mg 3 times daily (maximum
dose, 20 mg 3 times daily).
NOTE: Discontinue treatment if lack of significant
antianginal response within 3 months of initiation.
Dose Adjustment:
Renal Impairment:
In patients with CrCl of 30–60 mL/minute, initial and
maximum dose is 20 mg twice daily.
In patients with CrCl <30 mL/minute, use is
contraindicated.
Hepatic Impairment:
Use in hepatic impairment has not been studied.
Precautions:
Extrapyramidal symptoms (new-onset or worsening of
parkinsonian symptoms have been reported)
Renal impairment (elimination is primarily renal; use with
caution in mild renal impairment).
Elderly (decreased renal function has been observed with
increased Trimetazidine exposure; induced gait
disturbances and/or hypotension may increase fall risk).
Lactation (not known if excreted in breastmilk;
breastfeeding is not recommended).
Adverse Drug Reactions:
Common: Dizziness, headache, pruritus, rash, urticaria,
abdominal pain, diarrhea, dyspepsia, nausea, vomiting,
weakness
Less Common: Acute generalized exanthematous
pustulosis (AGEP), agranulocytosis, angioedema,
constipation, drowsiness, flushing, gait instability,
extrasystoles, hepatitis, hypotension, insomnia,
movement disorders, palpitations, Parkinsonian
symptoms (tremor, akinesia, hypertonia), restless leg
syndrome (RLS), tachycardia, thrombocytopenia,
thrombocytopenic purpura
Drug Interactions:
Avoid concomitant use with:
Increases risk of adverse or toxic effects of Trimetazidine:
Metoclopramide (extrapyramidal symptoms)
Administration: To be taken with food.
Pregnancy Category: C
ATC Code: C01EB15
ANTIHYPERTENSIVES
AGENTS ACTING ON ARTERIOLAR
SMOOTH MUSCLE
Rx HYDRALAZINE
Oral: 25 mg and 50 mg tablet (as hydrochloride)
Inj.: 20 mg/mL (as hydrochloride), 1 mL ampule (IM, IV)
A direct vasodilator of arterioles with little effect on veins
and decreased systemic resistance.
Indication: Management of moderate to severe
hypertension
Contraindications: Mitral valve rheumatic heart disease
Dose:
Hypertension, by mouth, ADULT, initially 10 mg 4 times daily
for the first 2–4 days; increase to 25 mg 4 times daily for
the rest of the first week; further increase gradually by
10–25 mg/dose every 2–5 days to 50 mg 4 times daily
(maximum dose, 300 mg daily in divided doses); CHILD,
initially 0.75–1 mg/kg daily in 2–4 divided doses;
increase over 3–4 weeks up to 7.5 mg/kg daily in 2–4
divided doses (maximum daily dose, 200 mg daily).
Acute hypertension, by IM or IV injection, CHILD, 0.1 to 0.2
mg/kg per dose every 4–6 hours as needed (maximum
dose, 20 mg), up to 1.7–3.5 mg/kg daily in 4–6 divided
doses.
Hypertensive emergency, by IM or IV injection, ADULT, 10–
20 mg every 4–6 hours as needed. [NOTE: NOT
recommended due to unpredictable and prolonged
antihypertensive effects.]
Hypertensive emergency in pregnancy with systolic BP ≥160
mmHg or diastolic BP ≥110 mmHg, by IM or IV injection,
ADULT, initially 5 or 10 mg, may repeat dose in 20–40
minutes with 5–10 mg if blood pressure continues to
exceed thresholds (maximum total cumulative dose, 20
mg IV or 30 mg IM); after the initial dose, may initiate a
continuous infusion of 0.5–10 mg/hour instead of
intermittent dosing.
Perioperative hypertension, by IV injection, ADULT, 3 to 20
mg every 20–60 minutes as needed. [NOTE: Lower end of
dosing range is preferred in the immediate perioperative period
and in patients with renal failure. Avoid use in perioperative
hypertension, especially in patients with ischemic heart disease,
aortic dissection, or an intracranial process due to unpredictable
and prolonged antihypertensive effects.]
Dose Adjustment:
Geriatric:
Use lower initial doses within the recommended dosage
range.
Renal Impairment:
For patients with CrCl of 10–50 mL/minute, administer
every 8 hours.
For patients with CrCl <10 mL/minute, administer every 8–
16 hours in fast acetylators and every 12–24 hours in
slow acetylators.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-156-320.jpg)
![C
CARDIOVASCULAR SYSTEM
113
Precautions:
Drug-induced lupus-like syndrome (dose-related); fluid or
sodium retention (drug-induced; may require addition or
increased dose of a diuretic); peripheral neuritis
(associated with paresthesia, numbness, and tingling,
possibly due to an anti-pyridoxine effect).
Cardiovascular disease (increase in tachycardia may
increase myocardial oxygen demand); pulmonary
hypertension (may cause hypotension); renal
impairment; hepatic impairment (undergoes extensive
hepatic metabolism).
Elderly.
Pregnancy (crosses the placenta; may cause adverse
events); lactation (excreted into breastmilk; use with
caution in nursing mothers).
Adverse Drug Reactions:
Common: Angina pectoris, flushing, orthostatic
hypotension, palpitations, paradoxical hypertension,
peripheral edema, tachycardia, vascular collapse,
anxiety, chills, depression, disorientation, dizziness,
fever, headache, increased intracranial pressure,
psychotic reaction, pruritus, rash, urticaria, anorexia,
constipation, diarrhea, nausea, paralytic ileus, vomiting,
dysuria, impotence, agranulocytosis, eosinophilia,
erythrocyte count reduced, hemoglobin decreased,
hemolytic anemia, leukopenia, muscle cramps,
peripheral neuritis, rheumatoid arthritis, tremor,
weakness, conjunctivitis, lacrimation, dyspnea, nasal
congestion
Less Common: Diaphoresis, drug-induced lupus-like
syndrome, fever, arthralgia, splenomegaly,
lymphadenopathy, asthenia, myalgia, malaise, pleuritic
chest pain, edema, positive ANA and LE cells,
maculopapular facial rash, positive direct Coombs' test,
pericarditis, pericardial tamponade
Rare: Thrombocytopenia
Drug Interactions:
Monitor closely with:
Enhances antihypertensive effect of Hydralazine:
Alfuzosin, Barbiturates, Brimonidine (Topical), Diazoxide,
Herbs with hypotensive properties, Other
Antihypertensive Agents, Molsidomine, Nicorandil,
Pentoxifylline, Phosphodiesterase-5 Inhibitors,
Prostacyclin Analogues
Increases risk of adverse or toxic effects of Hydralazine:
Orthostatic hypotension: Dapoxetine, Duloxetine, Other
Antihypertensive Agents, Levodopa, MAO Inhibitors
[except Linezolid, Tedizolid]
Increases risk of adverse or toxic effects of Risperidone
(hypotensive effect)
Reduces antihypertensive effect of Hydralazine:
Methylphenidate, Nonsteroidal Anti-Inflammatory Agents
e.g., Ibuprofen
Avoid concomitant use with:
Increases risk of adverse or toxic effects of the following
drugs:
Hypotensive effect: Amifostine, Obinutuzumab,
Rituximab
TEST INTERACTION. Produces a positive direct Coombs’ Test,
interfering with blood cross-matching.
Administration: Food enhances bioavailability when taken
orally. Administer consistently with regard to meals.
For IV route, administer as a slow IV push with a
maximum rate of 5 mg/minute.
Pregnancy Category: C
ATC Code: C02DB02
Rx
NITROGLYCERIN
(GLYCERYL TRINITRATE)
Inj.: 1 mg/mL, 10 mL and 25 mL ampule (IV)
An antianginal agent that forms free radical nitric oxide,
which activates guanylate cyclase in smooth muscle,
increasing cGMP, leading to dephosphorylation of
myosin light chains and smooth muscle relaxation. It
produces a more prominent vasodilator effect on the
peripheral veins than arteries. It has blood pressure
lowering effects and also reduces cardiac oxygen
demand by decreasing preload and afterload.
Indication: For coronary artery disease
Dose:
Coronary artery disease, by IV injection, ADULT, 5
micrograms/minute, increase by 5 micrograms/minute
every 3–5 minutes until 20 micrograms/minute; if no
response at 20 micrograms/minute, may increase dose
by 10-20 micrograms/minute every 3–5 minutes
(maximum dose, 400 micrograms/minute).
See Nitroglycerin (Glyceryl Trinitrate) under Cardiac Therapy
– Vasodilators used in Cardiac Disease in Chapter 3:
Cardiovascular System for other information.
Pregnancy Category: B / C (product-specific)
ATC Code: Not available
Rx SODIUM NITROPRUSSIDE
Inj.: 50 mg powder, ampule (IV infusion)
A direct, short-acting vasodilating agent that acts directly on
the venous and arteriolar smooth muscle causing
peripheral vasodilation. It does not affect other smooth
muscle tissue, such as the uterus or duodenum, and has
no direct effect on vasomotor centers, sympathetic
nerves, or adrenergic receptors.
Indications: Management of hypertensive crisis; heart
failure and low-output syndromes; for controlled
hypotension during anesthesia
Contraindications: Inadequate cerebral circulation; use
during emergency surgery in patients near death;](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-157-320.jpg)




![C
CARDIOVASCULAR SYSTEM
118
Ophthalmic effects (can cause idiosyncratic reactions;
acute myopia and secondary angle-closure glaucoma
have been reported).
Adverse Drug Reactions:
Common: Dizziness, headache, fatigue, cough, muscle
cramps, nausea, asthenia, orthostatic effects,
impotence, diarrhea
Less Common: Syncope, chest pain, abdominal pain,
orthostatic hypotension, palpitation, tachycardia,
vomiting, dyspepsia, constipation, flatulence, dry mouth,
insomnia, nervousness, paresthesia, somnolence,
vertigo, pruritus, rash, dyspnea, gout, back pain,
arthralgia, diaphoresis, decreased libido, tinnitus,
urinary tract infection, angioedema, hypotension, cough
Administration: Take once daily in the morning. If to be
taken twice daily, take the first dose in the morning and
the second dose before 6 in the evening.
See individual monographs for Enalapril under Agents
Acting on the Renin-Angiotensin System – ACE
Inhibitors, Plain in Chapter 3: Cardiovascular System and
Hydrochlorothiazide under Diuretics – Thiazide Diuretics
in Chapter 3: Cardiovascular System for other
information.
Pregnancy Category: D
ATC Code: C09BA02; C03AX01
ANGIOTENSIN II ANTAGONISTS, PLAIN
GENERAL INFORMATION
Also known as Angiotensin Receptor Blockers (ARB), they
act by blocking the type 1 angiotensin II (AT1) receptors
on blood vessels and other tissues such as the heart,
which prevents the stimulation of vascular smooth
muscle contraction.
Precautions:
WARNING: Fetal Toxicity. Drugs acting directly on the
renin-angiotensin system can cause injury and
death to the developing fetus. When pregnancy is
detected, discontinue as soon as possible.
Peripheral vascular disease (patients may be more likely to
have renal artery stenosis)
Volume or sodium depletion (may activate the renin-
angiotensin system leading to excessive hypotension)
Aortic or mitral valve stenosis and hypertrophic
cardiomyopathy; angioedema (may occur rarely; may
involve head and neck or the intestine)
Hypotension (symptomatic hypotension may occur upon
initiation in patients who are salt- or volume-depleted);
Heart failure
Hyperkalemia; renal function deterioration (increased risk
of hyperkalemia);
Hepatic impairment
Renal artery stenosis (avoid use in patients with unstented
unilateral or bilateral renal artery stenosis).
Surgical patients (if on chronic ARB therapy, intraoperative
hypotension may occur with induction and maintenance
of general anesthesia).
Elderly (may be volume-depleted due to diuretic use and/or
blunted thirst reflex resulting in inadequate fluid intake).
Pregnancy (avoid use unless essential; may adversely affect
fetal and neonatal BP control and renal function)
Lactation (not known if excreted into breastmilk;
information is limited).
NOTE: Concomitant use of an ACE inhibitor or renin inhibitor,
e.g., Aliskiren, is associated with an increased risk of
hypotension, hyperkalemia, and renal dysfunction.
Drug Interactions:
Monitor closely with:
Decreases metabolism of ARB:
Antifungal Agents, e.g., Azole Derivatives, (Systemic),
CYP2C8 Substrates, CYP2C9 Substrates
Enhances therapeutic effect (antihypertensive effect) of
ARB:
Alfuzosin, Barbiturates e.g. Phenobarbital, Brimonidine
(Topical), Canagliflozin, Diazoxide, MAO Inhibitors
[except Linezolid, Tedizolid], Molsidomine, Nicorandil,
NSAIDs, Other Antihypertensive Agents, Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g. Sildenafil,
Prostacyclin Analogues e.g. Epoprostenol
Increases risk of adverse or toxic effects of ARB:
Antifungal Agents, e.g., Azole Derivatives, (Systemic)
Hyperkalemic effect: Canagliflozin, Heparin, Eplerenone,
Nicorandil NSAIDS (also acute renal failure), Tolvaptan,
Trimethoprim
Orthostatic hypotension: Dapoxetine, MAO Inhibitors
[except Linezolid, Tedizolid]
First ARB dose hypotension: Loop diuretics, Thiazide
diuretics
Other Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Ciprofloxacin (systemic) (arrhythmogenic effect),
Cyclosporine (systemic) (hyperkalemic effect),
Drospirenone (hyperkalemic effect), Duloxetine
(orthostatic hypotension), Levodopa (orthostatic
hypotension), Risperidone (hypotensive effect)
Reduces therapeutic effect of ARB:
Methylphenidate, Rifampicin
Avoid concomitant use with:
Increases risk of adverse or toxic effects (hyperkalemia) of
ARB:
Aliskiren (also hypotensive, and nephrotoxic effects),
Potassium Supplements, Drugs that cause Potassium
retention, e.g., Potassium-sparing Diuretics,
Spironolactone
Increases risk of adverse or toxic effects (hypotensive
effect) of the following drugs:
ACE Inhibitors e.g. Enalapril, Amifostine [withhold ARB 24
hours prior to Amifostine administration], Obinutuzumab
[withhold ARB 12 hours prior to Obinutuzumab infusion
until 1 hour after the end of the infusion], Ramipril,
Rituximab, Sodium Phosphates (also nephrotoxic effect,
specifically acute phosphate nephropathy)](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-162-320.jpg)
![C
CARDIOVASCULAR SYSTEM
119
Increases serum concentration of the following drugs:
ACE Inhibitors e.g. Enalapril, Amodiaquine, Lithium,
Ramipril [Ramiprilat]
NOTE: Dual blockade of the Renin-Angiotensin-Aldosterone
system, i.e., ARB and ACEI combination, in patients with
established heart failure, atherosclerotic disease, or
diabetes with end-organ damage is associated with
higher risk for hypotension, syncope, hyperkalemia, and
disordered renal function, including acute renal failure.
Rx IRBESARTAN
Oral: 150 mg and 300 mg tablet
An angiotensin receptor antagonist that binds to the AT1
angiotensin II receptor. It blocks the vasoconstrictor
effect of angiotensin II, as well as sodium and water
reabsorption which results in a decrease in blood
pressure.
Indication: Treatment of hypertension alone or in
combination with other antihypertensive agents
Contraindication: Concomitant use with aliskiren in patients
with diabetes mellitus
Dose:
Hypertension, by mouth, ADULT, 150 mg once daily;
patients may be titrated to 300 mg once daily; usual
dosage range, 150–300 mg daily; target dose, 300 mg
once daily.
Dose Adjustment:
Renal Impairment
Use with caution. Dose adjustment is only required if patient
is volume-depleted.
Volume Depletion:
Start dose at 75 mg.
Adverse Drug Reactions:
Common: Fatigue, diarrhea, dyspepsia, upper respiratory
infection, cough
Less Common: Abdominal distension, abnormal urination,
angina, angioedema, arrhythmia, arthritis, bronchitis,
bursitis, cardiopulmonary arrest, cerebrovascular
accident, chest pain (noncardiac), chills, congestion,
conjunctivitis, constipation, depression, dermatitis,
dyspnea, ear infection, ear pain, ecchymosis, epistaxis,
erythema, facial edema, fever, flatulence, flushing,
gastroenteritis, gout, hearing abnormality, heart failure,
hepatitis, hypertension or hypotension, hypertensive
crisis, jaundice, decreased libido, MI, muscle aches,
muscle cramps, muscle weakness, numbness,
orthostatic hypotension, paresthesia, prostate disorder,
pruritus, pulmonary congestion, renal failure, impaired
renal function, sexual dysfunction, sleep disturbance,
somnolence, thrombocytopenia, TIA, tremor, upper
extremity edema, urticaria, vision disturbance, wheezing
Rare: Hyperkalemia, anemia, rhabdomyolysis
Administration: May be administered with or without food.
See for General Information on Agents Acting on the Renin-
Angiotensin System – Angiotensin II Antagonists, Plain in
Chapter 3: Cardiovascular System for other information.
Pregnancy Category: D
ATC Code: C09CA04
Rx LOSARTAN
Oral: 50 mg and 100 mg tablet (as potassium salt)
An angiotensin II type 1 (AT1) receptor blocker whose
efficacy in hypertension is similar to that of ACE
inhibitors, but is associated with a lower incidence of
side-effects, such as dry cough and angioedema.
Indications: Treatment of hypertension; treatment of
diabetic nephropathy in patients with type 2 diabetes
mellitus (noninsulin dependent, NIDDM) and a history of
hypertension; risk reduction of stroke in patients with
HTN and left ventricular hypertrophy (LVH)
Contraindication: Concomitant use with aliskiren in patients
with diabetes mellitus
Dose:
Hypertension, by mouth, ADULT, usual starting dose, 50 mg
once daily; can be administered once or twice daily with
a total daily dose ranging from 25–100 mg (usual initial
dose in patients receiving diuretics, or those with
intravascular volume depletion: 25 mg once daily).
Nephropathy in type 2 DM and hypertension, by mouth,
ADULT, initial dose, 50 mg once daily; can be increased
to 100 mg once daily based on BP response.
Stroke reduction, HTN with LVH, by mouth, ADULT, 50 mg
once daily (maximum daily dose, 100 mg); may be in
combination with a thiazide diuretic.
Dose Adjustment:
Renal Impairment:
For severe impairment, refer patient to a specialist.
Hepatic Impairment:
For mild-to-moderate hepatic impairment, dose reduction is
warranted.
For severe impairment, refer patient to a specialist.
Adverse Drug Reactions:
Common: Dizziness, fatigue, headache, hyperkalemia,
hypoglycemia, nausea, upper respiratory tract infections,
urinary tract infections
Less Common: Abnormal liver function, angina, back pain,
decreased hemoglobin, diarrhea, dyspepsia, dyspnea,
edema, hypotension (first-dose), insomnia, malaise,
muscle cramps, myalgia, nasal congestion, palpitation,
pharyngitis, pruritus, rash, sleep disorders
Rare: Anaphylaxis, anemia, angioedema, atrial fibrillation,
cerebrovascular accidents, cough, depression, erectile
dysfunction, hepatitis, hyponatremia, pancreatitis,
purpura, renal impairment, rhabdomyolysis, syncope,
thrombocytopenia, vasculitis
Administration: May be taken with or without food.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-163-320.jpg)





![C
CARDIOVASCULAR SYSTEM
125
Bradycardia (may occur; reduce dose if heart rate drops to
<55 beats/minute); Hypotension or syncope (may occur
within the first 30 days of therapy); Angina
Heart failure (may experience a worsening of renal function;
worsening heart failure or fluid retention may occur
during upward titration).
Floppy iris syndrome (has been observed in cataract surgery
patients who were on or were previously treated with
alpha1 blockers);
Myasthenia gravis; peripheral vascular disease (may
precipitate or aggravate symptoms of arterial
insufficiency).
Bronchospastic disease (use with caution and close
monitoring)
Hepatic impairment
Psoriasis (associated with induction or exacerbation of
psoriasis)
Thyroid disease (may mask signs of hyperthyroidism; abrupt
withdrawal may exacerbate symptoms of
hyperthyroidism or precipitate thyroid storm)
Abrupt withdrawal (may cause acute tachycardia,
hypertension, and/or ischemia; severe exacerbation of
angina, ventricular arrhythmias, and myocardial
infarction have been reported; chronic betablocker
therapy should not be routinely withdrawn prior to major
surgery)
Elderly (bradycardia may be observed more frequently).
Pregnancy (increased risk of cardiovascular defects was
observed); lactation (not known if excreted in breastmilk;
may cause serious adverse reactions in the nursing
infant).
Adverse Drug Reactions:
Common: Hypotension, bradycardia, syncope, peripheral
edema, generalized edema, angina, dependent edema,
AV block, cerebrovascular accident, hypertension,
hypervolemia or hypovolemia, orthostatic hypotension,
palpitation, dizziness, fatigue, headache, depression,
fever, hypoesthesia, hypotonia, insomnia, malaise,
somnolence, vertigo, hyperglycemia,
hypercholesterolemia, hypertriglyceridemia, diabetes
mellitus, gout, hyperkalemia, hyperuricemia,
hypoglycemia, hyponatremia, weight gain, diarrhea,
nausea, vomiting, abdominal pain, melena, periodontitis,
weight loss, impotence, anemia, decreased prothrombin,
purpura, thrombocytopenia, weakness, back pain,
arthralgia, arthritis, muscle cramps, paresthesia, blurred
vision, glycosuria, hematuria, renal insufficiency, cough,
nasopharyngitis, rales, dyspnea, pulmonary edema,
rhinitis, nasal congestion, sinus congestion, injury,
allergy, flulike syndrome, sudden death
Less Common: Anaphylactoid reaction, alopecia,
angioedema, aplastic anemia, amnesia, asthma,
bronchospasm, bundle branch block, cholestatic
jaundice, concentration decreased, diaphoresis,
erythema multiforme, exfoliative dermatitis, GI
hemorrhage, decreased hearing, hypersensitivity
reaction, hypokalemia, hypokinesia, interstitial
pneumonitis, leukopenia, libido decreased, migraine,
myocardial ischemia, nervousness, neuralgia,
nightmares, pancytopenia, paresis, peripheral ischemia,
photosensitivity, pruritus, rash, respiratory alkalosis,
seizure, Stevens-Johnson syndrome, tachycardia,
tinnitus, toxic epidermal necrolysis, urinary incontinence,
urticaria, xerostomia
Drug Interactions:
Monitor closely with:
Decreases metabolism of Carvedilol:
Aminoquinolines e.g. Antimalarial drugs; Phenothiazine
Antipsychotic Agents, CYP2D6 Inhibitors (Moderate)
Decreases metabolism of Phenothiazine Antipsychotic
Agents
Enhances therapeutic effect of Carvedilol:
Bradycardic effect: Acetylcholinesterase Inhibitors e.g.,
Neostigmine, Amiodarone, Anilidopiperidine Opioids e.g.,
Fentanyl (bradycardic effect; antihypertensive effect),
Bretylium (also AV blockade), Cardiac Glycosides e.g.,
Digoxin, Dipyridamole, Disopyramide, Other Bradycardia-
causing Agents, Regorafenib, Ruxolitinib, Tofacitinib
Antihypertensive effect: Anilidopiperidine Opioids e.g.
Fentanyl, Phenothiazine Antipsychotic Agents,
Barbiturates e.g. Phenobarbital, Brimonidine (Topical),
Calcium Channel Blockers, Non-Dihydropyridine [except
Bepridil], Diazoxide, MAO Inhibitors [except Linezolid,
Tedizolid], Molsidomine, Nicardipine, Nicorandil,
Nifedipine (also inotropic effects), Other
Antihypertensive Agents , Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g. Sidenafil,
Prostacyclin Analogues e.g. Epoporestenol, Reserpine;
Propafenone (possesses independent beta blocking
activity)
Enhances therapeutic effect of the following drugs:
Bradycardic effect: Fingolimod, Ivabradine, Midodrine
Hypoglycemic effect: Insulin, Sulfonylureas e.g.,
Gliclazide
Disopyramide (negative inotropic effect)
Lacosamide (AV blocking effect)
Increases risk of adverse or toxic effects of Carvedilol:
Amiodarone (cardiac arrest), Calcium Channel Blockers,
Non-Dihydropyridine [except Bepridil] (bradycardia; signs
of heart failure), MAO Inhibitors [except Linezolid,
Tedizolid] (orthostatic hypotension), Nicardipine (may
precipitate signs of heart failure), Other Antihypertensive
Agent
Increases risk of adverse or toxic effects of the following
drugs:
Cholinergic Agonists e.g., Betanechol (cardiac
conduction abnormalities; bronchoconstriction),
Duloxetine (orthostatic hypotension), Levodopa
(orthostatic hypotension), Risperidone (hypotensive
effect)
Reduces therapeutic effect of Carvedilol:
Antihypertensive effect: Methylphenidate, Nonsteroidal
Anti-Inflammatory Agents
Avoid concomitant use with:
Decreases metabolism of Carvedilol:
CYP2D6 Inhibitors
Enhances therapeutic effect of Carvedilol:
Bradycardic effect: Dronedarone, Rivastigmine
Enhances therapeutic effect of the following drugs:](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-169-320.jpg)
![C
CARDIOVASCULAR SYSTEM
126
Alpha / Beta Agonists, Direct-Acting [except Dipivefrin]
(vasopressor effect), Ceritinib (bradycardic effect), Ergot
Derivatives e.g., Ergotamine (vasoconstricting effect)
Increases risk of adverse or toxic effects of Carvedilol:
Alpha2 Agonists e.g., Clonidine (AV-blocking and sinus
node dysfunction effects; rebound hypertension),
Floctafenine
Increases risk of adverse or toxic effects of the following
drugs:
Alpha1 Blockers e.g. Tamsulosin (orthostatic
hypotension), Amifostine (hypotensive effect), Grass
Pollen Allergen Extract / 5 Grass Extract (inhibits the
ability to effectively treat severe allergic reactions with
Epinephrine), Methacholine, Obinutuzumab
(hypotensive effect), Rituximab (hypotensive effect)
Increases serum concentration of Carvedilol:
Abiraterone Acetate, Dronedarone, Panobinostat
Increases serum concentration of the following drugs:
Afatinib [reduce Afatinib by 10 mg], Bosutinib, Colchicine
(increase distribution into certain tissues, e.g., brain),
Cyclosporine (Systemic), Dabigatran Etexilate,
Doxorubicin (Conventional), Edoxaban, Everolimus.
Pazopanib, Silodosin, Topotecan, Vincristine (Liposomal)
Reduces therapeutic effect of the following drugs:
Alpha / Beta Agonists, Direct-Acting [except Dipivefrin]
(beta-adrenoceptor-mediated effects, including anti-
anaphylactic effects of epinephrine), Beta2 Agonists
(bronchodilatory effect), Theophylline Derivatives
(bronchodilatory effect)
Administration: Administer with food to minimize the risk of
orthostatic hypotension.
Initiate only in stable patients or hospitalized patients
after volume status has been optimized and IV diuretics,
vasodilators, and inotropic agents have all been
successfully discontinued. Stabilize other heart failure
medications and minimize fluid retention prior to
initiating therapy.
Pregnancy Category: C
ATC Code: C07AG02
BETA-BLOCKING AGENTS,
NON-SELECTIVE
Rx PROPRANOLOL
Oral: 10 mg and 40 mg tablet (as hydrochloride)
A non-selective beta-adrenergic blocker that competitively
blocks responses to beta1 and beta2adrenergic
stimulation, which results in decreases in heart rate,
myocardial contractility, blood pressure, and myocardial
oxygen demand. Propranolol exhibits no intrinsic
sympathomimetic activity (ISA).
Indications: Antianginal; Management of acute coronary
syndrome; post-myocardial infarction (MI) maintenance;
antihypertensive
Dose:
Hypertension, by mouth, ADULT, 40 mg twice daily; increase
dosage every 3–7 days; usual dosage range, 40–160 mg
twice daily; usual dose, 120 to 240 mg divided in 2–3
doses daily (maximum daily dose, 640 mg);
ADOLESCENT and CHILD, initially 1–2 mg/kg daily
divided in 2–3 doses daily; titrate dose to effect
(maximum dose, 4 mg/kg daily up to 640 mg daily).
Obstructive hypertrophic cardiomyopathy, by mouth, ADULT,
20–40 mg 3–4 times daily.
Post-MI mortality reduction, by mouth, ADULT, initially 40
mg 3 times daily; usual dosage range, 180 to 240 mg
daily in 3–4 divided doses.
Stable angina, by mouth, ADULT, 80–320 mg daily in
divided doses 2–4 times daily.
Dose Adjustment:
Geriatric:
For use in hypertension, consider lower initial doses and
titrate to response.
Renal and Hepatic Impairment:
Use with caution. Renal and/or hepatic impairment
increases systemic exposure to propranolol.
Administration: To be taken on an empty stomach.
See Propranolol under Cardiac Therapy – Antiarrhythmics
(Class II Antiarrhythmics) in Chapter 3: Cardiovascular
System for other information.
Pregnancy Category: C
ATC Code: C07AA05
BETA-BLOCKING AGENTS, SELECTIVE
GENERAL INFORMATION
Selective beta-blockers (cardio-selective) exhibit a
competitive inhibitory effect on beta1adrenergic
receptors, with little or no effect on beta2receptors,
except at high doses.
Mode of Action: Competitively inhibits beta1adrenergic
receptors, preventing the action of norepinephrine and
epinephrine on these receptors. Beta1-adrenergic
receptors are primarily located in the heart. Their activity
causes a reduction in sympathetic influences, including
chronotropy (heart rate), inotropy (contractility),
dromotropy (electrical conduction), and lusitropy
(relaxation).
Contraindications: Reversible airway diseases; second- or
third-degree heart block (except in patients with
functioning artificial pacemaker); shock (cardiogenic and
hypovolemic); bradycardia (45 to 50 beats/minute); sick
sinus syndrome (except in the presence of a pacemaker);
severe hypotension; uncontrolled heart failure;
concomitant IV administration of calcium channel
blockers; pulmonary hypertension](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-170-320.jpg)
![C
CARDIOVASCULAR SYSTEM
127
Precautions:
WARNING: Do NOT withdraw beta blocker therapy
abruptly. Gradually taper over 1–2 weeks to avoid
acute tachycardia, hypertension, and/or ischemia.
Abrupt withdrawal may exacerbate angina and, in
some cases, cause myocardial infarction, ventricular
arrhythmias, and rebound hypertension. Temporary
but prompt resumption of beta-blocker therapy may
be indicated with worsening of angina or acute
coronary insufficiency.
Major surgery: Do NOT withdraw chronic beta blocker
therapy prior to major surgery.
Atrial fibrillation; Atrioventricular block (commonly produces
mild first-degree heart block; may also produce severe
first- (P-R interval ≥0.26 sec), second-, or third-degree
heart block; patients with acute myocardial infarction
have a high risk of developing heart block of varying
degrees)
Hypotension (symptomatic hypotension may occur with use)
Anaphylactic reactions (may become more sensitive to
repeated challenges; treatment of anaphylaxis, e.g.,
epinephrine, may be ineffective or even promote
undesirable effects)
Extravasation (can lead to skin necrosis and sloughing)
Hyperkalemia (associated with elevations in serum
potassium and development of hyperkalemia; monitor
serum potassium during therapy); hepatic impairment.
Bronchospastic disease (may be exacerbated)
Conduction abnormality (can cause bradycardia, including
sinus pause, heart block, severe bradycardia, and
cardiac arrest)
Diabetes (may potentiate and/or mask signs and symptoms
of hypoglycemia)
Heart failure (monitor for worsening of condition).
Myasthenia gravis
Peripheral vascular disease and Raynaud’s disease (can
precipitate or aggravate symptoms or arterial
insufficiency)
Pheochromocytoma (may aggravate hypertension; requires
adequate alpha blockade prior to use of beta-blockers)
Prinzmetal variant angina (requires concomitant alpha1-
adrenergic receptor blockage, unopposed alpha1-
adrenergic receptors mediate coronary vasoconstriction
and can worsen angina symptoms).
Psoriasis (associated with induction or exacerbation of
psoriasis)
Psychiatric disease (may cause or exacerbate CNS
depression)
Renal impairment (active metabolite is retained); thyroid
disease (may mask signs of hyperthyroidism, e.g.,
tachycardia; abrupt withdrawal may exacerbate
symptoms of hyperthyroidism and precipitate thyroid
storm; may alter thyroid function tests).
Elderly (bradycardia may be observed more frequently in
patients >65 years).
Pregnancy (crosses the placenta; may cause intrauterine
growth restriction, small placenta, fetal or neonatal
bradycardia, hypoglycemia, respiratory depression);
lactation (excreted in breast milk and detected in the
serum and urine of nursing infants; use with caution).
Adverse Drug Reactions:
Common: Alteration of glucose and lipid metabolism,
bradycardia, bronchospasm, cold extremities,
depression, diarrhea, dizziness, dyspepsia, dyspnea,
exacerbation of Raynaud’s phenomenon, fatigue,
hallucinations, first-degree heart block (P-R interval
≥0.26 seconds), heart failure, hypotension, nausea,
pruritus, second- and third-degree heart block, shortness
of breath, tiredness, syncope, vomiting, wheezing
Less Common: Acute urinary retention, anxiety, cardiogenic
shock, chest pain, claudication, confusion, constipation,
flatulence, gastric pain, headache, heartburn,
hyperhidrosis, impaired concentration, impotence,
insomnia, muscle cramps, nasal congestion,
nervousness, nightmares, palpitations, peripheral
edema, Peyronie’s disease, rash, reduced libido, sleep
disturbances, somnolence, taste disturbance, urticaria,
visual disturbances, vertigo, xerostomia
Rare: Agranulocytosis, alopecia, arthritis, blurred vision,
cardiac arrest, catatonia, emotional lability, exacerbation
of psoriasis, gangrene, hepatitis, hypersensitivity
reaction, jaundice, laryngospasm, liver function
abnormality, respiratory distress, retroperitoneal fibrosis,
thrombocytopenia, thrombocytopenic purpura, tinnitus
Drug Interactions:
Monitor closely with:
Decreases metabolism of Beta Blockers:
Aminoquinolines e.g., Antimalarial drugs
Enhances therapeutic effect of Beta Blockers:
Bradycardic effect: Acetylcholinesterase Inhibitors e.g.,
Neostigmine, Amiodarone; Anilidopiperidine Opioids e.g.,
Fentanyl (bradycardic and antihypertensive effects),
Bretylium (also AV blockade), Dipyridamole,
Disopyramide (also negative inotropic effect),
Regorafenib, Tofacitinib, Other Bradycardia-causing
Agents
Antihypertensive effect: Barbiturates e.g., Phenobarbital,
Brimonidine (Topical), Calcium Channel Blockers, Non-
Dihydropyridine [except Bepridil] e.g., Verapamil,
Diazoxide, Molsidomine, Nicorandil, Nifedipine (also
negative inotropic effect), Other Antihypertensives,
Pentoxifylline, Phosphodiesterase-5 Inhibitors e.g.,
Sildenafil, Prostacyclin Analogues e.g., Epoprostenol,
Reserpine; Propafenone (possesses independent beta
blocking activity)
Enhances therapeutic effect of the following drugs:
Bradycardic effect: Fingolimod, Ivabradine, Midodrine
Hypoglycemic effect: Insulin, Sulfonylureas e.g.,
Gliclazide
Lacosamide (AV blocking effect)
Increases risk of adverse or toxic effects of Beta Blockers:
Amiodarone (cardiac arrest), Calcium Channel Blockers,
Non-Dihydropyridine [except Bepridil] (bradycardia; signs
of heart failure), MAO Inhibitors [except Linezolid,
Tedizolid] (orthostatic hypotension), Other
Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Cardiac Glycosides (bradycardic effect); Cholinergic
Agonists (cardiac conduction abnormalities;](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-171-320.jpg)
![C
CARDIOVASCULAR SYSTEM
128
bronchoconstriction); Duloxetine (orthostatic
hypotension)
Levodopa (orthostatic hypotension); MAO Inhibitors
[except Linezolid, Tedizolid] (orthostatic hypotension)
Risperidone (hypotensive effect)
Reduces therapeutic effect of Beta Blockers:
Methylphenidate (antihypertensive effect); Nonsteroidal
Anti-Inflammatory Agents (antihypertensive effect)
Reduces therapeutic effect of the following drugs:
Beta2 Agonists (bronchodilatory effect); Theophylline
Derivatives (bronchodilatory effect)
Avoid concomitant use with:
Enhances therapeutic effect of Beta Blockers:
Alpha2 Agonists (AV blocking effect),
Bradycardic effect: Dronedarone, Rivastigmine,
Ruxolitinib
Enhances therapeutic effect of the following drugs:
Alpha / Beta Agonists, Direct-Acting [except Dipivefrin]
(vasopressor effect); Ceritinib (bradycardic effect); Ergot
Derivatives (vasoconstricting effect)
Increases risk of adverse or toxic effects of Beta Blockers:
CYP2D6 Inhibitors (heart block)
Increases risk of adverse or toxic effects of the following
drugs:
Alpha1 Blockers (orthostatic hypotension), Alpha2
Agonists (rebound hypertension; sinus node
dysfunction), Amifostine (hypotensive effect),
Floctafenine, Grass Pollen Allergen Extract / 5 Grass
Extract (inhibits the ability to effectively treat severe
allergic reactions with Epinephrine)
Methacholine, Obinutuzumab (hypotensive effect),
Rituximab (hypotensive effect)
Increases serum concentration of Beta Blockers:
CYP2D6 Inhibitors, Dronedarone
Reduces therapeutic effect of the following drugs:
Alpha / Beta Agonists, Direct-Acting [except Dipivefrin]
(beta-adrenoceptor mediated effects, including anti-
anaphylactic effects of Epinephrine)
Rx ATENOLOL
Oral: 50 mg and 100 mg tablet
A beta1-selective antagonist that competitively blocks beta1-
adrenergic stimulation, with little or no effect on beta2-
receptors except at high doses. It exhibits no intrinsic
sympathomimetic activity (ISA).
Indications: Treatment of hypertension, alone or in
combination with other agents; management of angina
pectoris; secondary prevention post-myocardial
infarction; for acute coronary syndrome
Dose:
Hypertension, by mouth, ADULT, initially 25–50 mg once
daily, may increase to 100 mg once daily after 1–2
weeks (usual dose, 100 mg once daily; target dose, 100
mg once daily); CHILD, 0.5–1 mg/kg per dose daily;
usual dosage range, 0.5 to 1.5 mg/kg daily (maximum
dose, 2 mg/kg daily for up to 100 mg daily).
Angina pectoris, by mouth, ADULT, 50 mg once daily; may
increase to 100 mg daily; some patients may require 200
mg daily.
Post-myocardial infarction, by mouth, ADULT, 100 mg daily
or 50 mg twice daily for 6–9 days post-myocardial
infarction.
Dose Adjustment:
Geriatric:
In the management of hypertension, consider lower initial
doses and titrate to response.
Renal Impairment:
If CrCl is 15–35 mL/minute per 1.73m2, maximum dose is
50 mg daily.
If CrCl is <15 mL/minute per 1.73m2, maximum dose is 25
mg daily.
For patients on hemodialysis, administer dose post-dialysis
or administer 25–50 mg supplemental dose. Atenolol is
moderately dialyzable (20% to 50%) via hemodialysis.
Administration: May be taken without regard to meals.
NOTE: When administered acutely, monitor ECG and blood
pressure.
See General Information on Beta Blocking Agents, Selective
listed above for other information.
Pregnancy Category: D
ATC Code: C07AB03
Rx BISOPROLOL
Oral: 2.5 mg and 5 mg tablet (as fumarate)
A beta1-selective antagonist that competitively blocks beta1
adrenergic stimulation, with little or no effect on beta2-
receptors at doses ≤20 mg.
Indication: Management of coronary heart failure
Dose:
Hypertension, by mouth, ADULT, initially 2.5–5 mg once
daily; may be increased to 10 mg and then up to 20 mg
once daily, if necessary; usual dose range 5–10 mg once
daily.
Heart failure, by mouth, ADULT, initially 1.25 mg once daily
(maximum dose, 10 mg once daily); increase dose
gradually and monitor for congestive signs and
symptoms of HF making every effort to achieve target
dose shown to be effective.
NOTE: Initiate only in stable patients or hospitalized patients
after volume status has been optimized and IV diuretics,
vasodilators, and inotropic agents have all been](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-172-320.jpg)
![C
CARDIOVASCULAR SYSTEM
129
successfully discontinued. Caution should be used when
initiating in patients who require inotropes during their
hospital course.
Dose Adjustment:
Renal Impairment:
For use in hypertension, if CrCl <40 mL/minute, initiate at
2.5 mg daily; increase cautiously.
Hepatic Impairment:
For patients with hepatitis or cirrhosis, initiate at 2.5 mg
daily; increase cautiously.
Administration: May be taken without regard to meals.
See General Information on Beta Blocking Agents, Selective
listed above for other information.
Pregnancy Category: C
ATC Code: C07AB07
Rx METOPROLOL
Oral: 50 mg and 100 mg tablet (as tartrate)
A beta1-adrenoceptor (cardio-selective) antagonist without
intrinsic sympathomimetic activity (ISA), which may be
advantageous in treating hypertensive patients who also
suffer from asthma, diabetes, or peripheral vascular
disease.
Indications: Management of hypertension; angina pectoris;
acute coronary syndrome; post-myocardial infarction
maintenance
Dose:
Angina, by mouth, ADULT, initially 50 mg twice daily; usual
dosage range is 50–200 mg twice daily (maximum dose,
400 mg daily); increase dose gradually at weekly
intervals to achieve desired effect.
Hypertension, by mouth, ADULT, initially 50 mg twice daily;
effective dosage range is 100–450 mg daily in 2–3
divided doses; increase dose at weekly intervals to
desired effect (maximum total daily dose, 450 mg; usual
dosage range, 50–100 mg twice daily; target dose, 100–
200 mg daily); CHILD 1–17 years, initially 1–2 mg/kg
daily (maximum dose, 6 mg/kg daily (≤200 mg daily) ;
administer in 2 divided doses.
Myocardial infarction, early treatment, by mouth, ADULT,
25–50 mg every 6–12 hours; transition over the next 2–
3 days to twice daily dosing and increase as tolerated to
a maximum daily dose of 200 mg. [NOTE: The ACCF/AHA
guidelines for the management of STEMI recommend initiation
within the first 24 hours. Do not initiate this regimen in those with
signs of heart failure, a low output state, increased risk of
cardiogenic shock, or other contraindications.]
Myocardial infarction, secondary prevention, by mouth,
ADULT, 25–100 mg twice daily; optimize dose based on
heart rate and blood pressure; continue indefinitely.
Dose Adjustment:
Geriaric:
In the management of hypertension, consider lower initial
doses and titrate to response.
Renal Impairment:
For mild-to-moderate impairment, no dose adjustment is
necessary.
For severe impairment, refer patient to a specialist.
Hepatic Impairment:
For mild-to-moderate impairment, dose reduction may be
warranted
For severe impairment, refer patient to a specialist.
Administration: To be taken with or immediately following
food.
See General Information on Beta Blocking Agents, Selective
listed above for other information.
Pregnancy Category: C
ATC Code: C07AB02
CALCIUM CHANNEL BLOCKERS
SELECTIVE CALCIUM CHANNEL BLOCKERS WITH
MAINLY VASCULAR EFFECTS
Rx AMLODIPINE
Oral: 5 mg and 10 mg tablet (as besilate / camsylate)
A long-acting dihydropyridine, calcium channel blocker,
which is useful for hypertension and coronary artery
disease.
Indication: Management of hypertension
Contraindications: unstable angina; cardiogenic shock;
hypotension; significant aortic stenosis; in instances of
MI with heart failure or poor LV function
Dose:
Hypertension, by mouth, ADULT, initially 2.5 mg once daily,
increased if necessary (maximum dose, 10 mg once
daily); CHILD, refer to a specialist.
Dose Adjustment:
Hepatic Impairment:
In patients with hepatic insufficiency, consider dose
reduction, initiating with 2.5 mg daily.
In patients with severe impairment, titrate slowly.
Precautions:
Hypotension (poor cardiac function if given with other
cardiodepressant drugs); congestive heart failure; aortic
stenosis; pre-existing abnormalities in the sinoatrial
and/or atrioventricular node (increased angina or MI can
develop after starting or increasing the dose, particularly
in patients with severe obstructive coronary artery
disease).
Hepatic impairment (half-life prolonged); Acute porphyria](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-173-320.jpg)
![C
CARDIOVASCULAR SYSTEM
130
Increased intracranial pressure; Glaucoma
Pregnancy (limited information on use in humans; risk to
fetus should be balanced against the risk of uncontrolled
maternal hypertension); lactation (presence in milk is
possible; monitor infant).
Adverse Drug Reactions:
Common: Abdominal pain, dizziness, fatigue, flushing,
gingival hyperplasia, headache, nausea, palpitation,
peripheral edema, pulmonary edema, rash, sleep
disturbances
Less Common: Arthralgia, dryness of mouth, chest pain,
constipation, dyspepsia, dyspnea, GI disturbances,
gynecomastia, hypotension, impotence, myalgia,
paresthesia, polyuria, mood changes, pruritus,
pulmonary edema, sweating, syncope, tachycardia, taste
disturbances, tinnitus, tremor, urinary disturbances,
weight changes
Rare: Agitation, alopecia, amnesia, angioedema,
arrhythmias, ataxia, cardiac failure, cholestasis,
coughing, dermatitis, erythema multiforme, gastritis,
hepatitis, hyperglycemia, myocardial infarction,
pancreatitis, Parkinsonism, parosmia, jaundice,
peripheral neuropathy, purpura, thrombocytopenia,
twitching, vasculitis, abnormal visual accommodation,
xerophthalmia
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Amlodipine:
Drugs that reduce blood pressure (enhanced
hypotensive effects)
Avoid concomitant use with:
Reduces therapeutic effect of Amlodipine:
Calcium Salts
Increases serum concentration of the following drugs,
increasing its risk of adverse or toxic effects:
Simvastatin [limit Simvastatin dose to 20 mg daily]
(myopathy)
Administration: May be taken with or without food.
Pregnancy Category: C
ATC Code: C08CA01
Rx FELODIPINE
Oral: 5 mg and 10 mg MR tablet
A dihydropyridine calcium channel blocker that inhibits
calcium ions from entering select voltage-sensitive areas
of vascular smooth muscle and myocardium during
depolarization, producing a relaxation of coronary
vascular smooth muscle and coronary vasodilation.
Indication: Management of hypertension
Dose:
Hypertension, by mouth, ADULT, 5 mg once daily; adjust
dose as needed at no less than 2-week intervals; usual
dose range, 5–10 once daily; ADOLESCENT and CHILD
≥6 years, initially 2.5 mg once daily; may increase as
needed at no less than 2-week intervals (maximum dose,
10 mg once daily).
Dose Adjustment:
Geriatric:
Consider lower initial doses and titrate at no less than 2-
week intervals to response.
Hepatic Impairment:
Initially administer 2.5 mg once daily. Monitor blood
pressure closely during titration.
Precautions:
Angina or myocardial infarction (reflex tachycardia may
occur)
Hypotension or syncope (symptomatic hypotension with or
without syncope rarely occur)
Peripheral edema (dose-dependent)
Aortic stenosis (may reduce coronary perfusion resulting in
ischemia); Heart failure (avoid use)
Hepatic impairment (may require lower starting dose)
Hypertrophic cardiomyopathy (reduction in afterload may
worsen symptoms associated with this condition)
Elderly (may experience a greater hypotensive response;
constipation may be more of a problem)
Pregnancy (untreated chronic maternal hypertension is
associated with adverse events in the fetus, infant, and
mother); lactation (not known if excreted in breastmilk)
Adverse Drug Reactions:
Common: Headache, peripheral edema, flushing,
tachycardia
Less Common: Abdominal pain, acid regurgitation, anemia,
angioedema, angina pectoris, anxiety disorders, arm
pain, arrhythmia, arthralgia, back pain, bronchitis, chest
pain, CHF, constipation, contusion, CVA, decreased
libido, depression, diarrhea, dizziness, dry mouth,
dyspnea, dysuria, epistaxis, erythema, facial edema,
flatulence, flulike illness, flushing, foot pain, gingival
hyperplasia, gynecomastia, hip pain, hypotension,
impotence, influenza, insomnia, irritability, knee pain, leg
pain, leukocytoclastic vasculitis, MI, muscle cramps,
myalgia, nausea, nervousness, palpitation, paresthesia,
pharyngitis, polyuria, premature beats, respiratory
infection, sinusitis, somnolence, syncope, urinary
frequency, urinary urgency, urticaria, visual
disturbances, vomiting
NOTE: Doses >10 mg daily are associated with greater
antihypertensive effects but also with a large increase in
the incidence of peripheral edema and other
vasodilatory adverse effects.
Drug Interactions:
Monitor closely with:
Decreases metabolism of Felodipine:
Cyclosporine (Systemic), CYP2C8 Substrates, CYP3A4
Inhibitors (Moderate)
Enhances antihypertensive effect of Felodipine:
Alfuzosin, Alpha1 Blockers, Barbiturates e.g.,
Phenobarbital, Brimonidine (Topical); Non-
Dihydropyridine Calcium Channel Blockers e.g.,
Verapamil, Diazoxide, Magnesium Salts, MAO Inhibitors
[except Linezolid, Tedizolid], Molsidomine, Nicorandil,](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-174-320.jpg)
![C
CARDIOVASCULAR SYSTEM
131
Other Antihypertensive Agents; Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g., Sildenafil,
Prostacyclin Analogues e.g., Epoprostenol
Enhances therapeutic effect of the following drugs:
Nondepolarizing neuromuscular-blocking Agents e.g.,
Vecuronium (neuromuscular-blocking effect),
Nitroprusside (hypotensive effect)
Increases absorption of Felodipine:
Ethyl Alcohol
Increases metabolism of Felodipine:
Barbiturates e.g., Phenobarbital
Increases risk of adverse or toxic effects of Felodipine:
Dapoxetine (orthostatic hypotension), MAO Inhibitors
[except Linezolid, Tedizolid] (orthostatic hypotension),
Other Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Atosiban (pulmonary edema and/or dyspnea),
Duloxetine (orthostatic hypotension), Levodopa
(orthostatic hypotension), Magnesium Salts, Risperidone
(hypotensive effect)
Reduces antihypertensive effect of Felodipine:
Calcium Salts, Methylphenidate
Reduces therapeutic effect of Clopidogrel
Avoid concomitant use with:
Decreases metabolism of Felodipine:
Antifungal Agents, Azole Derivatives, (Systemic) [except
Fluconazole, Isavuconazonium Sulfate], CYP3A4
Inhibitors (Strong), Macrolide Antibiotics [except
Azithromycin, Fidaxomicin, Spiramycin]
Decreases serum concentration of Felodipine:
Dabrafenib, Mitotane, Phenytoin, Rifamycin Derivatives
Increases metabolism of Felodipine:
Carbamazepine, CYP3A4 Inducers (Strong), Nafcillin
Increases risk of adverse or toxic effects of Felodipine:
Antifungal Agents, Azole Derivatives, Systemic [except
Fluconazole] (negative inotropic effects), Mifepristone,
Stiripentol
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine (hypotensive effect), Obinutuzumab [withhold
Felodipine 12 hours prior to Obinutuzumab infusion until
1 hour after the end of the infusion] (hypotensive effect),
Phenytoin, Rituximab (hypotensive effect)
Increases serum concentration of Felodipine:
Cimetidine, Fosphenytoin, Fusidic Acid (Systemic),
Grapefruit Juice, Idelalisib, Itraconazole, Ketoconazole
(Systemic), Mifepristone, Stiripentol
Increases serum concentration of the following drugs:
Amodiaquine, Phenytoin
Reduces therapeutic effect of Felodipine:
Phenytoin
Administration: May be administered without food or with a
small meal that is low in fat and carbohydrates. Avoid
grapefruit juice during therapy.
Swallow tablet whole. Do NOT divide, crush, or chew.
NOTE: Felodipine peak plasma concentrations are
increased up to two-fold when taken after a meal high in
fat or carbohydrates. Grapefruit juice similarly increases
felodipine Cmax by two-fold. Increased therapeutic and
vasodilator side effects, including severe hypotension
and myocardial ischemia, may occur.
Pregnancy Category: C
ATC Code: C08CA02
Rx NICARDIPINE
Inj.: 1 mg/mL (as hydrochloride), 2 mL and 10 mL ampule
(IV)
A calcium channel blocker that inhibits calcium ions from
entering select voltage-sensitive areas of vascular
smooth muscle and myocardium. It produces a
relaxation of coronary vascular smooth muscle and
coronary vasodilation, thus increasing myocardial oxygen
delivery in patients with vasospastic angina.
Indication: Management of acute hypertension
Contraindications: Advanced aortic stenosis
Dose:
Acute hypertension, by IV infusion, ADULT, 5 mg/ hour
initially, may increase by 2.5 mg/hour every 5 minutes
for rapid titration, to every 15 minutes for gradual
titration (maximum dose, 15 mg/hour); in rapidly titrated
patients, consider reduction to 3 mg/hour after response
is achieved
Dose Adjustment:
Geriatric:
Initiate at the low end of the dosage range. Monitor closely.
Renal and Hepatic Impairment:
Dose adjustment may be necessary. Titrate slowly with
careful monitoring. Consider lower starting dose and
closely monitor response.
Precautions:
WARNING: Significant differences exist between oral
and IV dosing. Use caution when converting from
one route of administration to another.
Angina, myocardial infarction (increased frequency,
duration, or severity of angina and/or MI has occurred
with initiation or dosage titration; reflex tachycardia may
occur);
Hypotension; Syncope (rarely occurs); Peripheral edema
(dose-dependent); Tachycardia (may occur).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-175-320.jpg)
![C
CARDIOVASCULAR SYSTEM
132
Aortic stenosis (may reduce coronary perfusion resulting in
ischemia)
Heart failure (may worsen symptoms of HF due to mild
negative inotropic effects of nicardipine, particularly with
concomitant beta blockade)
Hypertrophic cardiomyopathy with outflow tract obstruction
(reduction in afterload may worsen symptoms
associated with this condition)
Hepatic impairment; Renal impairment
Abrupt withdrawal may cause rebound angina in patients
with CAD
Elderly (constipation may be more of a problem; may
experience greater hypotensive response)
Pregnancy (adverse events have been observed in some
animal reproduction studies; crosses the placenta;
changes in fetal heart rate, neonatal hypotension and
neonatal acidosis have been observed following
maternal use); lactation (minimally excreted in
breastmilk; breastfeeding is not recommended).
Adverse Drug Reactions:
Common: Flushing, pedal edema, exacerbation of angina
pectoris, hypotension, palpitations, tachycardia, chest
pain, extrasystoles, hemopericardium, supraventricular
tachycardia, hypertension, edema, headache, dizziness,
hypoesthesia, intracranial hemorrhage, pain,
somnolence, diaphoresis, skin rash, hypokalemia,
nausea, vomiting, dyspepsia, abdominal pain,
xerostomia, hematuria, injection site reaction, pain at
injection site, weakness, myalgia, paresthesia
Less Common: Abnormal dreams, abnormal vision, angina
pectoris, anxiety, atrial fibrillation, atrioventricular block,
arthralgia, atypical chest pain, blurred vision, cerebral
ischemia, confusion, conjunctivitis, constipation, deep
vein thrombophlebitis, depression, ST segment
depression, dyspnea, ear disease, fever, gingival
hyperplasia, heart block, hot flash, hyperkinesia,
hypersensitivity reaction, hypophosphatemia,
hypertonia, impotence, infection, insomnia, inversion T
wave on ECG, malaise, myocardial infarction, neck pain,
nervousness, nocturia, orthostatic hypotension,
parotitis, pericarditis, peripheral vascular disease,
respiratory tract disease, rhinitis, sinus node
dysfunction, sinusitis, sore throat, sustained tachycardia,
syncope, thrombocytopenia, tinnitus, tremor, urinary
frequency, ventricular extrasystoles, ventricular
tachycardia, vertigo, vomiting
Drug Interactions:
Monitor closely with:
Decreases metabolism of Nicardipine:
Cyclosporine (Systemic), CYP2C19 Substrates, CYP2D6
Substrates
Enhances therapeutic effects of Nicardipine:
Antihypertensive effect: Alpha1 Blockers e.g. Alfuzosin,
Barbiturates e.g. Phenobarbital, Brimonidine (Topical),
Non-Dihydropyridine Calcium Channel Blockers,
Diazoxide, Magnesium Salts, Molsidomine, Nicorandil,
Pentoxifylline, Phosphodiesterase-5 Inhibitors e.g.
Sildenafil, Prostacyclin Analogues e.g. Epoporestenol,
Other Antihypertensive Agents
Moderate Risk QTc-prolonging Agents, Indeterminate
Risk and Risk Modifying (QTc-prolonging agents)
Enhances therapeutic effect of the following drugs:
Aripiprazole, Carvedilol (hypotensive effect),
Nondepolarizing Neuromuscular-blocking Agents e.g.
Pancuronium (neuromuscular-blocking effect),
Nitroprusside (hypotensive effect)
Increases metabolism of Nicardipine:
Barbiturates e.g. Phenobarbital
Increases risk of adverse or toxic effects of Nicardipine:
Dapoxetine (orthostatic hypotension), MAO Inhibitors
[except Linezolid, Tedizolid] (orthostatic hypotension),
Other Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Atosiban (pulmonary edema and/or dyspnea), Carvedilol
(may precipitate signs of heart failure), Duloxetine
(orthostatic hypotension), Levodopa (orthostatic
hypotension), Magnesium Salts, Risperidone
(hypotensive effect)
Reduces therapeutic effect of Nicardipine:
Barbiturates e.g Phenobarbital, Calcium Salts,
Methylphenidate
Reduces therapeutic effect of the following drugs:
Codeine (prevents metabolic conversion to its active
metabolite, morphine); Tramadol (prevents metabolic
conversion to its active metabolite)
Avoid concomitant use with:
Decreases metabolism of Nicardipine:
Antifungal Agents, Azole Derivatives, Systemic [except
Fluconazole], CYP2C9 Substrates, CYP3A4 Inhibitors;
Macrolide Antibiotics [except Azithromycin, Spiramycin]
Decreases serum concentration of Nicardipine:
Dabrafenib, Efavirenz, Mitotane, Phenytoin, Rifamycin
Derivatives, Siltuximab
Decreases serum concentration of the following drugs:
Clopidogrel, Tamoxifen
Enhances therapeutic effect of the following drugs:
Highest Risk QTc-prolonging Agents, Indeterminate Risk
and Risk Modifying (QTc-prolonging effect)
Enhances therapeutic effect of Nicardipine:
Mifepristone (QTc-prolonging effect)
Increases metabolism of Nicardipine:
Carbamazepine, CYP3A4 Inducers, Nafcillin
Increases risk of adverse or toxic effects of Nicardipine:
Azole Antifungal Agents (Systemic) [except Fluconazole,]
(negative inotropic effects), Grapefruit Juice,
Mifepristone, Stiripentol
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine [withhold Nicardipine 24 hours prior to
Amifostine administration] (hypotensive effect),
Citalopram (serotonin syndrome; QT prolongation),
Fosphenytoin, Highest Risk QTc-prolonging Agents,
Indeterminate Risk and Risk Modifying (alterations of
cardiac rhythm), Obinutuzumab [withhold Nicardipine 12](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-176-320.jpg)
![C
CARDIOVASCULAR SYSTEM
133
hours prior to Obinutuzumab infusion until 1 hour after
the end of the infusion] (hypotensive effect), Phenytoin,
Rituximab (hypotensive effect)
Increases serum concentration of Nicardipine:
Fosphenytoin, Fusidic Acid (Systemic), Grapefruit Juice,
Idelalisib, Mifepristone, Simeprevir, Stiripentol
Increases serum concentration of the following drugs:
Afatinib [reduce Afatinib dose by 10mg], Bosutinib,
Cilostazol [reduce Cilostazol dose to 50 mg twice daily],
Citalopram [limit Citalopram dose to a maximum of 20
mg daily], Colchicine (increases distribution into certain
tissues, e.g., brain), Dabigatran Etexilate, Diclofenac
(Systemic), Doxorubicin (Conventional), Edoxaban,
Eliglustat [reduce Eliglustat dose to 84 mg daily],
Everolimus, Lacosamide, Lomitapide [limit maximum
Lomitapide dose to 30 mg daily], Metoprolol, Pazopanib,
Phenytoin, Pimozide, Silodosin, Thioridazine, Topotecan,
Vincristine (Liposomal)
Reduces therapeutic effect of Nicardipine:
Phenytoin
Reduces therapeutic effect of the following drugs:
Clopidogrel, Fosphenytoin
Administration: Administer by slow continuous IV infusion
via a central line or through a large peripheral vein. Avoid
use of small peripheral veins to minimize infusion site
reactions.
Do NOT combine or run in the same line as other
medications.
Monitor infusion site closely to prevent extravasation.
Peripheral venous irritation may be minimized by
changing the site of infusion every 12 hours.
Evaluate cardiac status and blood pressure and monitor
for rash, hypotension, bradycardia, confusion, and
nausea when starting, adjusting dose, or discontinuing.
NOTE: Parenteral administration is indicated only for short-term use.
Teach patient orthostatic precautions.
Pregnancy Category: C
ATC Code: C08CA04
Rx NIFEDIPINE
Oral: 10 mg capsule
30 mg MR tablet
A calcium channel blocker that inhibits calcium ion from
entering select voltage-sensitive areas of vascular
smooth muscle and myocardium during depolarization.
It produces coronary vasodilation and reduces peripheral
vascular resistance and ultimately, arterial blood
pressure.
Indication: Treatment of hypertension
Contraindications: Concomitant use with strong CYP3A4
inducers (e.g., rifampin); cardiogenic shock; STEMI;
Heart failure
Dose:
Hypertension, by mouth, ADULT, initially 30–60 mg once
daily, titrate to 30–90 mg daily (maximum, 90–120 mg
daily).
NOTE: Adjust dose at 7– to 14–day intervals to allow for
adequate assessment of new dose. If clinically indicated,
titration may be done more rapidly with appropriate
monitoring.
Use same total daily dose when switching from
immediate-release
to sustained-release formulation.
Dose Adjustment:
Geriatric:
Consider lower initial doses and titrate to response. Half-life
is extended in elderly patients (6.7 hours) as compared
to younger subjects (3.8 hours).
Hepatic Impairment:
Use with caution. Clearance is reduced in cirrhotic patients,
which may lead to increased systemic exposure. Monitor
closely for adverse effects or toxicity and consider dose
adjustments.
Precautions:
WARNING: Use with extreme caution due to rapid and
prolonged fall in blood pressure.
Use is restricted for acute hypertensive emergencies in
patients less than 18 years old.
Abrupt withdrawal (may cause rebound angina in patients
with CAD).
Angina or MI (increased angina and/or MI have occurred;
reflex tachycardia may occur resulting in angina and/or
MI in patients with obstructive coronary disease)
Hypotension or syncope (rarely occurs; blood pressure must
be lowered at a rate appropriate for the patient's clinical
condition; death, cerebrovascular ischemia, syncope,
stroke, acute myocardial infarction, and fetal distress,
have been reported)
Peripheral edema (most common side effect).
Aortic stenosis (may reduce coronary perfusion resulting in
myocardial ischemia); Heart failure (avoid use)
Hypertrophic cardiomyopathy with outflow tract obstruction
(reduction in afterload may worsen symptoms
associated with this condition).
Gastrointestinal strictures (alterations in GI anatomy, e.g.,
severe GI narrowing, history of GI cancer, obstruction,
bowel resection, gastric bypass, vertical banded
gastroplasty, and underlying hypomotility disorders have
led to bezoar formation with extended release forms);
hepatic impairment.
Immediate-release formulations should not be used to
manage primary hypertension (adequate studies have
not been conducted)
May contain lactose (do not administer in patients with
galactose intolerance, Lapp lactase deficiency, or
glucose-galactose malabsorption syndromes).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-177-320.jpg)
![C
CARDIOVASCULAR SYSTEM
134
Surgery (cardiopulmonary bypass, intraoperative blood loss
or vasodilating anesthesia may result in severe
hypotension and/or increased fluid requirements;
consider withdrawing nifedipine >36 hours before
surgery).
Elderly (immediate-release tablets may cause hypotension
and risk of precipitating myocardial ischemia; may
experience a greater hypotensive response; constipation
may be more of a problem).
Pregnancy (crosses the placenta and small amounts can be
detected in the urine of newborn infants; an increase in
perinatal asphyxia, cesarean delivery, prematurity, and
intrauterine growth retardation have been reported);
lactation (excreted in breast milk; breastfeeding is not
recommended).
Adverse Drug Reactions:
Common: Flushing, peripheral edema (dose-related),
palpitation, transient hypotension (dose-related),
coronary heart failure, lightheadedness, dizziness,
giddiness, nervousness, headache, mood changes,
fatigue, shakiness, jitteriness, sleep disturbances,
difficulties in balance, fever, chills, dermatitis, pruritus,
urticaria, sexual difficulties, nausea, heartburn,
constipation, diarrhea, cramps, flatulence, muscle
cramps or tremor, weakness, inflammation, joint
stiffness, gingival hyperplasia, blurred vision, coughing,
wheezing, nasal congestion, sore throat, chest
congestion, dyspnea, diaphoresis
Less Common: Agranulocytosis, allergic hepatitis, alopecia,
anemia, aplastic anemia, angina, angioedema,
arrhythmia, arthritis with positive ANA, bezoars, cerebral
ischemia, depression, dysosmia, epistaxis, EPS, erectile
dysfunction, erythromelalgia, exanthematous pustulosis,
erythema multiforme, exfoliative dermatitis, facial
edema, gastroesophageal reflux, gastrointestinal
obstruction, gastrointestinal ulceration, gynecomastia,
hematuria, ischemia, leukopenia, lip cancer, memory
dysfunction, migraine, myalgia, myoclonus, nocturia,
paranoid syndrome, parotitis, periorbital edema,
photosensitivity, polyuria, purpura, Stevens-Johnson
syndrome, syncope, tachycardia, taste perversion,
thrombocytopenia, tinnitus, toxic epidermal necrolysis,
transient blindness, ventricular arrhythm
Drug Interactions:
Monitor closely with:
Decreases metabolism of Nifedipine:
Cyclosporine (Systemic)
Enhances antihypertensive effect of Nifedipine:
Alpha1 Blockers e.g. Alfuzosin, Barbiturates e.g.
Phenobarbital, Brimonidine (Topical), Non-
dihydropyridine Calcium Channel Blockers, Diazoxide,
Magnesium Salts, Molsidomine, Nicorandil, Other
Antihypertensive Agents, Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g. Sildenafil,
Prostacyclin Analogues e.g. Epoprostenol
Enhances therapeutic effect of the following drugs:
Aripiprazole, Beta Blockers (hypotensive effect; negative
inotropic effect), Nondepolarizing Neuromuscular-
blocking Agents e.g. Pancuronium (neuromuscular-
blocking effect), Nitroprusside (hypotensive effect)
Increases metabolism of Nifedipine:
Barbiturates e.g. Phenobarbital
Increases risk of adverse or toxic effects of Nifedipine:
Dapoxetine (orthostatic hypotension), MAO Inhibitors
[except Linezolid, Tedizolid] (orthostatic hypotension),
Other Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Atosiban (pulmonary edema and/or dyspnea),
Duloxetine (orthostatic hypotension), Fluoxetine,
Levodopa (orthostatic hypotension), Magnesium Salts,
Risperidone (hypotensive effect)
Reduces therapeutic effect of Nifedipine:
Calcium Salts, Melatonin (antihypertensive effect),
Methylphenidate (antihypertensive effect)
Reduces therapeutic effect of Clopidogrel
Avoid concomitant use with:
Decreases metabolism of Nifedipine:
CYP3A4 Inhibitors, Macrolide Antibiotics [except
Azithromycin, Spiramycin]
Decreases serum concentration of Nifedipine:
Dabrafenib, Phenytoin
Enhances therapeutic effect of Nifedipine:
Cimetidine, Grapefruit Juice
Enhances therapeutic effect of Tizanidine
Increases metabolism of Nifedipine:
CYP3A4 Inducers (Strong), Nafcillin
Increases risk of adverse or toxic effects of Nifedipine:
Azole Derivatives (Systemic) [except Fluconazole,
Isavuconazonium Sulfate], Grapefruit Juice (severe
hypotension; myocardial ischemia), Mifepristone,
Stiripentol
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine [withhold Nifedipine 24 hours prior to
Amifostine administration] (hypotensive effect),
Obinutuzumab [withhold Nifedipine 12 hours prior to
Obinutuzumab infusion until 1 hour after the end of the
infusion] (hypotensive effect), Rituximab (hypotensive
effect), Tizanidine
Increases serum concentration of Nifedipine:
Cimetidine, Conivaptan, Fusidic Acid (Systemic),
Idelalisib, Mifepristone, Stiripentol
Increases serum concentration of the following drugs:
Phenytoin, Tizanidine [initiate Tizanidine at 2 mg and
increase in 2–4 mg increments based on patient
response]
Reduces therapeutic effect of Nifedipine:
Dabrafenib
Administration: May be taken with or without food. Capsules
are rapidly absorbed orally if administered without food
but may result in vasodilator side effects. If flushing is](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-178-320.jpg)
![C
CARDIOVASCULAR SYSTEM
135
problematic, administer low-fat meals to decrease
flushing.
Swallow tablets whole. Do NOT crush, split, or chew.
Teach patient orthostatic precautions.
NOTE: For Adalat CC, Afeditab CR, Nifediac CC, administer
on an empty stomach (as per manufacturer labelling).
Other extended-release products may not have this
recommendation; consult product labeling.
Nifedipine serum levels may be decreased if taken with
food. Food may decrease the rate but not the extent of
absorption of Procardia XL®.
Pregnancy Category: C
ATC Code: C08CA05
Rx NIMODIPINE
Oral: 30 mg tablet
A calcium channel blocker that inhibits calcium ion from
entering select voltage-sensitive areas of vascular
smooth muscle and myocardium during depolarization.
Nimodipine has a greater effect on cerebral arterials
than other arterials due to the drug's increased
lipophilicity and cerebral distribution.
Indication: Prophylaxis and treatment of ischemic
neurologic deficits caused by cerebral vasospasms
following subarachnoid hemorrhage of aneurysmal origin
Contraindications: Concomitant use with phenobarbital,
phenytoin, carbamazepine, or rifampin; concomitant use
with strong CYP3A4 inhibitors (e.g., clarithromycin,
telithromycin, delaviridine, indinavir, nelfinavir, ritonavir,
saquinavir, ketoconazole, itraconazole, voriconazole,
and nefazodone)
Dose:
Subarachnoid hemorrhage: oral: 60 mg every 4 hours for 21
consecutive days (maximum total duration of therapy), or
until transitioning IV therapy is needed.
Dose Adjustment:
Renal Impairment:
Nimodipine undergoes minimal renal elimination. Dose
adjustment may not be necessary.
Not removed by hemodialysis or peritoneal dialysis.
Supplemental dose is not necessary.
Hepatic Impairment:
Use with caution in patients with cirrhosis. Reduce dose to
30 mg every 4 hours.
Precautions:
Angina or MI (increased angina and/or MI have occurred
with initiation or dosage titration CCBs; reflex
tachycardia may occur resulting in angina and/or MI in
patients with obstructive coronary disease)
Hypotension or syncope (symptomatic hypotension with or
without syncope can occur; monitor blood pressure
closely during treatment); Peripheral edema.
Gastrointestinal events (intestinal pseudo-obstruction and
ileus)
Hepatic impairment (monitor blood pressure and heart rate
closely)
Hypertrophic cardiomyopathy with outflow tract obstruction
Elderly (may experience a greater hypotensive response;
constipation may be more of a problem)
Pregnancy (crosses the placenta; adverse events have been
observed in animal reproduction studies); lactation
(excreted into breastmilk; breast-feeding is not
recommended).
Adverse Drug Reactions:
Common: Decreased blood pressure, bradycardia,
headache, nausea
Less Common: Anemia, decreased platelet count,
diaphoresis, edema, disseminated intravascular
coagulation, dizziness, flushing, gastrointestinal
hemorrhage, GI pseudo-obstruction, hematoma,
hepatitis, hypertension, intestinal obstruction, jaundice,
muscle cramps, palpitations, pruritus, rebound
vasospasm, thrombocytopenia, vomiting, wheezing
Drug Interactions:
Monitor closely with:
Decreases metabolism of Nimodipine:
Cyclosporine (Systemic)
Enhances antihypertensive effect of Nimodipine:
Alpha1 Blockers e.g. Alfuzosin, Barbiturates e.g.
Phenobarbital, Brimonidine (Topical), Non-
Dihydropyridine Calcium Channel Blockers e.g.
Verapamil, Diazoxide, Magnesium Salts, MAO Inhibitors
[except Linezolid, Tedizolid], Molsidomine, Nicorandil,
Other Antihypertensive Agents, Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g. Sildenafil,
Prostacyclin Analogues e.g. Epoprostenol
Enhances therapeutic effect of the following drugs:
Nondepolarizing Neuromuscular-blocking Agents e.g.
Pancuronium (neuromuscular-blocking effect),
Nitroprusside (hypotensive effect)
Increases metabolism of Nimodipine:
Barbiturates e.g. Phenobarbital, Nafcillin
Increases risk of adverse or toxic effects of Nimodipine:
Dapoxetine (orthostatic hypotension)
MAO Inhibitors [except Linezolid, Tedizolid] (orthostatic
hypotension)
Other Antihypertensive Agents
Increases risk of adverse or toxic effects of the following
drugs:
Atosiban (pulmonary edema and/or dyspnea),
Duloxetine (orthostatic hypotension), Levodopa
(orthostatic hypotension), Magnesium Salts, Risperidone
(hypotensive effect)
Reduces antihypertensive effect of Nimodipine:
Methylphenidate
Reduces therapeutic effect of Clopidogrel](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-179-320.jpg)
![C
CARDIOVASCULAR SYSTEM
136
Avoid concomitant use with:
Decreases metabolism of Nimodipine:
Macrolide Antibiotics [except Azithromycin, Fidaxomicin,
Spiramycin]
Decreases serum concentration of Nimodipine:
CYP3A4 Inducers (Strong), Dabrafenib
Enhances therapeutic effect of Nimodipine:
Cimetidine
Increases risk of adverse or toxic effects of Nimodipine:
Mifepristone, Stiripentol
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine [withhold Nimodipine 24 hours prior to
Amifostine administration] (hypotensive effect);
Obinutuzumab [withhold Nifedipine 12 hours prior to
Obinutuzumab infusion until 1 hour after the end of the
infusion] (hypotensive effect); Rituximab (hypotensive
effect)
Increases serum concentration of Nimodipine:
Cimetidine, Conivaptan, CYP3A4 Inhibitors (Strong),
Fusidic Acid (Systemic), Idelalisib, Mifepristone,
Stiripentol
Reduces therapeutic effect of Nimodipine:
Dabrafenib
Administration: Administer consistently with or without
meals.
Swallow tablet whole with an adequate amount of fluid,
e.g., glass of water. Do NOT crush tablet.
Avoid alkaline mixtures for 2 hours before or after
administration. Patient should not be lying down during
administration.
Do NOT administer parenterally. Life-threatening
adverse events have occurred when contents of oral
formulation were administered parenterally.
Pregnancy Category: C
ATC Code: C08CA06
SELECTIVE CALCIUM CHANNEL
BLOCKERS WITH DIRECT
CARDIAC EFFECTS
GENERAL INFORMATION
Selective calcium-channel blockers (CCBs) exhibit an
inhibitory effect on L-type calcium channels. It is used for
the treatment of hypertension, angina, and arrhythmias.
Mode of Action: Binds to L-type calcium channels located on
the vascular smooth muscle, cardiac myocytes, and
cardiac nodal tissue, blocking entry of calcium into the
cell. This causes vascular smooth muscle relaxation,
decreased myocardial force generation, decreased heart
rate, and decreased conduction velocity within the heart.
Precautions:
WARNING: All CCBs have some degree of negative
inotropic effect and may, in excessive doses or in
combination with other drugs, produce myocardial
depression especially after MI.
Abrupt withdrawal and long-term use (has been associated
with severe angina).
Conduction abnormalities (may worsen first-degree AV
block and exacerbate bradycardia); arrhythmia (severe
hypotension likely to occur upon administration); heart
failure (can exacerbate condition); impaired left
ventricular function; hypotension or syncope
(symptomatic hypotension with or without syncope rarely
occur);
Hypertrophic cardiomyopathy [HCM] with outflow tract
obstruction.
Hepatic and renal impairment (in severe impairment,
monitor hemodynamics and ECG); Increased hepatic
enzymes (rarely observed)
Diabetes mellitus (affects insulin secretion and its
peripheral action).
Attenuated neuromuscular transmission (decreased
neuromuscular transmission has been reported).
Patients taking beta-blockers or digitalis (at risk of AV block,
bradycardia, asystole, or sinus arrest);
Patients at risk to develop intestinal obstruction (diltiazem
has an inhibitory effect on intestinal motility; may be
associated with mood changes).
Children (severe apnea, bradycardia, hypotensive
reactions, and cardiac arrest may occur).
Elderly (greater hypotensive response; constipation may be
more of a problem)
Pregnancy (crosses the placenta; adverse events were
observed in some animal reproduction studies); lactation
(excreted into breast milk; not recommended).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-180-320.jpg)
![C
CARDIOVASCULAR SYSTEM
137
Rx DILTIAZEM
Oral: 60 mg tablet (as hydrochloride)
60 mg, 120 mg, 180 mg, and 240 mg MR capsule (as
hydrochloride)
120 mg and 180 mg MR tablet (as hydrochloride)
A non-dihydropyridine calcium channel blocker, which has a
negative chronotropic effect, thus decreasing the
workload of the heart, and consequently reducing its
oxygen requirements.
Indication: Prophylaxis and treatment of angina
Contraindications: Marked bradycardia (<40
beats/minute); sick sinus syndrome (without
pacemaker); severe hypotension (<90 mmHg systolic);
CHF; acute porphyria; second- or third-degree AV block
(without pacemaker); Wolff-Parkinson-White syndrome;
acute MI and pulmonary congestion; pregnancy
Dose:
Angina, by mouth, ADULT, initially 30 mg 3 or 4 times daily;
increase as required or at 1- to 2-day interval until
optimum response is obtained (maximum dose, 360 mg
daily in 3–4 divided doses); doses of up to 360 mg/day
may be needed in unstable angina;
controlled-release products, initially 180 mg once daily;
increase as required up to 360 mg once daily.
NOTE: Dose should not be increased if heart rate drops to
50 beats/minute.
Dose Adjustment:
Geriatric:
Start treatment at a lower dose.
Renal Impairment:
Start treatment at a lower dose. Use with caution.
Hepatic Impairment:
For mild-to-moderate hepatic impairment, dose reduction
may be warranted.
For severe impairment, refer patient to a specialist.
Adverse Drug Reactions:
Common: Abdominal pain, bradycardia, dizziness, dyspnea,
congestion, flushing, headache, fatigue, nausea,
nervousness, pain, palpitations, peripheral edema,
vasodilation, vomiting
Less Common: AV block, gout
Rare: Depression, EPS, gum hyperplasia, gynecomastia,
hepatitis, hypersensitivity reactions, photosensitivity
reactions, rash
Drug Interactions:
Monitor closely with:
Increases risk of adverse or toxic effects of Diltiazem:
Drugs causing hypotension, bradycardia, or slow cardiac
conduction, e.g., Amlodipine, Diazepam, Methyldopa;
Hydrochlorothiazide (bradycardia; hypotension)
Increases risk of adverse or toxic effects of the following
drugs:
Carbamazepine, Digoxin, Midazolam (sedative and
respiratory depressant effects; due to decreased
metabolism), Phenytoin, Ritonavir (due to increased
serum concentration)
Reduces therapeutic effect of Rifampicin (due to increased
metabolism)
Avoid concomitant use with:
Increases risk of adverse or toxic effects of the following
drugs due to increased serum concentration:
Colchicine, HMG-CoA Reductase Inhibitors, e.g.,
Atorvastatin, Simvastatin (rhabdomyolysis; myopathy)
Administration: Normal release preparations may be taken
with or without food. Administer immediate-release
preparations before meals and at bedtime. For long-
acting dosage forms, swallow whole. Do NOT open, chew,
or crush.
NOTE: Serum levels may be elevated if taken with food.
See General Information on Calcium Channel Blockers –
Selective Calcium Channel Blockers with Direct Cardiac
Effects in Chapter 3: Cardiovascular System for other
information.
Pregnancy Category: C
ATC Code: C08DB01
Rx VERAPAMIL
Oral: 80 mg tablet (as hydrochloride)
240 mg MR tablet (as hydrochloride)
Inj.: 2.5 mg/mL (as hydrochloride), 2 mL ampule (IV)
A calcium channel blocker that inhibits calcium ion from
entering the “slow channels” or select voltage-sensitive
areas of vascular smooth muscle and myocardium
during depolarization, producing relaxation of coronary
vascular smooth muscle and coronary vasodilation.
Indication: Treatment of angina pectoris (vasospastic,
chronic stable, unstable), supraventricular arrhythmia,
and hypertension.
Contraindications: Severe left ventricular dysfunction;
hypotension (systolic pressure <90 mm Hg) or
cardiogenic shock; sick sinus syndrome (except in
patients with a functioning pacemaker) ; second- or third-
degree AV block (except in patients with a functioning
pacemaker) ; atrial flutter or fibrillation and an accessory
bypass tract (Wolff-Parkinson-White [WPW] syndrome,
Lown-Ganong-Levine syndrome)
Dose:
Angina, by mouth, ADULT, immediate-release tablets,
initially 80-120 mg 3 times daily; usual dose range, 80-
160 mg 3 times daily;
modified-release tablets, initially 180 mg once daily at
bedtime; if inadequate response, may increase dose at
weekly intervals to 240 mg once daily, then 360 mg once](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-181-320.jpg)
![C
CARDIOVASCULAR SYSTEM
138
daily, then 480 mg once daily (maximum dose, 480 mg
daily).
Hypertension, by mouth, ADULT, immediate-release tablets,
initially 80-120 mg 3 times daily; usual dose range, 80-
160 mg 3 times daily;
sustained-release tablets, initially 180-240 mg once
daily at bedtime.
Dose Adjustment:
Renal Impairment:
Use with caution. Monitor ECG.
Hepatic Impairment:
Dose reduction may be required.
In patients with cirrhosis, reduce dose to 20% of normal
dose. Monitor ECG.
Adverse Drug Reactions:
Common: Peripheral edema, hypotension, CHF, pulmonary
edema, AV block, bradycardia, flushing, headache,
fatigue, dizziness, lethargy, pain, sleep disturbance,
rash, gingival hyperplasia, constipation, dyspepsia,
nausea, diarrhea, myalgia, paresthesia, dyspnea, flulike
syndrome
Less Common: Abdominal discomfort, alopecia, angina,
arthralgia, atrioventricular dissociation, blurred vision,
bruising, cerebrovascular accident, chest pain,
claudication, confusion, diaphoresis, ECG abnormal,
equilibrium disorders, erythema multiforme, exanthema,
extrapyramidal symptoms, galactorrhea or
hyperprolactinemia, gastrointestinal distress,
gynecomastia, hyperkeratosis, impotence, insomnia,
macules, MI, muscle cramps, palpitation, psychosis,
purpura (vasculitis), shakiness, somnolence, spotty
menstruation, SJS, syncope, tinnitus, urination
increased, urticaria, weakness, xerostomia, asystole,
eosinophilia, EPS, exfoliative dermatitis, GI obstruction,
hair color change, paralytic ileus, Parkinsonian
syndrome, pulseless electrical activity, shock, ventricular
fibrillation
Drug Interactions:
NOTE: Verapamil is a substrate of CYP1A2 (minor), CYP2B6
(minor), CYP2C9 (minor), CYP2E1 (minor), CYP3A4
(major), and P-glycoprotein.
Monitor closely with:
Decreases metabolism of the following drugs:
Pimecrolimus, Tacrolimus
Enhances antihypertensive effect of Verapamil:
Alfuzosin; Alpha1 Blockers e.g. Clonidine;
Anilidopiperidine Opioids e.g. Fentanyl; Barbiturates e.g.
Phenobarbital, Brimonidine (Topical); Diazoxide;
Magnesium Salts; MAO Inhibitors [except Linezolid,
Tedizolid]; Molsidomine; Nicorandil; Pentoxifylline;
Phosphodiesterase-5 Inhibitors e.g. Sildenafil;
Prostacyclin Analogues e.g. Epoprostenol; Quinidine,
Other Antihypertensive Agents
Enhances therapeutic effects of Verapamil:
Bradycardic effect: Anilidopiperidine Opioids, Bretylium
(AV blockade), Other Bradycardia-causing Agents,
Regorafenib, Ruxolitinib, Tofacitinib
AV blocking effect: Clonidine, Bretylium
Enhances therapeutic effect of the following drugs:
Aripiprazole, Beta Blockers [except Levobunolol,
Metipranolol] (hypotensive effect), Cardiac Glycosides
(AV blocking effect), Ethyl Alcohol, Fingolimod
(bradycardic effect), Lacosamide (AV blocking effect),
Midodrine (bradycardic effect), Non-depolarizing
Neuromuscular-blocking Agents e.g. Atracurium
(neuromuscular-blocking effect), Nitroprusside
(hypotensive effect), Salicylates (anticoagulant effect)
Increases risk of adverse or toxic effects of Verapamil:
MAO Inhibitors [except Linezolid, Tedizolid] (orthostatic
hypotension); Other Antihypertensive Agents
Avoid concomitant use with:
Decreases metabolism of Verapamil:
Azole Derivatives (Systemic) e.g. Ketoconazole,
Carbamazepine, Cyclosporine (Systemic), CYP3A4
Inhibitors (Strong), Macrolide Antibiotics [except
Azithromycin, Fidaxomicin, Spiramycin], Protease
Inhibitors e.g. Indinavir [reduce Verapamil dose by 50%]
Enhances therapeutic effect of Verapamil:
Cimetidine, Ivabradine (QTc-prolonging effect),
Telithromycin (bradycardic effect; antihypertensive
effect)
Enhances therapeutic effect of the following drugs:
Amiodarone (bradycardic effect) Ceritinib (bradycardic
effect), Dantrolene (negative inotropic effect),
Dronedarone (AV-blocking effect and other
electrophysiologic effects), Ivabradine (bradycardic
effect), Tizanidine
Increases metabolism of Verapamil:
CYP3A4 Inducers, Nafcillin
Increases risk of adverse or toxic effects of Verapamil:
Azole Derivatives e.g., Ketoconazole (Systemic) (negative
inotropic effects); Calcium Channel Blockers,
Dihydropyridine e.g. Amlodipine (hypotensive effect),
Dantrolene (hyperkalemic effect), Mifepristone,
Protease Inhibitors (AV nodal blockade), Stiripentol
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine [withhold Verapamil 24 hours prior to
Amifostine administration], Amiodarone (sinus arrest),
Avanafil, Budesonide (corticosteroid excess),
Carbamazepine, Ceritinib (symptomatic bradycardia),
Colchicine (Colchicine toxicity), Disopyramide (profound
depression of myocardial contractility), Fosphenytoin
(Phenytoin toxicity), Ibrutinib; Lovastatin [initiate
Lovastatin at 10 mg daily; do not exceed 20 mg daily]
(myositis; rhabdomyolysis), Obinutuzumab [withhold
Nicardipine 12 hours prior to Obinutuzumab infusion
until 1 hour after the end of the infusion] (hypotensive
effect), Oxycodone, Phenytoin, Rituximab (hypotensive
effect), Sonidegib (musculoskeletal adverse reactions),
Tizanidine, Ulipristal, Zopiclone
Increases serum concentration of Verapamil:
Atorvastatin, Cimetidine, Conivaptan, Fusidic Acid
(Systemic), Grapefruit Juice, Mifepristone, Protease
Inhibitors e.g. Indinavir [reduce Verapamil dose by 50%]
Stiripentol](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-182-320.jpg)
![C
CARDIOVASCULAR SYSTEM
139
Increases serum concentration of the following drugs:
Vincristine (Liposomal); Zopiclone [initial Zopiclone dose
should not exceed 3.75 mg]
Reduces therapeutic effect of Verapamil:
Carbamazepine, Phenytoin
TEST INTERACTION. May produce a false-positive result in the urine
detection of Methadone.
Administration: May be administered without regard to
meals. Do NOT crush or chew MR products.
For Calan SR, Isoptin SR, administer with food or milk.
Pregnancy Category: C
ATC Code: C08DA01
See Verapamil under Cardiac Therapy – Antiarrhythmics
(Class IV Antiarrhythmics) in Chapter 3: Cardiovascular
System for other information.
CENTRALLY ACTING
ANTIADRENERGIC AGENTS
Rx CLONIDINE
Oral: 75 micrograms and 150 micrograms tablet (as
hydrochloride)
Inj.: 150 micrograms/mL (as hydrochloride), 1 mL ampule
(IV)
An imidazoline-derived, centrally-acting agonist at alpha2-
adrenoceptors and imidazoline receptors, which acts by
reducing sympathetic tone resulting in BP lowering.
Indication: Hypertension (alone or used concomitantly with
other antihypertensive agents)
Contraindications: Bradyarrhythmia secondary to second- or
third-degree AV block or sick sinus syndrome.
Dose:
NOTE: Individualize dose based on patient’s BP response.
Hypertension, by mouth, ADULT, initially 75 micrograms 2–
3 times daily, increased by 75 micrograms daily every 2–
3 days (maximum dose, 1.2 mg daily; maintenance dose,
150–300 micrograms twice daily).
Hypertensive urgencies, by mouth, ADULT, 75 micrograms.
Dose Adjustment:
Renal Impairment:
Adjust dose according to the degree of impairment. Patients
may benefit from a lower initial dose.
For mild-to-moderate impairment, use with caution.
For severe impairment, refer to a specialist.
Precautions:
WARNING: Severe withdrawal syndrome (rebound
HTN) may occur after abrupt discontinuation.
Sudden cessation of treatment has, in some cases,
resulted in nervousness, agitation, headache, and
tremor accompanied or followed by a rapid rise in
BP and elevated catecholamine concentration in
the plasma.
Withdrawal syndrome (may be worsened by concomitant
administration of beta blockers; taper dose over 5–7
days before stopping the drug; excessive rise in BP
following discontinuation can be reversed by oral
administration).
Mild-to-moderate bradyarrhythmia, constipation, or
polyneuropathy (avoid use in patients with depression or
a history of it); coronary heart disease, severe coronary
insufficiency, conduction disturbances, recent MI,
cerebrovascular disease, Raynaud’s phenomenon or
other vasospastic peripheral vascular disease (may be
exacerbated).
CNS effects (may cause drowsiness; may increase effects
of alcohol); diabetes mellitus (may cause transient rise
in blood glucose); renal impairment (may worsen chronic
renal failure).
Surgery (stopping abruptly may precipitate a severe
withdrawal syndrome).
Elderly (can cause drowsiness); children (may be
particularly susceptible to hypertensive episodes
resulting from abrupt inability to take medication).
Pregnancy (may lower fetal heart rate; risk should be
balanced against the risk of uncontrolled maternal
hypertension; avoid IV injection); lactation (avoid use if
possible; limited data available; present in breastmilk;
may decrease prolactin secretion).
SKILLED TASKS. May impair ability to drive or operate machinery due
to drowsiness.
Adverse Drug Reactions:
Common: Constipation, depression, dizziness, drowsiness,
dry mouth, fatigue, headache, malaise, nausea,
orthostatic hypotension, salivary gland pain, sedation,
sexual dysfunction, sleep disturbances, vomiting.
Less Common: Bradycardia, confusion, delusion, disturbed
mental state, hallucination, itching, nightmare,
paresthesia, pruritus, rash, urticaria.
Rare: Alopecia, AV block, colonic pseudoobstruction,
decreased lacrimation, dry eyes, gynecomastia,
hepatitis, impaired visual accommodation, nasal
dryness, Raynaud’s phenomenon, urinary retention.
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Clonidine:
CNS Depressants [e.g., Alcohol, Barbiturates, Other
Sedating Drugs], Drugs that affect sinus node function or
AV nodal conduction [e.g., Digitalis, CCB (AV block;
bradycardia)]
Increases risk of adverse or toxic effects of Clonidine:
CNS Depressants [e.g., Alcohol, Barbiturates, Other
Sedating Drugs (sedation; bradycardia; hypotension)],
Drugs that reduce blood pressure and slow heart rate
(bradycardia; hypotension)](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-183-320.jpg)
![C
CARDIOVASCULAR SYSTEM
140
Avoid concomitant use with:
Increases risk of adverse or toxic effects of Clonidine:
Beta Blockers e.g., Propranolol (bradycardia;
hypotension; paradoxical increase in BP), Drugs that
reduce blood pressure and slow heart rate (bradycardia;
hypotension)
Reduces therapeutic effect of Clonidine:
Tricyclic Antidepressants e.g. Amitryptilline
(antihypertensive effect)
Administration: If further increments are needed to produce
the desired response, take larger portion of the oral daily
dose at bedtime to minimize drowsiness and dry mouth.
Advise the patient to get up gradually from sitting or lying
to minimize this effect, and to sit or lie down if the patient
becomes dizzy or light-headed.
Pregnancy Category: C
ATC Code: C02AC01
Rx METHYLDOPA
Oral: 250 mg tablet
A centrally-acting, alpha2-adrenoceptor agonist that is
useful in the management of hypertension in pregnancy.
Indication: For gestational hypertension and chronic
hypertension in pregnant women.
Contraindications: Pheochromocytoma; active liver disease;
depression, porphyria; patients in whom previous
methyldopa treatment resulted in liver abnormalities, or
direct Coombs’ positive hemolytic anemia
Dose:
Hypertension in pregnancy, by mouth, ADULT, initially 250
mg 2–3 times daily; gradually increase at intervals of 2
or more days, if necessary; (maximum dose, 3 g daily).
Dose Adjustment:
Renal Impairment:
Start with a small dose or adjust dosage frequency. May
require only usual initial dose.
For severe impairment, refer patient to a specialist.
Precautions:
Avoid abrupt withdrawal; monitor blood count and liver
function before treatment and at intervals during first 6–
12 weeks, or if unexplained fever occurs.
History of depression (may be exacerbated).
Renal impairment (increased sensitivity to hypotensive and
sedative effects); Hepatic impairment (caution in history
of liver disease; avoid use if possible).
Lactation (amount in breastmilk is too small to be harmful).
SKILLED TASKS. May impair ability to perform skilled or
hazardous tasks, e.g., operating machinery or driving.
Adverse Drug Reactions:
Common: Diarrhea, dizziness, dryness of mouth, fatigue,
fever, headache, light-headedness, positive Coombs’
test, sedation, tiredness, weakness.
Less Common: Angina, bradycardia, constipation,
depression, edema, sodium and water or fluid retention,
hemolytic anemia, impaired concentration and memory,
decreased libido and impotence in men, nasal
congestion, orthostatic hypotension, psychosis, rash,
sleep disturbance, sore or “black” tongue.
Rare: Arthralgia, bone marrow depression, hepatotoxicity
with acute or chronic active hepatitis or hepatic necrosis,
hyperprolactinemia, hypersensitivity reactions, jaundice,
leukopenia, myocarditis, nausea, pancreatitis,
Parkinsonism, pericarditis, sialadenitis, stomatitis,
thrombocytopenia, toxic epidermal necrolysis, urine
darkens on standing, vomiting.
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Methyldopa:
Antihypertensive effect: Chlorpromazine, Drugs that
reduce blood pressure
Increases risk of adverse or toxic effects of Methyldopa:
Chlorpromazine (extrapyramidal effects), Salbutamol
(acute hypotension)
Avoid concomitant use with:
Reduces therapeutic effect of Methyldopa:
Ibuprofen (antagonizes antihypertensive effect), Iron
Preparations {e.g., Ferrous Sulfate, Ferrous Gluconate
[due to reduced bioavailability] (antihypertensive
effect)}, Oral Contraceptives (Estrogen antagonizes
antihypertensive effect)
TEST INTERACTION. Produces a positive direct Coombs’
Test, interfering with blood cross-matching.
Administration: May be taken with or without food.
Advise the patient to get up gradually from sitting or lying
to minimize this effect, and to sit or lie down if the patient
becomes dizzy or light-headed.
Pregnancy Category: B
ATC Code: C02AB01 (levorotatory)
C02AB02 (racemic)
DIURETICS
LOW-CEILING DIURETICS
Rx HYDROCHLOROTHIAZIDE
Oral: 12.5 mg and 25 mg tablet
A moderately-potent, thiazide diuretic whose maximal
antihypertensive effect is usually observed at doses
lower than those that produce maximal diuretic effect. It
acts by blocking the reabsorption of sodium in the distal
convoluted tubules of the nephrons.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-184-320.jpg)

![C
CARDIOVASCULAR SYSTEM
142
Electrolyte disturbances (severe hyponatremia with
hypokalemia has been reported; dose-dependent;
hypochloremic alkalosis, hypomagnesemia, or
hypercalcemia may occur); photosensitivity; sulfonamide
(potential for T-cell-mediated type IV reactions).
Diabetes (may alter glucose control); gout (can be
precipitated).
Hypercholesterolemia (may increase cholesterol
concentration).
Hypokalemia (use with caution; correct before initiating
therapy).
Hepatic impairment (use with caution; undergoes extensive
hepatic metabolism; electrolyte and acid / base
imbalance in cirrhosis might lead to hepatic
encephalopathy).
Renal impairment (use with caution; approximately 70% is
excreted in the urine).
Systemic lupus erythematosus (can cause exacerbation or
activation).
Elderly (increased risk for severe hyponatremia with
hypokalemia in elderly women).
Pregnancy (crosses the placenta; found in cord blood; may
cause fetal or neonatal jaundice, thrombocytopenia, or
other adverse events); lactation (not known if excreted in
breast milk).
Adverse Drug Reactions:
Common: Agitation, anxiety, dizziness, fatigue, headache,
irritability, lethargy, malaise, nervousness, pain, tension,
tiredness, hypokalemia, back pain, muscle cramps or
spasm, paresthesia, weakness, rhinitis, infection,
arrhythmia, chest pain, flushing, orthostatic hypotension,
palpitation, peripheral edema, PVC, vasculitis,
depression, drowsiness, insomnia, lightheadedness,
vertigo, hives, pruritus, rash, hyperglycemia,
hyperuricemia, hypochloremia, hyponatremia,
decreased libido, abdominal pain, anorexia,
constipation, cramping, diarrhea, dyspepsia, gastric
irritation, nausea, vomiting, weight loss, xerostomia,
nocturia, polyuria, hypertonia, blurred vision,
conjunctivitis, glycosuria, cough, pharyngitis, rhinorrhea,
sinusitis, flulike syndrome
Less Common: Agranulocytosis, anaphylactic reaction,
aplastic anemia, bullous eruptions, erythema
multiforme, fever, hepatitis, hypercalcemia, cholestatic
jaundice, leukopenia, pancreatitis, photosensitivity,
pneumonitis, purpura, Stevens-Johnson syndrome,
thrombocytopenia, torsade de pointes
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Indapamide:
Antihypertensive effects: ACE Inhibitors, Alfuzosin,
Brimonidine [Topical], Diazoxide, Ethyl Alcohol, Herbs
with hypotensive properties, MAO Inhibitors [except
Linezolid, Tedizolid], Methylphenidate, Molsidomine,
Nicorandil, Other Antihypertensives, Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g. Sildenafil,
Prostacyclin Analogues e.g. Epoprostenol
Enhances therapeutic effect of the following drugs:
QTc-prolonging Agents, Ivabradine (arrhythmogenic
effect)
Increases risk of adverse or toxic effects of Indapamide:
Barbiturates e.g. Phenobarbital (orthostatic
hypotension), Beta2 Agonists (hypokalemia), Calcium
Salts (metabolic alkalosis due to decreased excretion of
Calcium Salts), Corticosteroids (hypokalemia),
Dexketoprofen, Ethyl Alcohol (orthostatic hypotension),
Opioid Analgesics, Other Antihypertensive Agents,
Licorice (hypokalemia), Multivitamins / Fluoride with ADE
(hypercalcemic effect), Multivitamins / Minerals [with
ADEK, Folate, Iron (hypercalcemic effect)], Multivitamins
/ Minerals [with AE, no Iron
Increases risk of adverse or toxic effects of the following
drugs:
ACE Inhibitors (nephrotoxicity), Allopurinol (allergic or
hypersensitivity reactions), Carbamazepine
(hyponatremia), Cardiac Glycosides (toxicity due to
hypokalemic and hypomagnesemic effects of
Indapamide), Cyclophosphamide (granulocytopenia),
Diazoxide, Duloxetine (orthostatic hypotension),
Levodopa (orthostatic hypotension), MAO Inhibitors
[except Linezolid, Tedizolid] (orthostatic hypotension),
Oxcarbazepine (hyponatremia), Porfimer
(photosensitizing effect)
Reduces therapeutic effect of Indapamide:
Herbs with hypertensive properties, NSAIDS
Reduces therapeutic effect of Antidiabetic Agents
Avoid concomitant use with:
Decreases absorption of Indapamide:
Bile Acid Sequestrants e.g. Cholestyramine
Decreases excretion of Lithium
Enhances therapeutic effect of the following drugs:
Dofetilide (QTc-prolonging effect), QTc-prolonging Agents
Increases risk of adverse or toxic effects of Indapamide:
Mifepristone (QTc-prolonging effect), SSRIs e.g.
Fluoxetine (hyponatremic effect)
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine (hypotensive effect), Levosulpiride, Rituximab
(hypotensive effect), Sodium Phosphates (nephrotoxic
effect, specifically the risk of acute phosphate
nephropathy), Topiramate (hypokalemic effect),
Risperidone (hypotensive effect), Verteporfin
(photosensitizing effect), Vitamin D Analogues
(hypercalcemic effect)
Increases serum concentration of the following drugs:
Dofetilide, Topiramate
Reduces therapeutic effect of Indapamide:
Bile Acid Sequestrants e.g. cholestyramine (diuretic
response)
Administration: May be administered without regard to
meals. Administer with food or milk to decrease GI
adverse effects.
Administer early in the day to avoid nocturia.
Swallow whole. Do NOT crush or chew.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-186-320.jpg)
![C
CARDIOVASCULAR SYSTEM
143
Pregnancy Category: B
ATC Code: C03BA11
HIGH-CEILING DIURETICS
Rx BUMETANIDE
Oral: 1 mg tablet
Inj.: 500 micrograms/mL, 4 mL ampule (IM, IV)
A loop diuretic that inhibits reabsorption of sodium and
chloride in the ascending loop of Henle and proximal
renal tubule, interfering with the chloride-binding
cotransport system, thus causing increased excretion of
water, sodium, chloride, magnesium, phosphate, and
calcium.
Indications: Management of congestive heart failure;
management of edema secondary to heart failure or
hepatic or renal disease, including nephrotic syndrome
Contraindications: Anuria; hepatic coma or states of severe
electrolyte depletion until the condition improves or is
corrected
Dose:
Heart failure, by mouth, ADULT, 0.5–2 mg 1–2 times daily;
may repeat in 4–5 hours for up to 2 doses (maximum
dose, 10 mg daily);
by IM or IV injection, 0.5–1 mg per dose; may repeat in
2–3 hours for up to 2 doses (maximum dose, 10 mg
daily).
Edema, by mouth, ADULT, 0.5–2 mg 1–2 times daily; may
repeat in 4–5 hours for up to 2 doses (maximum dose,
10 mg daily);
by IM or IV injection, 0.5–1 mg per dose; may repeat in
2–3 hours for up to 2 doses (maximum dose, 10 mg
daily;
by mouth, IM or IV injection, CHILD and INFANT, 0.015–
0.1 mg/kg per dose every 6–24 hours (maximum dose,
10 mg daily).
NOTE: Adjust doses based on individual patient’s needs.
Dose equivalency for patients with normal renal function
(approximate): Furosemide 40 mg = Bumetanide 1 mg =
Torsemide 20 mg = Ethacrynic Acid 50 mg
Precautions:
WARNING: Bumetanide is a potent diuretic. If given in
excess, can lead to a profound diuresis with water
and electrolyte depletion. Careful medical
supervision is required.
Fluid or electrolyte loss (can lower serum calcium
concentrations; can predispose a patient to serious
cardiac arrhythmias),
Hyperuricemia; Nephrotoxicity (monitor fluid status and
renal function to prevent oliguria, azotemia, and
reversible increases in BUN and creatinine),
Ototoxicity (may occur with rapid IV administration, renal
impairment, excessive doses, and concurrent use of
other ototoxins),
Sulfonamide allergy (may stimulate T-cell-mediated type IV
reactions),
Cirrhosis and ascites (sudden changes in fluid and
electrolyte balance and acid / base status may lead to
hepatic encephalopathy; increased risk of precipitating
hepatic coma),
Renal impairment (may exhibit diminished effects;
increased risk of adverse effects).
Diuretic resistance (can be overcome by IV administration,
use of two diuretics together, or the use of a diuretic with
a positive inotropic agent; monitor serum electrolytes
very closely).
Surgical patients (may render the patient volume depleted
and blood pressure may be labile during general
anesthesia if given the morning of surgery),
Elderly (excess amounts can lead to profound diuresis with
fluid and electrolyte loss; severe loss of sodium and/or
increase in BUN can cause confusion); neonates (potent
displacer of bilirubin in critically ill patients),
Pregnancy (adverse events have been observed in animal
reproduction studies); lactation (not known if excreted in
breastmilk; can decrease milk volume and suppress
lactation; breastfeeding is not recommended),
Adverse Drug Reactions:
Common: Dizziness, hyperuricemia, hypochloremia,
hypokalemia, hyponatremia, hyperglycemia, phosphorus
change, variations in bicarbonate and CO2 content,
abnormal serum calcium, abnormal lactate
dehydrogenase, azotemia, and muscle cramps.
Less Common: Abdominal pain, arthritic pain, asterixis,
auditory impairment, brain disease (preexisting liver
disease), chest pain, dehydration, diaphoresis, diarrhea,
dyspepsia, ECG changes, erectile dysfunction, fatigue,
glycosuria, headache, hyperventilation, hypotension,
musculoskeletal pain, nausea, nipple tenderness,
orthostatic hypotension, otalgia, ototoxicity, premature
ejaculation, proteinuria, pruritus, renal failure, skin rash,
Stevens-Johnson syndrome, thrombocytopenia, toxic
epidermal necrolysis, urticaria, vertigo, vomiting,
weakness, xerostomia
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Bumetanide:
Antihypertensive effect: Alfuzosin, Barbiturates e.g.
Phenobarbital, Brimonidine [Topical], Diazoxide, Herbs
with hypotensive properties, MAO Inhibitors [except
Linezolid, Tedizolid], Molsidomine, Nicorandil, Other
Antihypertensive Agents, Pentoxifylline,
Phosphodiesterase-5 Inhibitors e.g. Sildenafil,
Prostacyclin Analogues e.g., Epoprostenol
Diuretic effect: Fosphenytoin
Enhances therapeutic effect of the following drugs:
Dofetilide (QTc-prolonging effect), Ivabradine
(arrhythmogenic effect), Neuromuscular-blocking Agents
(neuromuscular-blocking effect)
Increases risk of adverse or toxic effects of Bumetanide:
Beta2 Agonists (hypokalemic effect), Corticosteroids
(hypokalemic effect), Cyclosporine, Licorice](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-187-320.jpg)
![C
CARDIOVASCULAR SYSTEM
144
(hypokalemic effect), Opioid Analgesics, Other
Antihypertensive Agents, Probenecid
Increases risk of adverse or toxic effects of the following
drugs:
ACE Inhibitors (hypotensive and nephrotoxic effects),
Allopurinol, Aminoglycosides (nephrotoxicity; ototoxicity),
Cardiac Glycosides (hypokalemia; hypomagnesemia),
Cisplatin (nephrotoxicity; ototoxicity), Duloxetine
(orthostatic hypotension), Levodopa (orthostatic
hypotension), MAO Inhibitors [except Linezolid, Tedizolid]
(orthostatic hypotension), Topiramate (hypokalemic
effect)
Reduces therapeutic effect of Bumetanide:
Methylphenidate (antihypertensive effect), Phenytoin
(diuretic effect), Probenecid, Salicylates (diuretic effect),
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Neuromuscular-blocking Agents
(neuromuscular-blocking effect)
Avoid concomitant use with:
Decreases absorption of Bumetamide:
Bile Acid Sequestrants e.g. Cholestryamine
Enhances therapeutic effect of Bumetanide:
Canagliflozin (antihypertensive effect)
Increases risk of adverse or toxic effects of the following
drugs:
Hypotensive effect: Amifostine, Levosulpiride,
Obinutuzumab, Risperidone, Rituximab
Sodium Phosphates (nephrotoxic effect, specifically,
acute phosphate nephropathy)
Increases serum concentration of Bumetanide:
Methotrexate
Increases serum concentration of the following drugs:
Foscarnet, Methotrexate
Reduces therapeutic effect of Bumetanide:
Methotrexate, NSAIDS (diuretic effect)
Administration:
For oral administration, take without food. Administering
with food slows the rate of absorption and reduces the
extent of absorption and may reduce diuretic efficacy.
May require increased intake of potassium-rich foods.
Administer an alternate-day schedule or a 3–4 daily
dosing regimen with rest periods of 1–2 days in between.
For IV administration, administer slowly, over 1–2
minutes.
Pregnancy Category: C
ATC Code: C03CA02
Rx FUROSEMIDE
Oral: 20 mg and 40 mg tablet
Inj.: 10 mg/mL, 2 mL ampule (IM, IV)
10 mg/mL, 25 mL ampule (IV infusion)
A potent, high-ceiling, sulfonamide loop diuretic, which
produces dose dependent diuresis of relatively short
duration.
Indications: Management of edema; pulmonary edema;
cerebral edema; hepatic cirrhosis; nephrotic syndrome;
oliguria due to renal failure; congestive heart failure
Contraindication: Severe fluid and sodium depletion
Dose:
Edema, by mouth, ADULT, 40 mg daily in divided doses, may
be increased gradually to 120 mg in resistant edema;
CHILD, 1–3 mg/kg daily (maximum, 40 mg daily);
INFANT, 1–6 mg/kg daily given in divided doses every 6–
12 hours; NEONATES or PREMATURE INFANTS, 1–4
mg/kg per dose once or twice daily due to poor
bioavailability;
by IV injection, NEONATES or PREMATURE INFANTS, 1–2
mg/kg per dose every 12–24 hours;
by continuous IV infusion, NEONATES or PREMATURE
INFANTS, 0.05 mg/kg per hour (maximum, 0.4 mg/kg
per hour).
Heart failure, by mouth, ADULT, initially 20–40 mg; may
repeat the same dose or increase dose in increments of
20–40 mg per dose at intervals of 6–8 hours (maximum
total daily dose, 600 mg); usual maintenance dose
interval is once or twice daily; adjust dosing frequency
based on patient-specific needs; CHILD and INFANT,
initially 2 mg/kg per dose, increased in increments of 1–
2 mg/kg per dose at intervals of 6–8 hours until a
satisfactory response is achieved (maximum dose, 6
mg/kg per dose);
by IM or IV injection, ADULT, initially 20–40 mg per dose,
may repeat the same dose or increase dose in
increments of 20 mg per dose and administer 1–2 hours
after previous dose (maximum dose, 200 mg per dose);
given once or twice daily; CHILD and INFANT, initially 1
mg/kg per dose, may increase dose in increments of 1
mg/kg per dose and administer not sooner than 2 hours
after previous dose, until a satisfactory response is
achieved; may administer maintenance dose at intervals
of every 6–12 hours (maximum dose, 6 mg/kg per dose);
by continuous IV infusion, ADULT, initially administer an
IV bolus dose 40–100 mg over 1 to 2 minutes, followed
by continuous IV infusion rate of 10–40 mg/hour; repeat
loading dose before increasing infusion rate.
Acute pulmonary edema, by slow IV injection, ADULT, 40 mg
initially, dose may be doubled every hour until a ceiling
dose of 160 mg; CHILD 1 mg/kg daily (maximum,
6mg/kg daily);
by slow IV drip or infusion, ADULT, 40 mg/hour.
Oliguria with glomerular filtration rate <20 mL/minute, by
slow IV infusion at a rate not exceeding 4 mg/minute,
ADULT, initially 250 mg over 1 hour; if urine output is not
satisfactory during the hour after the first dose, infuse
500 mg over 2 hours then, if there is no satisfactory
response during the hour after the second dose, infuse
1 g over 4 hours; if there still is no response after the](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-188-320.jpg)
![C
CARDIOVASCULAR SYSTEM
145
third dose, dialysis is probably necessary; may repeat
effective dose, up to 1 g, every 24 hours.
Dose Adjustment:
Geriatric:
Reduce dose.
Renal Impairment:
In acute renal failure, higher doses may be required to
initiate desired response. Avoid use in oliguric states.
Not removed by hemodialysis or peritoneal dialysis.
Supplemental dose is not necessary.
In CrCl <25 mL/minute, use upper end of the initial infusion
dosage range. If urine output is <1 mL/kg per hour,
double as necessary to a maximum of 80–160 mg/hour.
Monitor effects, particularly with high doses.
NOTE: Dose equivalency for patients with normal renal function
(approximate): Furosemide 40 mg = Bumetanide 1 mg =
Torsemide 20 mg = Ethacrynic Acid 50 mg
Precautions:
WARNING: Cases of tinnitus, hearing impairment,
and deafness have been reported. Ototoxicity is
related to rapid injection, severe renal impairment,
use of higher than recommended doses,
hyponatremia, or concomitant therapy with
aminoglycoside antibiotics or other ototoxic drugs.
If high doses are necessary, parenteral therapy
with controlled IV infusion is advisable.
Prostatic enlargement and/or obstruction (may precipitate
acute urinary retention).
Gout (may be aggravated by diuretic-induced
hyperuricemia).
Hypotension.
Diabetes (may see changes in glucose control); SLE (may
cause SLE exacerbation or activation).
Oliguria (correct hypovolemia before administration).
Renal impairment (monitor electrolytes particularly
potassium and sodium, as well as creatinine).
Hepatic impairment (hypokalemia may precipitate coma);
cirrhosis (diminished natriuretic effect with increased
sensitivity to hypokalemia and volume depletion);
alcoholic cirrhosis (increased risk of hypomagnesemia).
Severe urinary retention.
Patients at high risk for radiocontrast nephropathy (can lead
to higher incidence of deterioration in renal function).
Elderly (more susceptible to electrolyte imbalance and
orthostatic hypotension).
Pregnancy (avoid use; may cause electrolyte disturbance in
fetus; possible neonatal thrombocytopenia; monitor fetal
growth because of potential for higher fetal birth
weights); lactation (enters breastmilk; use with caution).
Adverse Drug Reactions:
Common: Dehydration, dizziness, gout, hyperuricemia,
hypokalemia, hypomagnesemia, hyponatremia,
orthostatic hypotension, syncope
Less Common: Dyslipidemia, hyperglycemia, hypocalcemia,
concentration, rash
Rare: Acute pancreatitis, agranulocytosis, bone marrow
depression, bullous eruptions, exfoliative dermatitis,
hemolytic anemia, interstitial nephritis, jaundice,
photosensitivity, Stevens-Johnson syndrome,
thrombocytopenia, tinnitus, vertigo
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Furosemide:
Alcohol (antihypertensive effect), Thiazide Diuretics [e.g.,
Hydrochlorothiazide (profound diuresis; serious
electrolyte disturbance)]
Increases risk of adverse or toxic effects of Furosemide:
Salbutamol (hypokalemia)
Increases risk of adverse or toxic effects of the following
drugs:
ACE Inhibitors [e.g., Enalapril (severe hypotension with
the first ACEi dose; ACEi-induced renal impairment)],
ARBs (excessive hypotension with the first ARB dose due
to volume depletion), Drugs causing hypotension [e.g.,
Amlodipine, Diazepam, Hydrochlorothiazide, Methyldopa
(hypotension)], Digoxin (cardiac toxicity due to
hypokalemia), NSAIDs including COX-2 Inhibitors
(nephrotoxicity), Ototoxic Drugs [e.g., Gentamicin,
Streptomycin (ototoxicity)]
Reduces therapeutic effect of Furosemide:
Selective and non-selective NSAIDs
Avoid concomitant use with:
Increases risk of adverse or toxic effects of Furosemide:
Hydrocortisone (hypokalemia)
Increases risk of adverse or toxic of Ibuprofen
(nephrotoxicity)
Reduces therapeutic effect of Furosemide:
Hydrocortisone (antagonism of diuretic effect), Ibuprofen
(antagonism of diuretic effect), Oral Contraceptives
(Estrogen antagonizes diuretic effect)
Reduces therapeutic effect of the following drugs:
Lidocaine (antagonized by hypokalemia), Metformin
(antagonism of hypoglycemic effect)
Administration:
For oral administration, take tablet once daily, in the
morning. If to be taken twice daily, take the first dose in
the morning and the second dose at lunchtime.
Advise the patient to get up gradually from sitting or lying
to minimize dizziness upon standing when taking the
medicine. The patient should sit or lie down if dizziness
occurs
For IV administration, administer no faster than 4
mg/minute to avoid ototoxicity. Dilute dose in a suitable
amount of infusion fluid, according to the hydration of
the patient.
Pregnancy Category: C
ATC Code: C03CA01](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-189-320.jpg)
![C
CARDIOVASCULAR SYSTEM
146
POTASSIUM-SPARING AGENTS
Rx SPIRONOLACTONE
Oral: 25 mg, 50 mg, and 100 mg tablet
A mineralocorticoid (aldosterone) receptor antagonist that
competes with aldosterone for receptor sites in the distal
renal tubules, increasing sodium chloride and water
excretion while conserving potassium and hydrogen ions.
Indications: Management of edema associated with
excessive aldosterone excretion or congestive heart
failure alone or in combination with other diuretics;
hypertension; primary hyperaldosteronism (establishing
diagnosis, short-term preoperative treatment, and long-
term maintenance therapy) ; hypokalemia; severe heart
failure (NYHA class IIIIV)
Contraindications: Anuria; acute renal insufficiency;
significant impairment of renal excretory function;
hyperkalemia; Addison disease; concomitant use with
eplerenone.
Dose:
Edema, by mouth, ADULT, 25–200 mg daily in 1–2 divided
doses; CHILD 1–17 years, 1 mg/kg daily, divided every
12–24 hours (maximum dose: 3.3 mg/kg daily, up to
100 mg daily).
Hypokalemia, by mouth, ADULT, 25–100 mg once daily.
Hypertension, by mouth, ADULT, 50–100 mg in 1–2 divided
doses; may adjust dose after 2 weeks (usual dosage
range, 25–50 mg daily); CHILD 1 to 17 years, 1 mg/kg
daily, divided every 12–24 hours (maximum dose: 3.3
mg/kg daily, up to 100 mg daily).
Diagnosis of primary aldosteronism, by mouth, ADULT,
long test, 400 mg once daily for 3–4 weeks; short test,
400 mg once daily for 4 days (maintenance until surgical
correction: 100–400 mg once daily).
Severe heart failure, NYHA class III–IV, by mouth, ADULT,
initially 12.5–25 mg once daily (maximum daily dose, 50
mg); if 25 mg once daily is not tolerated, reduce to 25 mg
every other day.
NOTE: To reduce delay in onset of effect, a loading dose of
2 or 3 times the daily dose may be administered on the
first day of therapy.
Dose Adjustment:
Geriatric:
Use with caution and monitor potassium closely. Avoid using
doses >25 mg daily in heart failure or reduced renal
function.
Renal Impairment:
In patients with heart failure:
If eGFR ≥50 mL/minute/1.73 m2, administer an initial
dose of 12.5–25 mg once daily (maintenance dose, 25
mg once daily; after 4 weeks of treatment with potassium
≤5 mEq/L).
If eGFR 30–49 mL/minute/1.73 m2, administer an initial
dose of 12.5 mg once daily or every other day
(maintenance dose, 12.5–25 mg once daily; after 4
weeks of treatment with potassium ≤5 mEq/L); if eGFR
<30 mL/minute/1.73 m2, use is not recommended.
Discontinue therapy if potassium >5 mEq/L or serum
creatinine >4 mg/dL. Withhold treatment if potassium
>5.5 mEq/L or renal function worsens. Hold doses until
potassium is <5 mEq/L and consider restarting with a
reduced dose after confirming resolution of
hyperkalemia or renal insufficiency for at least 72 hours.
SKILLED TASKS. May cause drowsiness or blurred vision.
Avoid performing tasks, which require mental alertness,
e.g., operating machinery or driving.
Precautions:
WARNING: Hazardous agent. Use appropriate
precautions for handling and disposal.
Spironolactone has been shown to be tumorigenic
in chronic toxicity studies in rats. Avoid
unnecessary use of this drug.
CNS effects (somnolence and dizziness have been
reported); gynecomastia (dose-related).
Fluid or electrolyte loss (excess amounts can lead to
profound diuresis); hyperkalemia (dose-related; rates of
hyperkalemia increase with declining renal function;
concurrent use of large doses of ACE inhibitors increases
the risk of hyperkalemia).
Adrenal vein catheterization; cirrhosis (avoid electrolyte and
acid / base imbalances that may lead to hepatic
encephalopathy); heart failure (eGFR should be >30
mL/minute/1.73 m2 or creatinine should be ≤2.5 mg/dL
(men) or ≤2 mg/dL (women) with no recent worsening,
and potassium should be <5 mEq/L with no history of
severe hyperkalemia; renal impairment (increased risk of
hyperkalemia).
Ethanol use (may increase risk of orthostasis).
Elderly (monitor patient for increased risk of hyperkalemia).
Pregnancy (crosses the placenta; have been shown to
cause feminization of the male fetus in animal studies;
avoid use during first trimester; avoid use in women of
reproductive potential); lactation (active metabolite,
canrenone, has been found in breastmilk; may decrease
milk volume and suppress lactation).
Adverse Drug Reactions:
Common: Vasculitis, ataxia, confusion, drowsiness,
headache, erythematous maculopapular rash, lethargy,
Stevens-Johnson syndrome, toxic epidermal necrolysis,
urticaria, amenorrhea, gynecomastia, hyperkalemia,
abdominal cramps, diarrhea, gastritis, gastrointestinal
hemorrhage, gastrointestinal ulcer, nausea, vomiting,
impotence, irregular menses, postmenopausal bleeding,
agranulocytosis, malignant neoplasm of breast,
hepatotoxicity, anaphylaxis, DRESS syndrome, increased
blood urea nitrogen, renal failure, renal insufficiency,
fever.
Drug Interactions:
Monitor closely with:
Enhances antihypertensive effect of Spironolactone:
Alfuzosin, Barbiturates, Brimonidine (Topical), Diazoxide,
Herbs with hypotensive properties, MAO Inhibitors
[except Linezolid, Tedizolid], Methylphenidate,](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-190-320.jpg)
![C
CARDIOVASCULAR SYSTEM
147
Molsidomine, Nicorandil, Other Antihypertensive Agents,
Pentoxifylline, Phosphodiesterase-5 Inhibitors,
Prostacyclin Analogues, Yohimbine
Enhances therapeutic effect of the following drugs:
ACE Inhibitors (hyperkalemic effect), Neuromuscular-
blocking Agents [Non-Depolarizing (neuromuscular-
blocking effect)], Quinidine
Increases risk of adverse or toxic effects of Spironolactone:
Angiotensin II Receptor Blockers (hyperkalemia),
Atorvastatin (enhanced effects on reducing endogenous
steroid activity), Canagliflozin (hyperkalemia;
hypotension), Cholestyramine Resin (metabolic acidosis;
hyperkalemia), Digoxin, Drospirenone (hyperkalemia),
Heparin (hyperkalemia), MAO Inhibitors [except
Linezolid, Tedizolid] (orthostatic hypotension), Nicorandil
(hyperkalemia), Nitrofurantoin (hyperkalemia),
Nonsteroidal Anti-Inflammatory Agents (hyperkalemia),
Opioid Analgesics, Other Antihypertensive Agents,
Tolvaptan (hyperkalemia), Trimethoprim (hyperkalemia)
Increases risk of adverse or toxic effects of the following
drugs:
Ciprofloxacin [Systemic (arrhythmogenic effect)],
Duloxetine (orthostatic hypotension), Levodopa
(orthostatic hypotension), Risperidone (hypotensive
effect)
Reduces antihypertensive effect of Spironolactone:
Nonsteroidal Anti-Inflammatory Agents
Reduces therapeutic effect of the following drugs:
Abiraterone acetate, Alpha / Beta Agonists
(vasoconstricting effect), Cardiac Glycosides (inotropic
effects)
Avoid concomitant use with:
Enhances therapeutic effect of the following drugs:
Mitotane
Increases risk of adverse or toxic effects of Spironolactone:
Hyperkalemia: Amiloride, Eplerenone, Potassium Salts,
Triamterene
Ammonium Chloride (systemic acidosis)
Increases risk of adverse or toxic effects of the following
drugs:
Amifostine (hypotensive effect), Cyclosporine [Systemic
(hyperkalemia)], Obinutuzumab (hypotensive effect),
Rituximab (hypotensive effect), Sodium Phosphates
(nephrotoxic effect, specifically, acute phosphate
nephropathy), Tacrolimus [Systemic (hyperkalemia)]
TEST INTERACTIONS. Produces a false increase in assays
used to determine digoxin concentrations.
Administration: Administer with food to increase absorption
and decrease GI upset.
Pregnancy Category: C
ATC Code: C03DA01
OTHER DIURETICS
Rx MANNITOL
Inj.: 20%, 250 mL and 500 mL bottle (IV)
A hexahydric alcohol related to mannose that acts as an
osmotic agent with little energy value. It is eliminated
from the body before any metabolism can take place.
When given parenterally, mannitol raises the osmotic
pressure of the plasma, thus drawing water out of body
tissues and producing an osmotic diuresis.
Indications: To reduce cerebral edema; to reduce increased
intraocular pressure
NOTE: NOT recommended for the prevention of acute renal
failure and/or promotion of diuresis.
Dose:
Increased intracranial pressure, cerebral edema, by IV
injection, ADULT, 0.25–1 g/kg per dose; may repeat
every 6–8 hours, as needed; maintain serum osmolality
<300–320 mOsm/kg; CHILD, 0.25–1 g/kg per dose;
repeat as needed to maintain serum osmolality <300–
320 mOsm/kg; administer over 30–60 minutes.
Reduction of intraocular pressure, by IV injection, ADULT,
0.25–2 g/kg administered over 30–60 minutes 1–1.5
hours prior to surgery; CHILD, 1 to 2 g/kg or 30–60 g/m2
administered over 30–60 minutes 1–1.5 hours prior to
surgery.
Reduction of intraocular pressure, traumatic hyphema, by IV
injection, ADULT, 1.5 g/kg administered over 45 minutes
twice daily for IOP >35 mm Hg; may administer every 8
hours; CHILD, 1.5 g/kg administered over 45 minutes
twice daily for IOP >35 mm Hg; may administer every 8
hours in patients with extremely high pressure.
Administration: Administer by intravenous route.
Concentration and rate of administration depends on
indication, severity, or adjusted to urine flow.
Inspect for crystals prior to administration. If crystals are
present, warm solution to re-dissolve crystals. Use filter
type administration set for infusion solutions greater
than or equal to 20%.
Do NOT administer until adequacy of renal function and
urine flow is established. Use 1–2 test doses to assess
renal response.
NEVER add to whole blood for transfusion or administer
through the same set by which blood is being infused to
prevent crenation and agglutination of red blood cells.
See Mannitol under Blood Substitutes and Perfusion
Solutions – I.V. Solutions producing Osmotic Diuresis in
Chapter 2: Blood and Blood Forming Organs for other
information.
Pregnancy Category: C
ATC Code: Not available](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-191-320.jpg)
![C
CARDIOVASCULAR SYSTEM
148
LIPID MODIFYING AGENTS
HMG CoA REDUCTASE INHIBITORS
Rx ATORVASTATIN
Oral: 10 mg, 20 mg, 40 mg, and 80 mg tablet (as calcium)
A selective, competitive inhibitor of 3-hydroxy-3-
methylglutaryl coenzyme A (HMG-CoA) reductase, which
prevents the conversion of HMG-CoA to mevalonate, an
early and rate-limiting step in cholesterol biosynthesis.
Indication: Adjunct to diet for the reduction of elevated total
cholesterol, LDL cholesterol, apolipoprotein B, and
triglycerides, and elevation HDL cholesterol in patients
with primary hypercholesterolemia and combined
hyperlipidemia
NOTE: Atorvastatin has not been studied in conditions
where the major lipoprotein abnormality is elevation of
chylomicrons (Fredrickson Types I and V).
Contraindications: Active liver disease, including
unexplained persistent elevations in hepatic
transaminase levels; pregnancy; breastfeeding
Dose:
NOTE: Individualize starting and maintenance doses
according to patient characteristics, such as goal of
therapy and response.
Hyperlipidemia, by mouth, ADULT, initially 10 or 20 mg once
daily; usual range, 10–80 mg once daily;
patients who require an LDL-C reduction of more than
45% may be started at 40 mg once daily.
Heterozygous Familial Hypercholesterolemia, by mouth,
CHILD 10–17 years, initially 10 mg daily (maximum
dose, 20 mg daily); adjust doses at intervals of 4 weeks
or more.
Homozygous Familial Hypercholesterolemia, by mouth,
ADULT, 10–80 mg daily.
Dose Adjustment:
Renal Impairment:
Hemodialysis does not have any significant effect on
atorvastatin clearance.
Hepatic Impairment:
In patients with active liver disease, use is contraindicated.
Precautions:
Skeletal muscle effects (rare cases of rhabdomyolysis with
acute renal failure secondary to myoglobinuria have
been reported; immune-mediated necrotizing myopathy,
IMNM, rarely occurs).
Liver dysfunction (jaundice has been reported; reversible
increases in liver function tests may occur); hepatic
impairment; endocrine function (increased HbA1c and
fasting serum glucose levels have been reported).
CNS toxicity (brain hemorrhage and CNS vascular lesions,
characterized by perivascular hemorrhages, edema, and
mononuclear cell infiltration of perivascular spaces have
been observed in animal studies); stroke or TIA (may
occur).
Elderly (use with caution; age ≥65 years is a predisposing
factor for myopathy); children (use of doses >20 mg has
not been studied).
Pregnancy (crosses the placenta; use with caution;
insufficient studies on use during pregnancy); lactation
(not known if excreted in breastmilk; use with caution).
Adverse Drug Reactions:
Common: Nasopharyngitis, arthralgia, diarrhea, pain in
extremity, urinary tract infection, dyspepsia, nausea,
musculoskeletal pain, muscle spasms, myalgia,
insomnia, pharyngolaryngeal pain
Less Common and Rare: Rhabdomyolysis, myopathy, liver
enzyme abnormalities, malaise, pyrexia, abdominal
discomfort, eructation, flatulence, hepatitis, cholestasis,
muscle fatigue, neck pain, joint swelling, hyperglycemia,
nightmare, epistaxis, urticaria, vision blurred, tinnitus,
positive WBC in urine, anaphylaxis, angioneurotic
edema, bullous rashes, fatigue, tendon rupture, fatal and
non-fatal hepatic failure, dizziness, depression,
peripheral neuropathy, pancreatitis
Drug Interactions:
Monitor closely with:
Increases distribution of the following drugs:
Oral Contraceptives [norethindrone; ethinyl estradiol]
Avoid concomitant use with:
Increases distribution of Atorvastatin:
Cyclosporine
Increases risk of adverse or toxic effects (myopathy) of
Atorvastatin:
Colchicine (including rhabdomyolysis), Cyclosporine,
CYP3A4 Inhibitors, i.e., Clarithromycin, HIV Protease
Inhibitors, Itraconazole, Fibric Acid Derivatives, Niacin
Increases serum concentration of Atorvastatin:
CYP3A4 Inhibitors (Strong) i.e., Clarithromycin, HIV
Protease Inhibitors, Itraconazole, Grapefruit Juice [avoid
excessive consumption, i.e., >1.2 L/day]
Administration: Administer as a single dose at any time of
the day, with or without food.
Pregnancy Category: X
ATC Code: C10AA05
Rx ROSUVASTATIN
Oral: 10 mg and 20 mg tablet (as calcium salt)
An active HMG-CoA reductase inhibitor, which is effective in
reducing LDL-cholesterol concentration and has been
efficacious in severe hypercholesterolemia.
Indications: Prevention of cardiovascular events in patients
at high risk of a first cardiovascular event; mixed
dyslipidemia, or homozygous familial
hypercholesterolemia in patients who have not
responded adequately to diet and other appropriate](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-192-320.jpg)
![C
CARDIOVASCULAR SYSTEM
149
measures; (adults) treatment of primary
hypercholesterolemia, e.g., heterozygous familial and
non-familial hypercholesterolemia; (children and
adolescents) treatment of heterozygous familial
hypercholesterolemia
Contraindications: Pregnancy; breastfeeding; women who
are planning to conceive or those using inadequate
contraception; severe renal impairment; active liver
disease; unexplained persistent elevation in serum
transaminases
Dose:
NOTE: Individualize doses based on baseline LDL-
cholesterol levels, recommended goal of therapy, and
patient response. Adjust doses at 4-week intervals or
more.
Reserve highest dose (40 mg) only for patients who fail
to achieve desired cholesterol level at 20 mg daily.
High cardiovascular risk, by mouth, ADULT MEN >50 years
and WOMEN >60 years, 20 mg once daily.
Hypercholesterolemia, by mouth, ADULT, initially 5 or 10 mg
once daily, may increase dose to 20 mg if necessary at
intervals of at least 4 weeks; usual range, 5–20 mg once
daily (maximum dose, 40 mg once daily); CHILD 10–18
years, initially 5 mg once daily (maximum dose, 20 mg
once daily).
Dose Adjustment:
Geriatric:
Start at low dose. Initiate dose at 5 mg once daily.
Renal Impairment:
For mild-to-moderate impairment, initiate dose at 5 mg once
daily with a maximum dose of 10 mg once daily.
Asian Ancestry:
Patients may build up higher drug levels and be at higher
risk to develop myopathy. Initiate dose at 5 mg. Do not
administer 40 mg dose.
Patients at Risk for Myopathy:
Consider lower initial dose, e.g., 5 mg daily in adults.
Precautions:
Renal impairment (may reduce elimination of rosuvastatin;
increases risk of myopathy); Hepatic effects (hepatic
impairment may impair elimination of rosuvastatin).
Myopathy (may occur with lipid lowering agent; monitor
creatine kinase (CK) levels and discontinue if these are
markedly elevated; increased risk for rhabdomyolysis);
immune-mediated necrotizing myopathy (have been
rarely reported)
Severe intercurrent illness, e.g., infection, trauma,
metabolic disorder, endocrine and electrolyte
disturbances, uncontrolled seizures (increases risk of
myopathy, rhabdomyolysis, and renal failure).
Diabetes mellitus (small increases in HbA1c and fasting
blood glucose have been reported); hematuria and
proteinuria; hypothyroidism (should be managed
adequately before starting treatment with a statin)
Treatment with systemic Sodium Fusidate (may increase
the risk of rhabdomyolysis)
Elderly (risk of myopathy is higher); children (safety and
efficacy have not been established in children <10 years;
establish a healthy lifestyle to reduce cardiovascular
risk)
Pregnancy (use during first trimester has been associated
with fetal malformation; decreased synthesis of
cholesterol may possibly affect fetal development);
lactation
Adverse Drug Reactions:
Common: Abdominal pain, arthralgia, constipation, diabetes
mellitus, dizziness, headache, flu-like illness, insomnia,
mild GI symptoms, myalgia, nausea, UTI, weakness
Less Common: Pruritus, rash, urticaria
Rare: Myopathy (including myositis), angioedema, alopecia,
amnesia, anaphylaxis, gynecomastia, hematuria,
hepatitis, hypersensitivity (rash, pruritus, urticaria),
impotence, interstitial lung disease, jaundice, liver
failure, pancreatitis, paresthesia, peripheral neuropathy,
proteinuria, rhabdomyolysis, renal failure, toxic
epidermal necrolysis
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Rosuvastatin:
Fibrates e.g. Fenofibrate (myopathy; rhabdomyolysis)
Avoid concomitant use with:
Enhances therapeutic effect of the following drugs:
Warfarin (increases INR)
Increases risk of adverse or toxic effects of Rosuvastatin:
Niacin (rhabdomyolysis; increased toxicity due to
pharmacodynamic synergism)
Increases risk of adverse or toxic effects of Warfarin
(bleeding)
Reduces absorption of Rosuvastatin:
Bile Acid Binding Resins [administer statin at least 1 hour
before, or 4 hours after, the resin]
Administration: May be taken with or without food. May be
taken at any time of the day.
Pregnancy Category: X
ATC Code: C10AA07
Rx SIMVASTATIN
Oral: 20 mg and 40 mg tablet
An HMG-CoA reductase inhibitor, which is effective in
reducing LDL cholesterol concentration, and has been
reported to reduce the incidence of fatal and non-fatal
MI, stroke and mortality, and the need for coronary and
non-coronary revascularization procedures.
Indications: For prevention of cardiovascular events in
patients with high cardiovascular risk due to
atherosclerotic cardiovascular disease or DM; primary
hypercholesterolemia; homozygous familial
hypercholesterolemia, or combined hyperlipidemia in](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-193-320.jpg)
![C
CARDIOVASCULAR SYSTEM
150
patients who have not yet responded adequately to diet
or other appropriate measures; (children and
adolescents) heterozygous familial
hypercholesterolemia
Contraindications: Known hypersensitivity to simvastatin or
any component of the formulation; active liver disease,
or persistently abnormal liver function tests; porphyria;
pregnancy (congenital anomalies reported; decreased
synthesis of cholesterol possibly affects fetal
development); breastfeeding
Dose:
Homozygous familial hypercholesterolemia, by mouth,
ADULT, initially 40 mg daily at night, adjusted at intervals
of at least 4 weeks (see restricted dosing with 80 mg
once daily at night).
Prevention of cardiovascular events, by mouth, ADULT,
initially 10–40 mg once daily at night, adjusted at
intervals of at least 4 weeks with recommended starting
dose of 40 mg for those at high risk of cardiovascular
events.
Primary hypercholesterolemia or combined hyperlipidemia,
by mouth, ADULT, 10–20 mg daily at night, adjusted at
intervals of at least 4 weeks (see restricted dosing with
80 mg once daily at night).
Heterozygous familial hypercholesterolemia, by mouth,
ADOLESCENT 10–18 years, initially 10 mg at night, may
increase if necessary, at intervals of at least 4 weeks to
a maximum of 40 mg at night.
NOTE: Maximum simvastatin dose:
with concomitant and diltiazem, 10 mg daily;
with concomitant amiodarone or amlodipine, 20 mg
daily. Contraindicated with erythromycin, clarithromycin,
ketoconazole, HIV protease inhibitors, and gemfibrozil.
Dose Adjustment:
Geriatric:
Use with caution. Start at low dose.
Renal Impairment:
For mild-to-moderate renal impairment, dose reduction is
warranted.
For severe impairment, refer patient to a specialist.
Hepatic Impairment:
Use with caution. Start at low dose. Contraindicated in
active liver disease or persistent abnormal liver function
tests.
Restricted Dosing for 80 mg:
Restrict use of 80-mg dose to patients who have been
taking Simvastatin 80 mg chronically, e.g., for 12 months
or more, without evidence of muscle toxicity, to minimize
the risk of myopathy, including rhabdomyolysis,
particularly during the first year of treatment.
Precautions:
Muscle effects (do not start simvastatin if creatine kinase
[CK] is elevated in patients at high risk of muscle effects;
risk of myopathy is increased if simvastatin is given at
high doses or with a fibrate, with lipid-lowering doses of
nicotinic acid, or with immunosuppressants; monitor
liver function and creatine kinase). Rhabdomyolysis
(rarely occurs; risk may be increased in renal impairment
and hypothyroidism).
Severe intercurrent illness, e.g., infection, trauma, or
metabolic disorder (increased risk of myopathy,
rhabdomyolysis, and renal failure;); hypothyroidism
(should be managed before starting treatment with a
statin); surgery (increased risk of acute renal
impairment, which increases the likelihood of myopathy
and rhabdomyolysis).
History of liver disease, or high alcohol intake (monitor liver
function at initiation of treatment, after 4 to 12 weeks
and periodically thereafter, e.g., at 6-month intervals or
when clinically indicated; discontinue if serum
transaminase concentration rises to, and persists at, 3
times the upper limit of the reference range); renal
impairment).
Elderly (increased risk of myopathy); Children (safety and
efficacy have not been established in children <10
years).
Adverse Drug Reactions:
Common: Abdominal pain, atrial fibrillation, constipation,
diabetes mellitus, dizziness, eczema, edema, elevated
CK and serum transaminase level, flatulence, gastritis,
headache, insomnia, myalgia, nausea, upper respiratory
infection, urinary tract infection, vertigo, vomiting
Less Common: Mild GI symptoms
Rare: Anaphylaxis, anemia, angioedema, gynecomastia,
hepatitis, hypersensitivity, impotence, interstitial lung
disease, jaundice, liver failure, myopathy, pancreatitis,
peripheral neuropathy, pruritus, rash, renal failure,
rhabdomyolysis, toxic epidermal necrolysis
Drug Interactions:
Monitor closely with:
Reduces therapeutic effect of Simvastatin:
Carbamazepine
Avoid concomitant use with:
Increases risk of adverse or toxic effects of simvastatin:
Clotrimazole (myopathy), CYP3A4 Inhibitors, e.g.,
Clarithromycin, Erythromycin, Ketoconazole, Diltiazem
(myopathy; rhabdomyolysis)
Increases serum concentration of the following drugs:
CYP3A4 Inhibitors, e.g., Clarithromycin, Erythromycin,
Ketoconazole, Diltiazem
Reduces absorption of simvastatin:
Bile Acid Binding Resins [administer statin at least 1 hour
before, or 4 hours after, the resin]
Administration: May be taken with or without food.
Avoid excessive consumption, i.e., >1 L daily of grapefruit
juice.
Pregnancy Category: X
ATC Code: C10AA01](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-194-320.jpg)














![G
GENITO URINARY SYSTEM AND SEX HORMONES
167
GENITO URINARY SYSTEM
AND SEX HORMONES
ANTIINFECTIVES AND ANTISEPTICS,
EXCLUDING COMBINATIONS WITH
CORTICOSTEROIDS
Rx NYSTATIN
Vaginal: 100,000 units per tablet
A polyene antifungal obtained from Streptomyces noursei
that interfere with the permeability of cell membrane of
fungi, particularly Candida.
Indications: Used in the prophylaxis and treatment of
infections caused by Candida, including vulvovaginal
candidiasis
NOTE: Diagnosis should be confirmed by KOH smears
and/or cultures prior to treatment. Some pathogens that
are also commonly associated with vulvovaginitis like
Trichomonas and Haemophilus vaginalis should be ruled
out through adequate laboratory procedures.
Dose:
Vaginal candidiasis, by vaginal insertion, ADULT, 100,000–
200,000 units daily for 14 days or longer.
NOTE: For cutaneous lesions, ointment, gel, cream, or
dusting powder having 100,000 units per gram can be
applied 2 to 4 times daily.
Precautions:
Intravaginal preparations may damage latex contraceptives
(an additional contraceptive method is recommended
during treatment);
Pregnancy (check first with a health care professional if
pregnant or trying to get pregnant).
Adverse Drug Reactions:
Contact dermatitis, ashes, including urticaria, irritation,
sensitization, generalized pustular eruptions
Drug Interactions:
Monitor closely with:
Increases risk of adverse or toxic effects:
Other vaginal products [consult health care professional]
Avoid concomitant use with:
Increases risk of adverse or toxic effects of Progesterone
(Intravaginal gel) (alters progesterone release)
Administration: For use in the vagina only. Do NOT take by
mouth.
Wash hands first before and after use. Insert 1 tablet in the
applicator tip. Lie on the back then gently insert
applicator high in the vagina and push plunger to release
the tablet. Gently remove the applicator. Wash it well with
warm water and soap.
Follow course of medication. Do NOT use in amounts other
than what is directed.
Pregnancy Category: A
ATC Code: G01AA01
OTHER GYNECOLOGICALS
UTEROTONICS
ERGOT ALKALOIDS
Rx
METHYLERGOMETRINE
(METHYLERGONOVINE)
Inj.: 200 micrograms/mL (as hydrogen maleate or
maleate), 1 mL ampule (IM, IV)
Methylergometrine is an amine ergot alkaloid that increases
tone, rate, and amplitude of contractions on the smooth
muscles of the uterus.
Indications: For management of third stage labor; routine
management after delivery of the placenta;
management of postpartum hemorrhage, uterine
subinvolution, and postpartum atony
Contraindications: Hypertension; toxemia; pregnancy or
patients with threatened spontaneous abortion
Dose:
Management of postpartum hemorrhage, by IM or IV
injection, ADULT, 0.2 mg after delivery of anterior
shoulder, after delivery of placenta, or during
puerperium, may be repeated every 24 hours as needed.
Management of postpartum hemorrhage, severe
hemorrhage, by IM or IV injection, ADULT, 0.2 mg after
delivery of anterior shoulder, after delivery of placenta,
or during puerperium, may be repeated as required at 2-
to 4-hour intervals.
NOTE: IV administration must only be considered during life-
threatening situations due to the possibility of inducing
sudden hypertension and cerebrovascular incident.
Dose Adjustment:
Renal and Hepatic Impairment:
Use with caution.
Precautions:
WARNING: Do NOT exceed dosing guidelines and
avoid prolonged administration. Ergot alkaloids
use may result in ergotism or intense
vasoconstriction resulting in peripheral vascular
ischemia and possible gangrene, usually
associated with overdose or prolonged chronic use.
Coronary heart disease; Hypertension; Heart disease;
Venoatrial shunts;
Mitral valve stenosis;
Sepsis;
Obliterative vascular disease;
Ergotism;](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-211-320.jpg)
![G
GENITO URINARY SYSTEM AND SEX HORMONES
168
Pleural and/or retroperitoneal fibrosis;
Hepatic and renal impairment;
Pregnancy (use with caution in women in second stage of
labor).
Adverse Drug Reactions: Acute MI, angina pectoris, arterial
spasm, atrioventricular block, bradycardia,
cerebrovascular accident, chest pain,
hyper/hypotension, palpitation, tachycardia, vasospasm,
ventricular fibrillation, dizziness, hallucinations,
headache, seizure, rash, water intoxication, abdominal
pain, diarrhea, foul taste, nausea, vomiting,
thrombophlebitis, leg cramps, paresthesia, tinnitus,
hematuria, dyspnea, nasal congestion, anaphylaxis, and
diaphoresis
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Methylergometrine:
Metoclopramide, Tedizolid (serotonergic effects)
Enhances therapeutic effect of Anti-emetics e.g., 5-HT3
Antagonists, Anti-psychotic Agents (dopamine blockade)
Increases risk of adverse or toxic effects of
Methylergometrine:
Anti-psychotic Agents, Tedizolid (serotonin syndrome),
CYP3A4 Inhibitors (ergotism), Metoclopramide
(serotonin syndrome; neuroleptic malignant syndrome)
Increases risk of adverse or toxic effects of the following
drugs:
Anti-emetics, e.g., 5-HT3 Antagonists (serotonin
syndrome), Anti-psychotic Agents (neuroleptic malignant
syndrome)
Avoid concomitant use with:
Enhances therapeutic effect of Methylergometrine:
Beta Blockers, Serotonin 5-HT1 Receptor Agonists
(vasoconstricting effects).
Enhances therapeutic effect of the following drugs:
Alpha / Beta Agonists, Alpha1 Agonists (hypertensive
effects), Serotonin 5-HT1 Receptor Agonists
(vasoconstricting effects)
Increases risk of adverse or toxic effects of
Methylergometrine:
Azole Antifungals, CYP3A4 Inhibitors, Dapoxetine,
Protease Inhibitors (ergotism), Serotonin Modulators
[except Tedizolid] (serotonin syndrome)
Increases serum concentration of Methylergometrine:
Anti-hepaciviral Combination Products, Boceprevir,
Fusidic Acid, Macrolide Antibiotics [except Azithromycin],
Mifepristone, Nitroglycerin
Reduces therapeutic effect of Nitroglycerin (vasodilatory
effect)
Administration: May be administered by IM or IV injection.
Limit IV use to patients with severe uterine bleeding or other
life-threatening emergency situations with doses given
over a period of not less than 1 minute. NOT for routine
IV administration due to risk of inducing sudden
hypertensive and cerebrovascular accidents. Some
clinicians recommend diluting the IV dose to a volume of
5 mL with 0.9% sodium chloride injection before
administration. Monitor blood pressure, CNS status, and
vaginal bleeding regularly.
Pregnancy Category: C
ATC Code: G02AB01
PROSTAGLANDINS
Rx CARBOPROST
Inj.: 125 micrograms/0.5 mL, 250 micrograms/mL
solution and 1 mL ampule/vial
Carboprost is a synthetic derivative of prostaglandin that
stimulates uterine smooth muscle, increasing uterine
tone.
Indication: For the treatment of post-partum hemorrhage
after failure of treatment with oxytocin therapy or if the
use of methylergometrine is contraindicated (pre-
eclampsia, hypertension, cardiovascular disease)
Contraindications: Acute pelvic inflammatory disease;
active cardiac, pulmonary, renal or hepatic disease
Dose:
NOTE: Ask clinician regarding the need for additional doses
and adequate dosing interval based on clinical events of
the patient.
Post-partum hemorrhage, by deep IM injection, ADULT, 250
micrograms/mL, then repeat every 15–90 minutes, if
needed (maximum total dose, 2 mg or 8 doses).
Dose Adjustment:
Renal and Hepatic Impairment:
Use with caution.
Precautions:
WARNING: A potent oxytocic agent. Strictly adhere to
recommended dosing. Use should only be under
the direct supervision of medically trained
personnel in a hospital that can immediately
provide intensive care unit and surgical facilities.
Glaucoma or raised intraocular pressure;
Asthma;
Hypertension, Hypotension, or any cardiovascular disease;
Anemia;
Jaundice;
Hepatic and renal impairment;
Diabetes;
Epilepsy
Adverse Drug Reactions:
Common: Diarrhea, nausea, vomiting, increase in body
temperature, flushing/hot flashes, chills, endometritis,
uterine hemorrhage, retained placenta or membranes,
headaches, cough](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-212-320.jpg)


![G
GENITO URINARY SYSTEM AND SEX HORMONES
171
undiagnosed vaginal bleeding; history of pruritus during
pregnancy, chorea, deteriorating otosclerosis,
cholestatic jaundice, or pemphigoid gestationis; after
evacuation of hydatidiform mole; smokers >35 years
Dose:
ADMINISTRATION. Each tablet (“pill”) should be taken at
approximately the same time each day. If one or more
tablets are forgotten for more than 12 hours,
contraceptive protection will be reduced.
For Schedule 1:
Sunday
Starter
Begins dose on first Sunday after onset of
menstruation. If the menstrual period
starts on a Sunday, take first tablet that
very same day. With a Sunday start, an
additional method of contraception should
be used until after the first 7 days of
consecutive administration.
21-
tablet
package
Take 1 tablet daily for 21 consecutive
days, followed by 7 days off the
medication.
Start new course on the 8th day after the
last tablet is taken.
28-
tablet
package
Take 1 tablet daily without interruption.
For Schedule 2:
Day 1
Starter
Take 1 tablet daily starting on the first day
of the menstrual cycle.
21-
tablet
package
Take 1 tablet daily for 21 consecutive
days, followed by 7 days off the
medication (during which withdrawal
bleeding occurs).
Start new course on the 8th day after the
last tablet is taken.
28-
tablet
package
Take 1 tablet daily without interruption
(withdrawal bleeding occurs when inactive
tablets are being taken).
NOTE: If all doses have not been taken on schedule and one
menstrual period is missed, the possibility of pregnancy
should be considered. If 2 consecutive menstrual
periods are missed, pregnancy test is required before
starting a new dosing cycle.
MISSED PILL. The critical time for loss of contraception
protection is when a pill is omitted either at the beginning
or at the end of a cycle (as this lengthens the pill free
interval). If a woman forgets to take a pill, she should
take it as soon as she remembers, and take the next one
at the normal time. If the delay with any pill is 24 hours
or longer, the pill may not work. Continue taking the pill
normally but be aware that contraception may not work
for the next 7 days. If these 7 days run beyond the end
of the packet, the next packet should be started at once,
omitting the 7 inactive tablets or the pill-free interval.
Emergency contraception is recommended if more than
2 combined oral contraceptive tablets are missed from
the first 7 tablets in a packet.
DIARRHEA AND VOMITING. Vomiting within 2 hours of taking
an oral contraceptive or very severe diarrhea can
interfere with the absorption of the drug. Additional
precautions should be used during, and for 7 days after,
recovery. If vomiting and diarrhea occur during the last 7
pills, omit inactive pills or next pill-free period.
Dose Adjustment:
Renal Impairment
In mild-to-moderate impairment, use with caution.
In severe impairment, refer patient to a specialist.
Precautions:
WARNING: Increased risk of cardiovascular side
effects in women who smoke cigarettes
(especially heavy smokers with ≥15 cigarettes
per day). Strongly advise women who use
combination hormonal contraceptives to stop
use of oral contraceptives or not to smoke.
Unexplained vaginal bleeding (investigate cause before
starting contraceptive);
Risk factors for venous thromboembolism and arterial
disease;
Migraine without focal aura or controlled with 5HT1 agonist;
Hyperprolactinemia;
Gallbladder disease;
Some types of hyperlipidemia;
History of severe depression especially if induced by
hormonal contraception;
Long-term immobilization [see Travel below];
Sickle-cell disease;
Inflammatory bowel disease, including Crohn’s disease;
Diabetes;
Smoking;
BMI >30;
Malabsorption syndromes;
Surgery;
Systemic Lupus Erythematosus (SLE);
Pregnancy (epidemiological evidence suggests no harmful
effects on fetus; use within 3 weeks of birth);
Breastfeeding (combined oral contraceptives may inhibit
lactation; use alternative method of contraception until
weaning or for 6 months after birth).
MIGRAINE. Report any increase in headache frequency or
onset of focal symptoms. Discontinue immediately and
refer urgently to a neurologist if focal neurological
symptoms not typical of aura persist for more than 1
hour.
TRAVEL. Women may be at an increased risk of deep-vein
thrombosis during travel involving long periods of
immobility (over 5 hours). The risk may be reduced by
appropriate exercise during the journey, and possibly by
wearing elastic hosiery.
Adverse Drug Reactions:
Common: Acne, breakthrough bleeding, breast enlargement
and tenderness, changes in libido, chloasma, fluid
retention, headache, hypertension, mood changes (e.g.,
depression), nausea, thrush, vomiting
Less Common: Alopecia, amenorrhea, contact lens
intolerance, hirsutism, hyperinsulinemia, insulin
resistance, rash
Rare: Allergy, breast cancer, cervical cancer, hypertension,
jaundice, liver cancer, pancreatitis, photosensitivity,
stroke, VTE](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-215-320.jpg)
![G
GENITO URINARY SYSTEM AND SEX HORMONES
172
Drug Interactions:
NOTE: Combined oral contraceptives are metabolized by
CYP3A4.
Monitor closely with:
Enhances therapeutic effect of Fixed Combinations of
Progestins and Estrogens:
NSAIDs including COX-2 Inhibitors (thrombogenic effect)
Enhances therapeutic effect of Immune Globulin
(thrombogenic effect)
Reduces contraceptive effect of Fixed Combinations of
Progestins and Estrogens:
Cephalosporins e.g. Ceftriaxone, Macrolide Antibiotics
e.g., Azithromycin, Erythromycin, Metronidazole,
Penicillins e.g., Benzylpenicillin, Amoxicillin,
Phenoxymethylpenicillin, Ampicillin, Quinolones e.g.,
Ciprofloxacin, Levofloxacin, Tetracyclines e.g.
Doxycycline
Reduces therapeutic effect of the following drugs:
Anti-diabetic Agents, Thyroid Products
Avoid concomitant use with:
Decreases serum concentration of Fixed Combinations of
Progestins and Estrogens:
Bile Acid Sequestrants [administer oral contraceptives at
least 1-4 hours prior to or 4-6 hours after a Bile Acid
Sequestrant], Dabrafenib, Efavirenz, Exemestane,
Griseofulvin, Lamotrigine, Topiramate
Enhances therapeutic effect of Tranexamic Acid
(thrombogenic effect)
Increases metabolism of Fixed Combinations of Progestins
and Estrogens:
Carbamazepine, CYP2C19 Inducers, CYP3A4 Inducers,
Phenobarbital, Rifampicin
Increases risk of adverse or toxic effects of the following
drugs:
Anti-hepaciviral Combination Products (hepatotoxic
effect), Vitamin K Antagonists, e.g., Warfarin
(thromboembolic disorders)
Reduces therapeutic effect of Fixed Combinations of
Progestins and Estrogens, leading to contraceptive
failure:
Artemether, Barbiturates e.g. Phenobarbital,
Carbamazepine, CYP2C19 Inducers, CYP3A4 Inducers,
Fosphenytoin, Mifepristone, Mycophenolate,
Phenobarbital, Phenytoin, Protease Inhibitor [except
Indinavir], Retinoic Acid Derivatives [except Adapalene,
Tretinoin (topical)], Rifamycin Derivatives, Rifampicin
Reduces therapeutic effect of the following drugs:
Amlodipine, Enalapril, Isosorbide Dinitrate, Methyldopa
(antagonizes hypotensive effect), Anastrozole, Anti-
coagulants e.g. Warfarin, Heparin (counteracts
anticoagulant effects), Furosemide, Hyaluronidase,
Hydrochlorothiazide (antagonizes diuretic effect),
Metformin (antagonizes hypoglycemic effect)
Rx
ETHINYLESTRADIOL +
DESOGESTREL
Oral: 30 micrograms ethinylestradiol + 150 micrograms
desogestrel per tablet as 21 active tablets or 28-day
tablet with 21 active and 7 inactive pills
A combined oral contraceptive, which contains estrogen as
ethinylestradiol, and progesterone as desogestrel. It
inhibits ovulation, reduces receptivity of the
endometrium for implantation, and thickens cervical
mucus that serves as a barrier to sperm.
Indication: Contraception
Dose:
Contraception, by mouth, ADULT (female), 1 tablet (30
micrograms ethinylestradiol + 150 micrograms
desogestrel) daily for 21 days, followed by 7 days of
inactive pills.
Administration: Administer at the same time each day at
intervals not more than 24 hours. If 1 or more tablets are
forgotten for more than 12 hours, contraceptive
protection will be reduced.
Take 1 tab daily starting the 1st pack on the 1st day of
menstruation, without interruption for 22 days, followed
by 6 tab-free days. Start with the blue tablets and follow
the directional arrows on the pack. For missed doses,
take as soon as remembered. If remembered >12 hours
than intended, risk of becoming pregnant increases.
See General Information on Progestins and Estrogens,
Fixed Combinations listed above for further information.
Pregnancy Category: X
ATC Code: G03AA09
Rx
ETHINYLESTRADIOL +
LEVONORGESTREL
Oral: 30 micrograms ethinylestradiol + 150 micrograms
levonorgestrel per tablet as 21 active tablets or 28-
day tablet with 21 active and 7 inactive pills
A combined, oral contraceptive, which contains estrogen as
ethinylestradiol and progesterone as levonorgestrel. It
inhibits ovulation, reduces receptivity of the
endometrium for implantation, and thickens cervical
mucus that serves as a barrier to sperm.
Indication: Contraception
Dose:
Contraception, by mouth, 1 tablet daily for 21 days starting
on day 1 of the menstrual cycle; repeat subsequent
courses after a 7-day tablet-free interval (during which
withdrawal bleeding occurs); or
28 tablets of everyday (ED) preparations, take 1 active
tablet daily starting on D1 of the cycle up to D21; repeat
subsequent courses without interval (withdrawal
bleeding occurs when inactive tablets are being taken).](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-216-320.jpg)
![G
GENITO URINARY SYSTEM AND SEX HORMONES
174
Remove no later than the end of the third year. This can be
replaced with a new implant at time of removal if
continued contraception is needed, after ruling out
possibility of pregnancy. Insertion can be done as
follows:
No hormonal
contraceptives
within past month
Insert between days 1 through 5 of
menstruation, even if still bleeding
Switching from
combination
hormonal
contraceptive
Transdermal system or vaginal ring
Insert on the day of the removal of the
transdermal system or vaginal ring or on
the day following the transdermal-free or
ring-free interval
Switching from a
progestin-only
contraceptive
Implant or intrauterine device (IUD)
Insert on same day as removal of implant
or IUD
Injection
Insert on day next injection is due
First trimester
abortion or
miscarriage
Insert within first 5 days following first
trimester abortion or miscarriage.
Second trimester
abortion or
miscarriage
Insert between 21 and 28 days following
second trimester abortion or miscarriage.
Postpartum
If not breast-feeding, insert between 21 to
28 days postpartum.
If breast-feeding, insert after the fourth
post-partum week and use a second non-
hormonal form of contraception for the
first 7 days of insertion.
Precautions:
Breast cancer;
Carbohydrate intolerance and diabetes;
Ovarian cysts;
Retinal vascular thrombosis (discontinue if there is loss of
vision, proptosis, diplopia, papilledema, or retinal
vascular lesions);
Thromboembolism and other vascular events (e.g., deep
vein thrombosis, myocardial infarction, pulmonary
embolism);
Changes in vaginal bleeding;
Cardiovascular diseases;
Depression;
Disease that may be exacerbated by fluid retention;
Gallbladder disease;
Hepatic adenomas or carcinomas;
Hepatic impairment;
Hyperlipidemia;
Hypertension;
Renal impairment;
Overweight women;
Wearers of contact lens;
Increased risk of cervical or ovarian cancer;
May change results of some laboratory tests (e.g.,
coagulation factors, lipids, glucose tolerance, binding
proteins);
Does not protect against HIV infection or other sexually
transmitted disease
Adverse Drug Reactions:
Common: Headache, acne vulgaris, menstrual disease (<3
episodes or 90 days; prolonged menstrual bleeding
lasting >14 days: >5 episodes in 90 days) amenorrhea
(no bleeding in 90 days); weight gain, abdominal pain,
vaginitis, mastalgia, pharyngitis
Less Common: Dizziness, emotional lability, depression,
nervousness, pain, localized erythema, dysmenorrhea,
nausea, leukorrhea, hypersensitivity, application site
reaction, local pain, hematoma at injection site, bruising
at injection site, back pain, flu-like symptoms
Rare: Alopecia, angioedema (including exacerbation of
hereditary angioedema), cerebrovascular accident,
anaphylaxis, convulsions, migraine, hypertension,
myocardial infarction, ovarian cyst, pulmonary embolism,
seizure
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of C1 Inhibitors (thrombogenic
effect)
Reduces therapeutic effect of Antidiabetic Agents
Avoid concomitant use with drugs that
Decrease serum concentration of Etonogestrel:
Acitretin, Aprepitant, Artemether, Bile Acid Sequestrants
[administer Etonogestrel at least 1–4 hours prior to or
4–6 hours after Bile Acid Sequestrants], Bosentan,
Carbamazepine, Dabrafenib, Exenatide, Lixisenatide
[administer Etonogestrel 1 hour before or 11 hours after
Lixisenatide], Lumacaftor, Mycophenolate, Nelfinavir,
Nevirapine, Oxcarbazepine, Perampanel, Prucalopride,
Rifamycin Derivatives, Saquinavir, Sugammadex,
Telaprevir, Topiramate
Enhance therapeutic effect of Etonogestrel:
Tranexamic Acid (thrombogenic effect)
Increase risk of adverse or toxic effects of Vitamin K
Antagonists e.g. Warfarin (thromboembolic disorders)
Increases serum concentration of Etonogestrel:
Atazanavir
Reduces therapeutic effect of Etonogestrel, leading to
contraceptive failure:
Barbiturates, Efavirenz, Fosphenytoin, Griseofulvin,
Mifepristone, Phenytoin, Retinoic Acid Derivatives
[except Adapalene, Tretinoin (topical)], Ulipristal [for
uterine fibroids, avoid Etonogestrel within 12 days of
stopping Ulipristal; for emergency contraceptive, avoid
Etonogestrel within 5 days of stopping Ulipristal]
Reduces therapeutic effect of Anticoagulants, Vitamin K
Antagonists e.g. Warfarin (anticoagulant effect)
Administration: Insert implant subdermally at the inner side
of the non-dominant upper arm approximately 8–10 cm
(3–4 inches) above the medial epicondyle of the
humerus just under the skin. Implant must be palpable
after insertion.
X-ray, CT scan, ultrasound scanning, or MRI can be used to
confirm the location of the implant if it is not palpable.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-218-320.jpg)



![G
GENITO URINARY SYSTEM AND SEX HORMONES
178
Increases risk of adverse or toxic effects of Dantrolene
(hepatotoxic effect)
Reduces therapeutic effect of Conjugated Estrogen:
Tocilizumab
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Thyroid Products
Avoid concomitant use with:
Decreases serum concentration of Conjugated Estrogen:
Dabrafenib, Enzalutamide
Increases metabolism of Conjugated Estrogen:
CYP1A2 Inducers, CYP3A4 Inducers
Increases serum concentration of Tizanidine
Reduces therapeutic effect of the following drugs:
Anastrozole, Anticoagulants, Exemestane,
Hyaluronidase, Somatropin
Administration: May be taken without regard to meals. Use
alone or in combination with progestin with the lowest
effective dose and for the shortest duration possible.
Consider adding progestin when prescribing estrogen for a
postmenopausal woman with a uterus to reduce the risk
of endometrial cancer.
NOTE: Women without uterus do not need progestin,
however, hysterectomized women with a history of
endometriosis may need progestin.
Pregnancy Category: X
ATC Code: G03CA57
PROGESTINS
General Information
Progestins are synthetic forms of progesterone that
suppresses ovulation, thickens cervical mucus, alters
follicle stimulating hormone (FSH) and luteinizing
hormone (LH) concentrations, slows the movement of
ovum through the fallopian tubes, and alters the
endometrium.
Contraindications: Breast cancer or other estrogen- or
progestin-dependent neoplasms (current or a history of);
hepatic tumors or disease; thrombosis or
thromboembolic disorders (current or history of);
undiagnosed abnormal genital bleeding
Precautions:
Warning: Do NOT use for prophylaxis of dementia. An
increased incidence of dementia was observed in
women ≥65 years of age taking conjugated
estrogens alone or in combination with
medroxyprogesterone acetate.
Do NOT use in the prevention of cardiovascular
disease. An increased risk of deep vein
thrombosis, stroke, pulmonary emboli, and
myocardial infarction was observed in conjugated
estrogens with medroxyprogesterone acetate in
postmenopausal women.
An increased risk of invasive breast cancer was
observed in postmenopausal women using
conjugated estrogens in combination with
medroxyprogesterone acetate. An increase in
abnormal mammogram findings has also been
observed with estrogen alone or in combination
with progestin therapy. Treatment may also lead to
severe hypercalcemia in patients with breast
cancer and bone metastases. Use is
contraindicated in patients with known or
suspected breast cancer.
Breast, cervical or ovarian cancer; Ovarian cysts;
Retinal vascular thrombosis (discontinue if there is loss of
vision, proptosis, diplopia, papilledema, or retinal
vascular lesions);
Transient dizziness or drowsiness;
Cardiovascular diseases;
Depression;
Disease that may be exacerbated by fluid retention;
Thromboembolism and other vascular events, e.g., DVT, MI,
PE;
Hypertension;
Changes in vaginal bleeding;
Carbohydrate intolerance and diabetes;
Gallbladder disease;
Hepatic tumor;
Hepatic impairment;
Hyperlipidemia;
Renal impairment;
Porphyria;
Does not protect against HIV infection or other sexually
transmitted disease;
Laboratory tests (may alter results, e.g., coagulation factors,
lipids, glucose tolerance, binding proteins);
Overweight women;
Wearers of contact lens
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of C1 Inhibitors (thrombogenic
effect)
Reduces therapeutic effect of Antidiabetic Agents
Avoid concomitant use with:
Decreases serum concentration of Progestins:
Acitretin, Aprepitant, Artemether, Bile Acid Sequestrants
[administer oral progestin-containing contraceptives at
least 1-4 hours prior to or 4-6 hours after Bile Acid
Sequestrants], Bosentan, Carbamazepine, Clobazam,
Dabrafenib, Darunavir, Exenatide, Felbamate,
Fosaprepitant, Lixisenatide [administer oral
contraceptives 1 hour before or at least 11 hours after
Lixisenatide], Lumacaftor, Mycophenolate, Nelfinavir,
Nevirapine, Oxcarbazepine, Prucalopride, Rifamycin
Derivatives, Saquinavir, Sugammadex, Telaprevir,
Topiramate](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-222-320.jpg)
![G
GENITO URINARY SYSTEM AND SEX HORMONES
179
Enhances therapeutic effect of Progestins:
Tranexamic Acid (thrombogenic effect)
Increases risk of adverse or toxic effects of Vitamin K
Antagonists e.g. Warfarin (thromboembolic disorders)
Reduces therapeutic effect of Progestins, leading to
contraceptive failure:
Barbiturates, Fosphenytoin, Griseofulvin, Mifepristone,
Phenytoin, Retinoic Acid Derivatives [except Adapalene,
Topical Bexarotene, Tretinoin (Topical)], Ulipristal [avoid
Progestins within 5 days of stopping Ulipristal]
Reduces therapeutic effect of the following drugs:
Anticoagulants, Vitamin K Antagonists e.g. Warfarin
(anticoagulant effect)
Administration: Use for the shortest duration possible at the
lowest effective dose in accordance with treatment
goals.
PREGNEN (4) DERIVATIVES
Rx MEDROXYPROGESTERONE
Oral: 5 mg and 10 mg tablet (as acetate)
Inj.: 50 mg/mL (as acetate), 3 mL vial + syringe (IM)
150 mg/mL (as acetate or enanthate), 1 mL vial (IM)
NOTE: Use one (1) inch long needle
Medroxyprogesterone transforms the endometrium from a
proliferative to a secretory state. If given parenterally, it
can inhibit gonadotropin production, preventing follicular
maturation and ovulation.
Indications: Prophylaxis for endometrial hyperplasia;
Management of abnormal uterine bleeding,
amenorrhea, renal cell carcinoma andendometrial
carcinoma; hormonal replacement therapy
Contraindications: Suspected or known pregnancy; hepatic
impairment or disease
Dose:
Prophylaxis for endometrial hyperplasia, by mouth, ADULT,
5–10 mg once a day, in combination with estrogen
replacement therapy beginning on day 1 or day 16 of
each cycle, continuing for 12 to 14 consecutive days per
month; or 2.5 mg once a day continuously with estrogen
replacement therapy.
Abnormal uterine bleeding, by IM injection, ADULT and
ADOLESCENT, 5–10 mg once a day starting on the 16th
day of the cycle and continue for 10 days; or begin on the
21st day of the cycle and continue for 5 days (withdrawal
bleeding usually occurs within 3–7 days after the
discontinuation).
Amenorrhea, by IM injection, ADULT and ADOLESCENT, 5–
10 mg once a day starting at any time and continuing for
5–10 days (withdrawal bleeding usually occurs within 3–
7 days after the discontinuation).
Renal cell carcinoma and endometrial carcinoma, by IM
injection, ADULT, 400–1,000 mg once a week; can be
reduced to 400 mg once a month; frequency of
administration can be reduced if improvement or
stabilization occurs.
Administration: Shake injectable suspension immediately
prior to use. Administer IM injection deeply into gluteal,
deltoid or anterior thigh muscle.
See Medroxyprogesterone under Hormonal Contraceptives
for Systemic Use for other information.
Pregnancy Category: X
ATC Code: G03DA02
PREGNADIEN DERIVATIVES
Rx DYDROGESTERONE
Oral: 10 mg tablet
A synthetic retroisomer of progesterone that lacks
androgenic, estrogenic, thermogenic, corticoid, and
anabolic properties. It induces secretory changes in the
endometrium.
Indications: Abnormal uterine bleeding; secondary
amenorrhea; dysmenorrhea; endometriosis; infertility;
irregular menstrual cycle; menopause; recurrent and
threated pregnancy loss; premenstrual syndrome;
severe hepatic impairment
Dose:
Abnormal uterine bleeding, by mouth, ADULT, 10 mg twice
daily for 5-7 days to stop bleeding. Then continue to 10
mg twice daily on days 11–25 of cycle for prevention.
Amenorrhea, secondary, by mouth, ADULT, 10 mg twice
daily on days 11–25 of cycle. [NOTE: Prime endometrium with
adequate estrogen, exogenous or endogenous, prior to
administration. A dose of 10 mg once daily for 14 consecutive days
of each 28-day cycle has shown efficacy in premenopausal women
with normal estrogen levels.]
Dysmenorrhea, by mouth, ADULT, 10 mg twice daily on days
5–25 of cycle.
Endometriosis, by mouth, ADULT, 10 mg 2 or 3 times daily
on days 5–25 of cycle, or continuously.
Infertility due to luteal insufficiency, by mouth, ADULT, 10
mg once daily on days 14–25 of cycle for ≥6 consecutive
cycles.
Irregular menstrual cycle, by mouth, ADULT, 10 mg twice
daily on days 11–25 of cycle.
Menopause, by mouth, ADULT, in combination with cyclic
estrogen therapy, 10 mg once daily for the last 12–14
days of cycle, may increase to 10 mg twice daily if
evidence of lack of response or withdrawal bleeding
occurs; in combination with continuous estrogen
therapy, 10 mg once daily for 14 consecutive days of a
28-day cycle.
Pregnancy loss, recurrent, by mouth, ADULT, 10 mg twice
daily; may be taken through week 20 of pregnancy.
Pregnancy loss, threatened, by mouth, ADULT, 40 mg
loading dose, followed by 10 mg every 8 hours until
symptoms resolve; or 10 mg twice daily, with or without
40 mg loading dose.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-223-320.jpg)

![G
GENITO URINARY SYSTEM AND SEX HORMONES
181
every 2 weeks until reaching 15 mg daily, continue for 6–
9 months or until presence of breakthrough bleeding.
Contraception, by mouth, ADULT, 350 micrograms once
daily; start on the first day of menstruation or after
miscarriage or abortion; if switching from a combined
oral contraceptive, begin on the day after finishing the
last active pill if the patient is not pregnant; if switching
from an UID, continue this or abstain or use an
alternative emergency contraceptive for at least 2 days
after contraceptive is initiated; in case of missed dose,
take as soon as remembered; if ≥3 hours late, use a
backup method of contraception for 48 hours. [NOTE:
Back up contraception is needed if therapy is initiated within 5
days of onset of menstruation. If started >5 days or at any time
women experienced amenorrhea, back up contraception should
be used for 2 days.]
Adverse Drug Reactions: Cerebral embolism, cerebral
thrombosis, deep vein thrombosis, edema, pulmonary
embolism, retinal thrombosis, depression, dizziness,
fatigue, headache, insomnia, migraine, emotional
lability, nervousness, acne vulgaris, alopecia, chloasma,
pruritus, skin rash, urticarial, amenorrhea, hirsutism,
hypermenorrhea, menstrual disease, weight gain,
abdominal pain, nausea, vomiting, breakthrough
bleeding, breast hypertrophy, breast tenderness, cervical
erosion, change in cervical secretions, decreased
lactation, genital discharge, mastalgia, spotting, vaginal
hemorrhage, hypersensitivity, cholestatic jaundice,
hepatitis, arm pain, leg pain, optic neuritis (with or
without vision loss)
Drug Interactions: No information found
Administration: Administer tablets at the same time each
day. NOT used for emergency contraception.
Pregnancy Category: X
ATC Code: G03DC02
GONADOTROPINS AND OTHER
OVULATION STIMULANTS
OVULATION STIMULANTS, SYNTHETIC
Rx CLOMIFENE
Oral: 50 mg tablet (as citrate)
A racemic mixture that acts at the level of the hypothalamus,
occupying the cell surface and intracellular estrogen
receptors (ERs) for longer durations than estrogen. It
inhibits receptor recycling, depletes hypothalamic ERs,
and prevents normal estrogenic negative feedback.
Inhibition of the feedback signal results in increased
pulsatile secretion of GnRH from the hypothalamus and
release of pituitary gonadotropins (FSH, LH) causing
growth of the ovarian follicle, followed by follicular
rupture.
Indications: Treatment of anovulatory infertility and male
infertility due to oligospermia
Contraindications: Hepatic disease or history of hepatic
impairment; abnormal uterine bleeding; enlargement or
development of ovarian cyst not due to polycystic ovarian
syndrome; uncontrolled thyroid or adrenal dysfunction;
presence of an organic intracranial lesion such as
pituitary tumor; pregnancy
Dose:
NOTE: Schedule intercourse to coincide with the expected
time of ovulation, usually 5–10 days after taking
Clomifene.
Ovulation induction, by mouth, ADULT (female), 50 mg once
a day for 5 days. Begin on or about the fifth day of cycle
if progestin-induced bleeding is expected or
spontaneous uterine bleeding occurs before starting
therapy. Therapy can be started anytime if there is no
recent uterine bleeding. Subsequent doses may be
increased to 100 mg once daily for 5 days only if
ovulation does not occur at the initial dose. Maximum
dose is 100 mg once a day for 5 days for 6 cycles (150
mg for women with PCOS). Long-term therapy of >6
cycles is not recommended; lower doses (12.5 to 25 mg
daily) can be used in women sensitive to clomiphene or
who consistently develop large ovarian cysts.
NOTE: May repeat 5-day cycle if needed as early as 30 days
after the previous therapy, ruling out the possibility of
pregnancy and using the lowest effective dose.
Discontinue treatment if ovulation does not occur after 3
courses of treatment; or if 3 ovulatory responses already
occurred but pregnancy is still not achieved.
Precautions:
Ovarian enlargement (generally regresses after stopping
treatment);
Visual disturbances;
Ovarian hyperstimulation syndrome;
Ascitic, pleural or pericardial fluids can be removed if
necessary to lessen symptoms (women with OHSS
should avoid pelvic examination and/or intercourse);
Borderline or invasive ovarian cancer;
Polycystic ovarian syndrome;
Patients unusually sensitive to pituitary gonadotropins;
Uterine fibroids
Adverse Drug Reactions:
Common: Ovarian enlargement
Less Common: Headache, hot flashes, breast discomfort,
abnormal uterine bleeding, distention,
bloating/discomfort, nausea, vomiting, visual symptoms
including blurred vision, diplopia, floaters, lights,
phosphenes, photophobia, scotomata, waves
Rare: Acute abdomen, alopecia, appetite increased,
constipation, depression, dermatitis, diarrhea, dizziness,
dry hair, fatigue, insomnia, lightheadedness,
nervousness, rash, urinary frequency/volume increased,
vaginal dryness, vertigo, weight gain or loss
Administration: Total daily dose should only be taken one at
a time to maximize effectiveness.
Pregnancy Category: X
ATC Code: G03GB02](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-225-320.jpg)

![G
GENITO URINARY SYSTEM AND SEX HORMONES
183
Avoid concomitant use with:
Decreases metabolism of Cyproterone:
CYP3A4 Inhibitors
Decreases serum concentration of Cyproterone:
CYP3A4 Inducers, Dabrafenib
Increases serum concentration of Cyproterone:
Mifepristone
Increases serum concentration of the following drugs:
Amodiaquine, HMG-CoA Reductase Inhibitors [except
Pitavastatin, Pravastatin, Rosuvastatin]
Reduces therapeutic effect of Cyproterone:
Ulipristal [for uterine fibroids, avoid progestins within 12
days of stopping ulipristal; for emergency contraception,
avoid progestins within 5 days of stopping ulipristal]
Reduces therapeutic effect of Anticoagulants
Administration:
For oral administration, take tablets at the same time each
day, after meals and with liquids. May be divided into
equal halves to facilitate swallowing.
For IM injection, administer slowly. Avoid IV injection to
prevent pulmonary microembolism.
Pregnancy Category: X
ATC Code: G03HA01
OTHER SEX HORMONES AND MODULATORS OF THE
GENITAL SYSTEM
Rx DANAZOL
Oral: 200 mg capsule
A synthetic derivative of ethisterone with weak androgenic
and anabolic properties. It suppresses pituitary output of
FSH and LH resulting to the regression and atrophy of
normal and ectopic endometrial tissues.
Indications: Treatment of endometriosis, fibrocystic breast
diseases, and hereditary angioedema
Contraindications: Undiagnosed genital bleeding;
pregnancy; breastfeeding; porphyria; markedly impaired
hepatic, renal, or cardiac function; androgen-dependent
tumor; thrombosis or thromboembolic disease (active or
history)
Dose:
Endometriosis, by mouth, ADULT (female),
mild disease, 200–400 mg daily;
moderate-to-severe, 800 mg daily in 2 divided doses;
continue therapy uninterrupted for 3–6 months up to 9
months.
Fibrocystic breast disease, by mouth, ADULT (female), 100–
400 mg daily in 2 divided doses; pain and tenderness
may be eliminated in 2–3 months; elimination of
nodularity may require therapy for 4–6 months.
Hereditary angioedema, by mouth, ADULT, 200 mg 2 to 3
times daily; after favorable response, decrease the
dosage to ≤100 mg at 1–3 months interval or longer if
needed; if an attack occurs, increase dose by up to 200
mg daily.
Precautions:
WARNING: Thromboembolism, thrombotic, and
thrombophlebitic events, including sagittal sinus
thrombosis and life-threatening or fatal strokes,
have been reported.
Peliosis hepatis and benign hepatic adenoma have
been reported with long-term use of the drug.
Has been associated with pseudomotor cerebri, a
case of benign intracranial hypertension.
Androgenic effects;
Blood lipid changes;
Diabetes;
Edematous condition;
Fibrocystic disease;
Porphyria;
Pregnancy (if patient becomes pregnant during treatment,
discontinue the drug, and appraise patient on the
potential risk to the fetus).
Adverse Drug Reactions:
Common and Less Common: Edema, flushing,
hypertension, MI, palpitation, tachycardia, depression,
dizziness, emotional lability, fainting, fatigue, headache,
nervousness, sleep disorders, Acne, alopecia, mild
hirsutism, maculopapular rash, papular rash, petechial
rash, pruritus, purpuric rash, seborrhea, urticaria,
vesicular rash, amenorrhea (may continue post therapy),
breast size reduction, glucose intolerance or glucagon
changes, libido changes, menstrual disturbances
(spotting, altered timing of cycle), semen abnormalities
(changes in volume, viscosity, sperm count or motility),
sex hormone and thyroid binding globulin changes,
constipation, gastroenteritis, nausea, vomiting,
spermatogenesis reduction, weight gain, vaginal
dryness, vaginal irritation, cholestatic jaundice, hepatic
adenoma, jaundice, malignant tumors (prolonged use),
peliosis, hepatis, back pain, extremity pain, joint lockup,
joint pain, joint swelling, muscle cramps, paresthesia,
spasms, neck pain, tremor, visual disturbances,
weakness, hematuria, Interstitial pneumonitis,
diaphoresis, voice change (hoarseness, sore throat,
instability, deepening of pitch), hepatotoxicity
(idiosyncratic)
Rare: Benign intracranial hypertension, anxiety, chills,
convulsions, Guillain Barré syndrome, erythema
multiforme, fever, Stevens-Johnson syndrome,
photosensitivity, clitoris hypertrophy, nipple discharge,
appetite changes, bleeding gums, pancreatitis, splenic
peliosis, pelvic pain, carpal tunnel syndrome, cataracts,
nasal congestion](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-227-320.jpg)
![G
GENITO URINARY SYSTEM AND SEX HORMONES
184
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of C1 Inhibitors (thrombogenic
effect)
Increases risk of adverse or toxic effects of Vitamin D
Analogues [except Calcipotriene] (hypercalcemic effect)
Increases risk of adverse or toxic effects of Danazol:
Corticosteroids (Dofetilide)
Reduces therapeutic effect of Antidiabetic Agents
Avoid concomitant use with:
Decreases metabolism of Carbamazepine
Enhances therapeutic effect of Vitamin K Antagonists e.g.
Warfarin (anticoagulant effect)
Increases risk of adverse or toxic effects of Cyclosporine
(hepatotoxic effect)
Increases serum concentration of the following drugs:
Cyclosporine, HMG-CoA Reductase Inhibitors [except
Fluvastatin, Pravastatin, Rosuvastatin],
Increases serum concentration of the following drugs:
Pimozide, Simvastatin
Pregnancy Category: X
ATC Code: G03XA01
UROLOGICALS
DRUGS USED IN BENIGN PROSTATIC
HYPERTROPHY (BPH)
ALPHA-ADRENOCEPTOR ANTAGONISTS
General Information
Alpha–adrenoceptor blockers act preferentially on the
receptors in the lower urinary tract resulting to relaxation
in the muscles of bladder and prostate.
Indications: Treatment of signs and symptoms of benign
prostatic hypertrophy and relief of symptoms of urinary
obstruction
Precautions:
Hypotension;
Volume depletion;
Renal impairment;
Hepatic impairment;
Patients who are receiving an antihypertensive treatment
may require dose reduction and supervision;
Monitor for an improved urine flow and for “first dose”
orthostatic hypotension, headache, or GI disturbances,
e.g., nausea, vomiting, at the beginning of therapy and
on a regular basis;
Elderly and patients undergoing cataract surgery (risk of
intraoperative floppy iris syndrome)
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Alpha-adrenoceptor
Antagonists:
Anti-hypertensives, Aprepitant, Calcium Channel
Blockers (hypotensive effect), Cimetidine, Dasatinib,
Fosaprepitant, Ivacaftor, Luliconazole, Netupitant
Enhances therapeutic effect of Alpha-adrenoceptor
Antagonists:
Nitroglycerin (hypotensive effect), Palbociclib,
Phosphodiesterase Inhibitors (hypotensive effect),
Simeprevir
Increases risk of adverse or toxic effects of Alpha-
adrenoceptor Antagonists:
Beta Blockers (orthostatic hypotension), CYP3A4
Inhibitors, e.g., Ketoconazole, Itraconazole, Ritonavir,
Dapoxetine (orthostatic hypotension), MAO Inhibitors
[except Linezolid, Tedizolid] (orthostatic hypotension)
Reduces therapeutic effect of Alpha-adrenoceptor
Antagonists:
Alpha / Beta Agonists (vasoconstricting effect),
Bosentan, CYP3A4 Inducers, Deferasirox, Siltuximab,
Toclizumab
Avoid concomitant use with:
Decreases serum concentration of Alpha-adrenoceptor
Antagonists:
CYP3A4 Inducers, Dabrafenib
Enhances therapeutic effect of Alpha-adrenoceptor
Antagonists:
Alpha1 Blockers (antihypertensive effect),
Phosphodiesterase-5 Inhibitors e.g. Sildenafil
(antihypertensive effect), Protease Inhibitors e.g.,
Indinavir, Telaprevir
Enhances therapeutic effect of QTc-prolonging Agents
(Highest Risk)
Increases risk of adverse or toxic effects of Alpha-
adrenoceptor Antagonists:
Beta Blockers [except Levobunolol, Metipranolol],
Stiripentol (orthostatic hypotension), CYP3A4 Inhibitors,
Fusidic Acid, Mifepristone (orthostatic hypotension),
Increases serum concentration of Alpha-adrenoceptor
Antagonists:
CYP3A4 Inhibitors, Fusidic Acid, Telaprevir
Reduces therapeutic effect of Alpha-adrenoceptor
Antagonists:
Dabrafenib
Rx ALFUZOSIN
Oral: 10 mg tablet (as hydrochloride)
An alpha1-selective adrenoceptor antagonist used in Benign
Prostatic Hypertrophy (BPH) to relieve symptoms of
urinary obstruction, including acute urinary retention.](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-228-320.jpg)


![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
187
SYSTEMIC HORMONAL
PREPARATIONS, EXCLUDING SEX
HORMONES AND INSULINS
PITUITARY AND HYPOTHALAMIC
HORMONES AND ANALOGUES
POSTERIOR PITUITARY LOBE HORMONES
VASOPRESSIN AND ANALOGUES
Rx DESMOPRESSIN
Oral: 100 micrograms and 200 micrograms tablet (as
acetate)
Inj.: 15 micrograms/mL (as acetate), 1 mL ampule (IM,
SC)
A synthetic analogue of the antidiuretic hormone arginine
vasopressin. It increases cAMP in renal tubular cells in a
dose dependent manner. This increases water
permeability, resulting in decreased urine volume and
increased urine osmolality, as well as increases plasma
levels of von Willebrand factor, factor VIII, and tPA
contributing to a shortened activated partial
thromboplastin time (aPTT) and bleeding time.
Indications: For the treatment of central diabetes insipidus
and primary nocturnal enuresis in children aged 5 years
and above
Contraindications: Hyponatremia (current or a history of),
CrCl <50 mL/minute), type 2B or platelet type (pseudo)
von Willebrand’s disease; habitual or psychogenic
polydipsia; cardiac insufficiency; conditions requiring
diuretic therapy (sublingual); nephrosis, severe hepatic
dysfunction (sublingual)
Dose:
Nocturnal emesis, by mouth, ADULT and CHILD ≥5 years,
initially 0.2 mg at bedtime, may be titrated up to 0.6 mg.
[NOTE: Limit fluid intake 1 hour prior to dose until the
next morning, or at least 8 hours after administration].
Diabetes insipidus, IM, SC, ADULT, 2–4 micrograms (0.5–1
mL) daily in 2 divided doses;
by mouth, ADULT and CHILD ≥4 years, 0.05 mg twice daily;
total daily dose should be increased or decreased as
needed to obtain adequate anti-diuresis (range: 0.1 to 1.2
mg 2–3 divided doses). [NOTE: Observe fluid restriction].
Age (years)
Initial Dose
(micrograms, 2-
3 times daily)
Range
(micrograms
daily)
Neonate 1 – 4 None stated
1 month -
2 years
10 30 – 150
2 – 12 50 100 – 800
12 – 18 100 200 – 1,200
Dose Adjustment:
Renal Impairment:
In CrCl <50 mL/minute, use is contraindicated.
Precautions:
Allergic reactions;
Hyponatremia;
Thrombotic events (use with caution in patients
predisposed to thrombus formation);
Von Willebrand disease type 2B; Habitual or psychogenic
polydipsia (use with caution);
Primary nocturnal enuresis (interrupt treatment if the
patient experiences an acute illness, e.g. fever,
recurrent vomiting, or diarrhea);
Vigorous exercise;
Any condition associated with increase in water
consumption;
Elderly and children.
Adverse Drug Reactions:
Common: Flushing (facial), headache, skin rash,
hyponatremia, water intoxication, abdominal cramps,
burning sensation at injection site, sore throat, erythema
or swelling at injection site, cough, nasal congestion,
upper respiratory tract infection
Less Common: Abnormality in thinking, agitation, balanitis,
chest pain, diarrhea, drowsiness, pain, coma, dyspepsia,
insomnia, edema, localized warm feeling, palpitations,
photophobia, seizure, eye pruritus, tachycardia,
vomiting, vulvar pain
Rare: Anaphylaxis, hypersensitivity reaction
Drug Interactions:
Monitor closely with:
Increases risk of adverse or toxic effects of Desmopressin:
Carbamazepine, Chlorpromazine, Chlorpropramide,
Lamotrigine, Nonsteroidal Anti-Inflammatory Agents,
Opioid Analgesics e.g., morphine, fentanyl, Selective
Serotonin Reuptake Inhibitors e.g. Fluoxetine, Sertraline,
Tricyclic Antidepressants e.g., Amitriptyline Imipramine,
Urea
Reduces therapeutic effect of Desmopressin:
Demeclocycline, Epinephrine [large doses], Ethyl Alcohol,
Heparin, Lithium
Avoid concomitant use with:
Reduces therapeutic effect of Desmopressin:
Tolvaptan
Administration: Restrict fluid intake from 1 hour before to 8
hours after taking desmopressin tablets to decrease the
possibility of water intoxication and hyponatremia.
Pregnancy Category: B
ATC Code: H01BA02](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-231-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
190
divided doses every 6 hours beginning 24 hours prior to
extubation and continuing for 4–6 doses afterwards
Antiemetic, by mouth or by IV injection, ADULT, 10 to 20 mg
15–30 minutes before treatment on each treatment day;
by IV injection, CHILD, 10 mg/m2 per dose every 12–24
hours on days of chemotherapy for severely emetogenic
chemotherapy courses.
Type of Therapy for
Adults
Route Dose
Continuous
infusion regimen
Oral or
IV
10 mg every 12
hours on each
treatment day
Mildly emetogenic
therapy
Oral, IM,
or IV
4 mg every 46
hours
Delayed nausea and vomiting, by mouth, ADULT, 4 to 10 mg
1–2 times daily for 2–4 days.
Multiple myeloma, by mouth or by IV injection, ADULT, 40
mg daily, days 1 to 4, 9 to 12, and 17 to 20, repeated
every 4 weeks, alone or as part of a regimen.
Multiple sclerosis, by mouth, ADULT, 30 mg daily for 1 week,
followed by 4–12 mg daily for 1 month.
Treatment of Addisonian crisis or shock, by IV injection,
ADULT, 4–10 mg as a single dose, may be repeated if
necessary.
Treatment of unresponsive shock, by IV route, ADULT, 1-6
mg/kg as a single dose or up to 40 mg initially followed
by repeat doses every 2–6 hours while shock persists.
Physiological replacement, by mouth or by IM or IV injection,
ADULT, as sodium phosphate, 0.03–0.15 mg/kg daily or
0.6 to 0.75 mg/m2 daily in divided doses every 6–12
hours; CHILD, 0.03 to 0.15 mg/kg daily or 0.6–0.75
mg/m2 daily in divided doses every 6-12 hours.
Croup or laryngotracheobronchitis, by mouth or by IM or IV
injection, CHILD, 0.6 mg/kg once (usual maximum dose,
16 mg; doses as high as 20 mg have been used), a single
oral dose of 0.15 mg/kg has been shown effective in
children with mild-to-moderate croup.
Bacterial meningitis, by IV injection, INFANT and CHILD >6
weeks, 0.15 mg/kg per dose every 6 hours for the first
2–4 days of antibiotic treatment; initiate 10–20 minutes
before or with the first dose of antibiotic.
Cushing's syndrome, diagnosis, by mouth, ADULT, 1 mg at
11 PM, draw blood at 8 AM; greater accuracy for
Cushing's syndrome may be achieved by the following:
0.5 mg every 6 hours for 48 hours (with 24hour urine
collection for 17hydroxycorticosteroid excretion)
Differentiation of Cushing's syndrome due to ACTH
excess from Cushing's due to other causes, 2 mg every 6
hours for 48 hours (with 24hour urine collection for
17hydroxy-corticosteroid excretion).
Adverse Drug Reactions: Arrhythmia, bradycardia, cardiac
arrest, cardiomyopathy, CHF, circulatory collapse,
edema, hypertension, myocardial rupture (post-MI),
syncope, thromboembolism, vasculitis, depression,
euphoria, emotional instability, headache, increased
intracranial pressure, insomnia, malaise, neuritis, mood
swings, personality changes, pseudotumor cerebri
(following discontinuation), seizure, psychic disorders,
vertigo, allergic dermatitis, acne, alopecia, angioedema,
bruising, dry skin, erythema, fragile skin, hypertrichosis,
hirsutism, hyperpigmentation or hypopigmentation, rash,
perianal pruritus (following IV injection), petechiae, skin
atrophy, impaired skin test reaction, striae, urticaria,
impaired wound healing, adrenal suppression,
decreased carbohydrate tolerance and glucose
intolerance, Cushing's syndrome, diabetes mellitus,
growth suppression (children), hypokalemic alkalosis,
hyperglycemia, menstrual irregularities, negative
nitrogen balance, protein catabolism, pituitary-adrenal
axis suppression, sodium retention, abdominal
distention, increased appetite, GI hemorrhage, GI
perforation, pancreatitis, peptic ulcer, ulcerative
esophagitis, weight gain; altered spermatogenesis,
hepatomegaly, nausea, arthropathy, aseptic necrosis
(femoral and humoral heads), fractures, muscle mass
loss, myopathy (in conjunction with neuromuscular
disease or neuromuscular-blocking agents),
thrombophlebitis, neuropathy, osteoporosis,
paresthesia, tendon rupture, weakness, vertebral
compression fractures, cataracts, exophthalmos,
glaucoma, increased intraocular pressure, glucosuria,
pulmonary edema, abnormal fat deposition,
anaphylactoid reaction, anaphylaxis, avascular necrosis,
diaphoresis, hiccups, hypersensitivity, impaired wound
healing, infections, Kaposi sarcoma, moon face,
secondary malignancy
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Dexamethasone:
Trastuzumab (neutropenic effect)
Enhances therapeutic effect of Warfarin (anticoagulant
effect)
Increases risk of adverse or toxic effects of Dexamethasone:
Denosumab (serious infections), Salicylates (GI
ulceration and bleeding)
Increases risk of adverse or toxic effects of the following
drugs:
Acetylcholinesterase Inhibitors e.g. pyridostigmine
edrophonium (increased muscular weakness),
Amphotericin B, Thiazide Diuretics, Loop Diuretics
(hypokalemic effect), Androgens (fluid-retaining effect),
COX-2 Inhibitors e.g. Celecoxib, Deferasirox (GI
ulceration or irritation; GI bleeding), NSAID (Non-
selective), Quinolone Antibiotics e.g. Levofloxacin
(tendonitis; tendon rupture)
Reduces absorption of Dexamethasone:
Bile Acid Sequestrants
Reduces diagnostic effect of Coccidioides immitis Skin Test
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Calcitriol, Corticorelin (blunts
plasma ACTH response to corticorelin), Urea Cycle
Disorder Agents (increases protein catabolism and
plasma ammonia concentrations, increasing doses of
Urea Cycle Disorder Agents needed to maintain
concentrations in the target range)
Avoid concomitant use with:
Decreases bioavailability of Dexamethasone:
Antacids [separate doses by at least 2 hours]
Decreases serum concentration of Dexamethasone:](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-234-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
191
Fosphenytoin, Phenytoin
Decreases serum concentration of the following drugs:
Dasatinib, Fosphenytoin, Imatinib [increase Imatinib
dose by at least 50%], Nilotinib, Phenytoin, Rilpivirine,
Ticagrelor [including its active metabolites], Vincristine
Enhances therapeutic effect of Dexamethasone:
Nondepolarazing Neuromuscular-Blocking Agents e.g.
Pancuronium, Atracurium (neuromuscular effect)
Enhances therapeutic effect of Thalidomide (thrombogenic
effect)
Increases risk of adverse or toxic effects of Dexamethasone:
Nondepolarizing Neuromuscular-Blocking Agents,
(increased muscle weakness, possibly progressing to
polyneuropathies and myopathies)], Pimecrolimus,
Tacrolimus (Topical)
Increases risk of adverse or toxic effects of the following
drugs:
Leflunomide (hematologic toxicity such as pancytopenia,
agranulocytosis, and/or thrombocytopenia),
Thalidomide (dermatologic adverse effect), Tofacitinib
(immunosuppressive effect), Vaccines (Live)
Increases serum concentration of Dexamethasone:
Mifepristone
Increases serum concentration of the following drugs:
Fosphenytoin, Phenytoin
Reduces therapeutic effect of Dexamethasone:
Mifepristone
Reduces therapeutic effect of the following drugs:
Aldesleukin (antineoplastic effect), BCG, (boosting
effects), Hyaluronidase, Vaccines (Inactivated)
[complete all age-appropriate vaccinations at least 2
weeks prior to starting Dexamethasone; if vaccinated
during Dexamethasone therapy, revaccinate at least 3
months after discontinuation],
Unknown impact on the therapeutic effect of Budesonide EC
Tablets (could dissolve prematurely if given with drugs
that lower gastric acid)
Administration: For oral administration, take after meals or
with food or milk to decrease GI effects. Increased
dietary intake of pyridoxine, vitamins A, B6, C, D, folate,
calcium, zinc, and phosphorus is also recommended.
See General Information on Corticosteroids for Systemic
Use – Glucocorticoids listed under Chapter 6: Systemic
Hormonal Preparations for further information.
Pregnancy Category: C
ATC Code: H02AB02
Rx HYDROCORTISONE
Oral: 5 mg and 20 mg tablet
Inj.: 100 mg and 250 mg (as sodium succinate), vial (IV)
50 mg/mL (as sodium succinate), 2 mL vial (IM, IV)
125 mg/mL powder (as sodium succinate), 2 mL vial
(IV)
A glucocorticoid used for replacement therapy in adrenal
insufficiency, management of autoimmune and
inflammatory conditions, and as emergency
management of anaphylaxis and severe systemic
allergies.
Indications: Management of autoimmune or inflammatory
conditions; endocrinal disorders; management of all
conditions requiring corticosteroids; replacement
therapy in cases of adrenocortical insufficiency (usually
in combination with a more potent mineral corticoid);
hypersensitivity reactions, such as anaphylactic shock
and angioedema; bilateral adrenalectomy
Contraindications: Systemic fungal infections; serious
infections, except septic shock or tuberculous
meningitis; viral, fungal, or tubercular skin lesions;
infective arthritis, skin or soft tissue infections near joints
or a prosthetic joint; concurrent administration of live
virus vaccines and immunosuppressive doses of
corticosteroids; IM administration in idiopathic
thrombocytopenia purpura; intrathecal administration
Dose:
Anti-inflammatory, by IV or IM injection, ADULT, 100 to 500
mg 3 or 4 times daily; CHILD, 2–4 mg/kg every 6 hours
for 24 hours, reduce over subsequent 24 hours or
change to oral prednisone
by mouth, ADULT, 20–240 mg once daily.
Initial control of autoimmune disease, by IV injection,
ADULT, 100–500 mg 3 or 4 times daily according to
severity of condition.
Status asthmaticus, by IV injection, ADULT and CHILD, 1–2
mg/kg per dose every 6 hours for 24 hours, then
maintenance of 0.5–1 mg/kg every 6 hours.
Physiologic replacement, by mouth, CHILD, 0.4–0.8 mg/m2
daily divided in 2–3 divided doses.
Stress dosing, surgery in patients who are adrenally-
suppressed or on chronic systemic steroids, by IV
injection, ADULT:
Level of
Stress
Conditions Dose
Minor
Inguinal
herniorrhaphy
25 mg for 1 day
Moderate
Joint replacement,
cholecystectomy
50–75 mg daily
(25 mg every 8–
12 hours) for 1–2
days
Major
Pancreatico-
duodenectomey,
esophago-
gastrectomy,
cardiac surgery
100–150 mg
daily
(50 mg every 8–
12 hours) for 2–3
days](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-235-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
192
Dose Adjustment:
Renal and Hepatic Impairment:
For mild-to-moderate impairment, dose reduction is
warranted.
For severe impairment, refer patient to a specialist.
Adverse Drug Reactions:
Common: Acne, adrenal suppression, amenorrhea,
bruising, delayed wound healing, dyslipidemia,
dyspepsia, edema, fat redistribution, fractures, growth
retardation, hirsutism, hyperglycemia, hypertension,
hypokalemia, increased appetite, increased
susceptibility to infection, masking of signs of infection,
muscle weakness and wasting, myopathy, osteoporosis,
psychiatric effects, skin atrophy, sodium and water
retention, weight gain
Less Common: Glaucoma, ocular hypertension,
osteonecrosis (femoral and humeral heads)
Rare: Anaphylactoid reaction, chorioretinopathy (central),
euphoria, hypersensitivity reactions, hypomania, peptic
ulceration, tendon rupture
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Hydrocortisone:
Trastuzumab (neutropenic effect)
Enhances therapeutic effect of the following drugs:
Warfarin (anticoagulant effect)
Increases risk of adverse or toxic effects of Hydrocortisone:
Denosumab (serious infections), Salicylates (GI
ulceration and bleeding)
Increases risk of adverse or toxic effects of the following
drugs:
Acetylcholinesterase Inhibitors (increased muscular
weakness), Amphotericin B, Thiazide Diuretics, Loop
Diuretics (hypokalemic effect), Androgens (fluid-
retaining effect), COX-2 Inhibitors e.g. Celecoxib,
Deferasirox (GI ulceration or irritation; GI bleeding),
NSAID (Non-selective), Quinolone Antibiotics (tendonitis;
tendon rupture)
Reduces absorption of Hydrocortisone:
Bile Acid Sequestrants
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Calcitriol, Corticorelin (blunts
plasma ACTH response to Corticorelin), Urea Cycle
Disorder Agents (increases protein catabolism and
plasma ammonia concentrations, increasing doses of
Urea Cycle Disorder Agents needed to maintain
concentrations in target range)
Reduces diagnostic effect of Coccidioides immitis Skin Test
Avoid concomitant use with:
Decreases bioavailability of Hydrocortisone:
Antacids [separate doses by at least 2 hours]
Increases risk of adverse or toxic effects of Hydrocortisone:
Nondepolarazing Neuromuscular-Blocking Agents,
(increased muscle weakness, possibly progressing to
polyneuropathies and myopathies), Pimecrolimus,
Tacrolimus (Topical)
Increases risk of adverse or toxic effects of the following
drugs:
Diuretics e.g., Furosemide, Hydrochlorothiazide
(hypokalemia), Drugs controlling Blood Glucose
Concentration (may increase blood glucose
concentration; may alter control of diabetes),
Leflunomide (hematologic toxicity such as pancytopenia,
agranulocytosis, and/or thrombocytopenia), Tofacitinib
(immunosuppressive effect), Vaccines (Live)
Increases serum concentration of Hydrocortisone:
Mifepristone
Reduces therapeutic effect of Hydrocortisone:
Mifepristone
Reduces therapeutic effect of the following drugs:
Aldesleukin (antineoplastic effect), Amlodipine,
Antihypertensives (e.g., Enalapril, Isosorbide Dinitrate,
Methyldopa), Diuretics (e.g., Furosemide,
Hydrochlorothiazide (antagonizes hypotensive effect),
BCG (Intravesical)
Reduces therapeutic effect of the following drugs:
Hyaluronidase, Vaccines (Inactivated [complete all age-
appropriate vaccinations at least 2 weeks prior to
starting Dexamethasone; if vaccinated during
Dexamethasone therapy, revaccinate at least 3 months
after discontinuation]), Vaccines (Live)
Reduces absorption of Calcium Salts
Unknown impact on the therapeutic effect of Budesonide EC
Tablets (could dissolve prematurely if given with drugs
that lower gastric acid)
Administration: Give directly or dilute in normal saline or
D5W. Administer within 24 hours after diluting.
See General Information on Corticosteroids for Systemic
Use – Glucocorticoids listed under Chapter 6: Systemic
Hormonal Preparations for further information.
Pregnancy Category: C; D in the 1st trimester
ATC Code: H02AB09](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-236-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
194
Increases risk of adverse or toxic effects of the following
drugs:
Acetylcholinesterase Inhibitors (increased muscular
weakness), Amphotericin B (hypokalemic effect),
Androgens (fluid-retaining effect), COX-2 Inhibitor,
Deferasirox (GI ulceration or irritation; GI bleeding), Loop
Diuretics (hypokalemic effect), NSAIDs (Non-selective),
Quinolone Antibiotics (tendonitis; tendon rupture),
Thiazide Diuretics (hypokalemic effect)
Reduces absorption of Methylprednisolone:
Bile Acid Sequestrants
Reduces diagnostic effect of Coccidioides immitis Skin Test
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Calcitriol (Systemic), Corticorelin
(blunts plasma ACTH response to Corticorelin), Urea
Cycle Disorder Agents (increases protein catabolism and
plasma ammonia concentrations, increasing doses of
Urea Cycle Disorder Agents needed to maintain
concentrations in target range)
Avoid concomitant use with:
Decreases bioavailability of Methylprednisolone:
Antacids [separate doses by at least 2 hours]
Increases risk of adverse or toxic effects of
Methylprednisolone:
Neuromuscular-blocking agents [Non-depolarizing
(increased muscle weakness, possibly progressing to
polyneuropathies and myopathies)], Pimecrolimus,
Tacrolimus
Increases risk of adverse or toxic effects of the following
drugs:
Leflunomide (hematologic toxicity such as pancytopenia,
agranulocytosis, and/or thrombocytopenia), Tofacitinib
(immunosuppressive effect), Vaccines (Live)
Increases serum concentration of Methylprednisolone:
Mifepristone
Reduces therapeutic effect of Methylprednisolone:
Mifepristone
Reduces therapeutic effect of the following drugs:
Aldesleukin (antineoplastic effect), BCG (Intravesical),
Hyaluronidase, Vaccines (Inactivated [complete all age-
appropriate vaccinations at least 2 weeks prior to
starting Dexamethasone; if vaccinated during
Dexamethasone therapy, revaccinate at least 3 months
after discontinuation]), Vaccines (Live)
Unknown impact on the therapeutic effect of Budesonide EC
Tablets (could dissolve prematurely if given with drugs
that lower gastric acid)
See General Information on Corticosteroids for Systemic
Use – Glucocorticoids listed under Chapter 6: Systemic
Hormonal Preparations for further information.
Pregnancy Category: C
ATC Code: H02AB04
Rx PREDNISOLONE
Oral: 15 mg/5 mL syrup (as sodium phosphate), 60 mL
A synthetic glucocorticoid, which can decrease
inflammation by suppressing migration of
polymorphonuclear leukocytes and by the reversal of
increased capillary permeability. It also suppresses the
immune system by reducing activity and volume of the
lymphatic system.
Indications: Relief of severe asthma; suppression of
inflammatory and allergic disorder
Contraindications: Acute superficial herpes simplex
keratitis; live or attenuated virus vaccines; systemic
fungal infections; varicella
Dose:
NOTE: Asthma Exacerbations. For the short course
outpatient “burst” type, continue burst until symptoms
resolve and the peak expiratory flow is at least 80% of
personal best.
Asthma exacerbations, by mouth, ADULT and CHILD ≥12
years, dose will depend on the type of treatment:
Guideline
Type of
Treatment
Dose
Global
Initiative for
Asthma
(GINA)
2015
Management
in primary
care or acute
care facility
1mg/kg daily as a
single daily dose
usually given for 5–
7 days (maximum,
50 mg daily).
National
Asthma
Education
and
Prevention
Program
(NAEPP)
2007
Asthma
exacerbation
(emergency
care or
hospital
doses)
40–80 mg daily in
a single dose or in
2 divided doses
until peak
expiratory flow is
70% of the
predicted or
personal best.
Short course
outpatient
“burst” (acute
asthma)
40–60 mg daily in
a single dose or in
2 divided doses for
5 to 10 days.
Long-term
treatment
7.5–60 mg daily
given as a single
dose in the
morning or every
other day as
needed for control
of asthma.
Asthma exacerbations, by mouth, CHILD <12 YEARS, dose
will depend on the age of the child,
Based on the Global Initiative for Asthma (GINA)
2015:
Age
(Years)
Dose
Maximum Dose
(mg daily)
<3
1–2 mg/kg daily for up
to 5 days
20
3–5
1–2 mg/kg daily for up
to 5 days
30](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-238-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
195
6–11
1–2 mg/kg daily
usually given for 3–5
days
40
Based on the National Asthma Education and
Prevention Program (NAEPP) 2007 Guidelines:
Type of
Treatment
Dose
Asthma
exacerbation
(emergency
care or hospital
doses)
1–2 mg/kg daily in 2 divided
doses (maximum, 60 mg daily)
until peak expiratory flow is 70%
of the predicted or personal best.
Short course
outpatient
“burst” (acute
asthma)
1–2 mg/kg daily as a single dose
or in 2 divided doses for 3–10
days (maximum dose, 60 mg
daily).
Long-term
treatment
0.25–2 mg/kg daily as a single
dose in the morning or every
other day as needed for control of
asthma (maximum dose, 60 mg
daily).
Rheumatoid arthritis, by mouth, ADULT, initially 5–7.5 mg
daily, then adjust dose as needed.
Multiple sclerosis, by mouth, ADULT, 200 mg daily for 1
week followed by 80 mg every other day for 1 month.
Anti-inflammatory or immunosuppressant, by mouth,
ADULT, 5–60 mg in 2–4 divided doses (maintenance,
2.5–15 mg daily); CHILD, 1–2 mg/kg once daily
(maximum, 60 mg daily).
Nephrotic syndrome, by mouth, CHILD, for the first 3
episodes, initially 2 mg/kg daily or 60 mg/m2 daily
(maximum, 80 mg daily) in 3–4 divided doses until urine
is protein-free for 3 consecutive days (maximum of 28
days), followed by 1–1.5 mg/kg per dose or 40 mg/m2
per dose given every other day for 4 weeks; for frequent
relapses, 0.5–1 mg/kg per dose as maintenance every
other day for 3–6 months.
Dose Adjustment:
Renal Impairment:
For patients undergoing hemodialysis, administer
appropriate dose post-hemodialysis since the drug is
slightly dialyzable.
Precautions:
Cataracts; Glaucoma
Adverse Drug Reactions:
Common: Cardiomyopathy, CHF, edema (including facial),
hypertension, headache, insomnia, malaise,
nervousness, pseudotumor cerebri, psychic disorders,
seizure, vertigo, bruising, facial erythema, hirsutism,
petechiae, skin test reaction suppression, thin fragile
skin, urticaria, decreased carbohydrate tolerance,
Cushing's syndrome, growth suppression,
hyperglycemia, diabetes mellitus, hypernatremia,
hypokalemia, hypokalemic alkalosis, menstrual
irregularities, negative nitrogen balance, pituitary-
adrenal axis suppression, abdominal distention,
increased appetite, indigestion, nausea, pancreatitis,
peptic ulcer, ulcerative esophagitis, weight gain,
arthralgia, aseptic necrosis (humeral or femoral heads),
fractures, tendon rupture, decreased muscle mass,
muscle weakness, osteoporosis, steroid myopathy,
weakness, cataracts, exophthalmus, eyelid edema,
glaucoma, increased intraocular pressure, epistaxis,
increased diaphoresis, irritation, impaired wound healing
Rare: Venous thrombosis
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Prednisolone:
Trastuzumab (neutropenic effect)
Enhances therapeutic effect of Warfarin (anticoagulant
effect)
Increases risk of adverse or toxic effects of Prednisolone:
Denosumab (serious infections), Salicylates (GI
ulceration and bleeding)
Increases risk of adverse or toxic effects of the following
drugs:
Acetylcholinesterase Inhibitors e.g. Neostigmine,
Edrophonium (increased muscular weakness),
Amphotericin B (hypokalemic effect), Androgens e.g.
Testosterone (fluid-retaining effect), COX-2 Inhibitors,
Deferasirox (GI ulceration or irritation; GI bleeding), Loop
Diuretics, Thiazide Diuretics (hypokalemic effect),
NSAIDs (Non-selective), Quinolone Antibiotics e.g.
Levofloxacin (tendonitis; tendon rupture)
Reduces absorption of Prednisolone:
Bile Acid Sequestrants e.g. Cholestryramine
Reduces diagnostic effect of Coccidioides immitis Skin Test
Reduces therapeutic effect of the following drugs:
Antidiabetic Agents, Calcitriol (Systemic), Corticorelin
(blunts plasma ACTH response to Corticorelin), Urea
Cycle Disorder Agents (increases protein catabolism and
plasma ammonia concentrations, increasing doses of
Urea Cycle Disorder Agents needed to maintain
concentrations in target range)
Avoid concomitant use with:
Decreases bioavailability of Prednisolone:
Antacids [separate doses by at least 2 hours]
Increases risk of adverse or toxic effects of Prednisolone:
Nondepolarizing Neuromuscular-blocking Agents
(increased muscle weakness, possibly progressing to
polyneuropathies and myopathies), Pimecrolimus,
Tacrolimus (Topical)
Increases risk of adverse or toxic effects of the following
drugs:
Leflunomide (hematologic toxicity such as pancytopenia,
agranulocytosis, and/or thrombocytopenia), Tofacitinib
(immunosuppressive effect), Vaccines (Live)
Increases serum concentration of Prednisolone:
Mifepristone, Ritonavir
Reduces therapeutic effect of Prednisolone:
Mifepristone
Reduces therapeutic effect of the following drugs:
Aldesleukin (antineoplastic effect), BCG (Intravesical),
Hyaluronidase, Vaccines (Inactivated [complete all age-](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-239-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
196
appropriate vaccinations at least 2 weeks prior to
starting Dexamethasone; if vaccinated during
Dexamethasone therapy, revaccinate at least 3 months
after discontinuation]), Vaccines (Live)
Unknown impact on the therapeutic effect of Budesonide EC
Tablets (could dissolve prematurely if given with drugs
that lower gastric acid)
Administration: Should be taken after meals or with food or
milk to decrease GI effects. Increased dietary intake of
pyridoxine, vitamins A, B6, C, D, folate, calcium, zinc, and
phosphorus is also recommended.
See General Information on Corticosteroids for Systemic
Use – Glucocorticoids listed under Chapter 6: Systemic
Hormonal Preparations for further information.
Pregnancy Category: C or D (product-specific)
ATC Code: H02AB06
Rx PREDNISONE
Oral: 5 mg, 10 mg, and 20 mg tablet
10 mg/5 mL suspension, 60 mL
A corticosteroid with glucocorticoid and anti-inflammatory
effects that can suppress adrenal function at high doses.
It is rapidly converted to the prednisolone in the body. Its
antitumor effects may be related to the inhibition of
glucose transport, phosphorylation, or induction of cell
death in immature lymphocytes. Its antiemetic effects
are thought to occur due to blockade of cerebral
innervations of the emetic center by inhibiting
prostaglandin synthesis.
Indications: Management of autoimmune disease; croup;
short-term suppression of inflammation in allergic
disorders; Pneumocystis carinii pneumonia; atopic
dermatitis; dermatomyositis or polymyositis; nephrotic
syndrome (idiopathic or related to lupus erythematosus);
immune-mediated thrombocytopenia; inflammatory
bowel disease; eye inflammation; rheumatic disease;
immunosuppression; acute severe asthma (reliever);
severe persistent asthma not responding to high-dose
inhaled steroids, long-acting agonists, and
methylxanthines (controller); adrenal insufficiency
Contraindications: Untreated systemic fungal infections;
administration of live attenuated virus vaccines with
immunosuppressive doses of prednisone
Dose:
NOTE: No definitive treatment guidelines exist. Dosing is
dependent on institution protocols and individual
response.
General dosing range, by mouth, initially 5–60 mg daily:
RECOMMENDATIONS ON APPROPRIATE USE:
Prior to use, dose and duration of treatment should be
based on the risk versus benefit for each individual
patient. Generally, use the smallest effective dose for the
shortest duration of time to minimize the adverse events.
Consider alternate day therapy for long-term therapy to
reduce adverse effects.
Dosage for infants and children should be based on severity
of the disease and response of the patient rather than
age, weight, or body surface area.
Gradually taper dose prior to discontinuing therapy,
especially long-term therapy. Abrupt withdrawal may
precipitate acute adrenal insufficiency.
Individualize tapering of dose based on the disease and
severity of condition. For example, the dose may be
tapered off by 10–20% every 3–5 days until a dose of 10
mg daily is reached. A slower weekly tapering is
recommended.
Autoimmune or inflammatory disease, by mouth, ADULT,
initially 5–60 mg once daily depending on the disease
and its severity, adjust dose according to response and
recommended guidelines; CHILD, initially 1–2 mg/kg
once daily (usual maximum dose, 60 mg) with dose
adjustments based on guidelines.
Croup, by mouth, CHILD, 1 mg/kg; repeat dose after 12–24
hours if necessary.
Pneumocystis carinii pneumonia, by mouth, ADULT, begin
within 72 hours of PCP therapy: 40 mg twice daily for 5
days, followed by 20 mg once daily for 11 days or until
antimicrobial regimen is completed; CHILD, 1 mg/kg
twice daily for 5 days, followed by 0.5–1 mg/kg twice
daily for 5 days, followed by 0.5 mg/kg once daily for 11–
21 days.
Acute asthma, by mouth, ADULT, 40–60 mg daily for 3–10
days as a single dose or in 2 divided doses; CHILD <12
years, 1–2 mg/kg daily for 3–10 days, with a maximum
of 60 mg daily.
Rheumatoid arthritis, by mouth, ADULT, ≤10 mg daily
[NOTE: Once the condition has stabilized, reduce to the
minimum required to maintain control of disorder.]
Acute gout, by mouth, ADULT, initially at least 0.5 mg/kg for
5–10 days.
Dermatomyositis/polymyositis, by mouth, ADULT, 1 mg/kg
daily (range of 0.5–1.5 mg/kg daily), often in conjunction
with steroid-sparing therapies.
Immune thrombocytopenia, by mouth, ADULT, 1–2 mg/kg
daily.
Nephrotic syndrome, by mouth, CHILD, initially 2 mg/kg
daily or 60 mg/m2 daily in 1–3 divided doses, with a
maximum of 80 mg daily until urine is protein free for 4–
6 weeks; followed by a maintenance dose of 2 mg/kgor
40 mg/m2every other day in the morning; discontinue
after 4–6 weeks by gradual tapering.
Lupus nephritis, induction, by mouth, ADULT, the following
doses apply:
Lupus
Nephritis
Class
Dose
III–IV
0.5–1 mg/kg daily (after glucocorticoid pulse)
tapered, after a few weeks, to the lowest
effective dose, combined with an
immunosuppressive agent
V
0.5 mg/kg daily for 6 months combined with
mycophenolate mofetil and, if no improvement is
seen after 6 months, use 0.5–1 mg/kg daily
(after glucocorticoid pulse) for an additional 6
months combined with cyclophosphamide](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-240-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
197
Dose Adjustment:
Renal Impairment:
For mild-to-moderate renal impairment, dose reduction is
warranted.
For severe impairment, refer patient to a specialist.
Adverse Drug Reactions:
Common: Acne, adrenal suppression, amenorrhea,
bruising, delayed wound healing, dyslipidemia,
dyspepsia, edema, fat redistribution, fractures, growth
retardation, hirsutism, hyperglycemia, hiccups,
hypertension, hypokalemia, increased appetite,
increased susceptibility to infections, malaise, masking
of signs of infection, muscle weakness and wasting,
myopathy, nausea, osteoporosis, psychiatric effects, skin
atrophy, sodium and water retention, weight gain
Less Common: Glaucoma, ocular hypertension,
Osteonecrosis or aseptic necrosis (femoral and humeral
heads)
Rare: Anaphylactoid reaction, chorioretinopathy (central),
euphoria, hypersensitivity reactions, hypomania, peptic
ulceration, tendon rupture
Drug Interactions:
NOTE: Prednisone is a substrate for CYP3A-based
interaction.
Please see Drug Interactions under Prednisolone
Administration: Best taken with food. Taking it early in the
morning reduces possible side effects.
See General Information on Corticosteroids for Systemic
Use – Glucocorticoids listed under Chapter 6: Systemic
Hormonal Preparations for further information.
Pregnancy Category: C; D in the 1st trimester
ATC Code: H02AB07
THYROID THERAPY
THYROID PREPARATIONS
Rx LEVOTHYROXINE
Oral: 50, 100, and 150 micrograms tablet (as
sodium/anhydrous sodium)
A synthetic form of thyroxine (T4), a thyroid hormone
involved in normal metabolism, growth, and
development. It promotes gluconeogenesis, increase
utilization of glycogen stores, stimulate synthesis of
proteins, and increase basal metabolic rate.
Indications: Management of hypothyroidism of any etiology;
TSH suppression
Contraindications: Hyperthyroidism from any cause; acute
MI; untreated subclinical (suppressed serum TSH level
with normal T3 and T4 levels); overt thyrotoxicosis of any
etiology; uncorrected adrenal insufficiency
Dose:
Chronic hypothyroidism, by mouth, CHILD, initially 25
micrograms daily, adjust by 25 micrograms every 2–4
weeks.
Congenital hypothyroidism, juvenile myxedema, by mouth,
NEONATE ≤1 month, initially 5–10 micrograms/kg daily,
adjust by 25 micrograms every 2–4 weeks until mild
toxic symptoms appear, then reduce dose slightly;
INFANT and CHILD >1 month, 5 micrograms/kg daily,
adjust by 25 micrograms every 2–4 weeks until mild
toxic symptoms appear, then reduce dose slightly.
Severe hypothyroidism, by mouth, ADULT, initially 12.5–25
micrograms daily, adjust by 25 micrograms every 2–4
weeks, as appropriate; CHILD, initially 25 micrograms
daily, adjust by 25 micrograms every 2–4 weeks
Subclinical hypothyroidism, if treated, by mouth, ADULT, 1
microgram/kg daily.
Hypothyroidism, by mouth, ADULT, usually 1.6–1.7
micrograms/kg daily, may give full dose right away if
without contraindications; for most, initially 50–100
micrograms daily before breakfast (25–50 micrograms
for patients >50 years), increase by 25–50 micrograms
every 3 to 4 weeks until normal metabolism is
maintained (maintenance dose, 100–200 micrograms
daily);
CHILD, dose would depend on the age:
Age Daily Dose (microgram/kg)
1–3
months*
10–15
3–6 months 8–10
6–12
months
6–8
1–5 years 5–6
6–12 years 4–5
>12 years 2–3
[NOTE: For infants 1-3 months at risk for developing
cardiac failure, administer a lower starting dose of 25
micrograms daily. If the initial serum thyroxine is
below 5 micrograms/dL, begin treatment at a higher
dose of 50 micrograms daily (12–17 micrograms/kg
daily).];
in cardiac disease, initially 25 micrograms daily or 50
micrograms on alternate days, adjusted by 25
micrograms every 4 weeks);
dosing for specific populations:
Population Dose
Adults <50 years;
children in whom
growth and puberty
are complete; adults
>50 years recently
treated for
hyperthyroidism or
who have been
hypothyroid for only a
few months
1.6–1.7
micrograms/kg daily;
usually ≤200
micrograms daily;
titrate dose every 6
weeks; may give full
dose right away if
without
contraindications.
Adults <50 years with
or without cardiac
disease
Initially 25–50
micrograms daily,
adjust by 12.5–25
microgram
increments at 6– to](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-241-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
198
8-week intervals, as
needed.
Adults >50 years with
cardiac disease
Initially 12.5–25
micrograms daily,
then adjusted by
12.5–25 microgram
increments at 4- to
6-week intervals, as
needed.
TSH suppression in well-differentiated thyroid cancer,
papillary and follicular, by mouth, ADULT, dose is highly
individualized; in general, more than 2 micrograms/kg
daily may be needed to suppress TSH to <0.1 mIU/L in
intermediate- to high-risk tumors; low-risk tumors may be
maintained at 0.1–0.5 mIU/L.
TSH suppression in benign nodules and nontoxic
multinodular goiter, by mouth, ADULT, initially 1.7–2
micrograms/kg daily may be used with a target TSH of
0.1–0.3 mIU/L [NOTE: Routine use is not recommended.
Avoid if TSH is already suppressed].
Dose Adjustment:
Geriatric:
Introduce gradually to avoid sudden increase in metabolic
demands. Maintenance replacement dose may be less
than in younger people.
The initial dose should not exceed 25–50 micrograms daily.
Maintain at intervals of at least 4 weeks.
Cardiovascular disorders (angina, heart failure, myocardial
infarction or insufficiency, hypertension):
Lower initial doses. Smaller increments and longer intervals
between increases could be necessary. Full replacement
dose may not be appropriate. Use with caution and
reduce dose as needed.
Long-standing Hypothyroidism:
Introduce gradually to avoid sudden increase in metabolic
demands. Maintenance replacement dose may be less
than in younger people.
Precautions:
WARNING: Use with caution in patients with underlying
coronary artery disease, previous MI, or acute coronary
syndromes and tachyarrhythmias.
Thyroid supplements are ineffective and potentially toxic
when used for the treatment of obesity or for weight
reduction, especially in euthyroid patients. High doses may
produce serious or even life-threatening toxic effects,
particularly when used with some anorectic.
Cardiovascular disorders, including angina, heart failure,
myocardial infarction or insufficiency, and hypertension;
Hypopituitarism or predisposition to adrenal insufficiency
(correct with a corticosteroid prior to treatment with
levothyroxine to prevent precipitation of an acute adrenal
crisis, e.g., panhypopituitarism);
Adrenal insufficiency (in uncorrected adrenal insufficiency,
glucocorticoid treatment should precede use of
levothyroxine);
Myxedema;
Diabetes insipidus or diabetes mellitus (may need to
increase dose of insulin or oral antidiabetic drug);
Myasthenic syndrome;
Osteoporosis;
Benign thyroid nodules (treatment should never be fully
repressive;
Avoid use in postmenopausal women, men more than 60
years of age, patients with cardiovascular disease,
osteoporosis, or systemic illness, and patients with large
thyroid nodules or long-standing goiters, or low-normal
TSH levels);
Elderly;
Pregnancy (monitor thyroid function each trimester;
reassess thyroxine maintenance dosage 6–8 weeks
post-partum);
Lactation (amount is too small to affect tests for neonatal
hypothyroidism).
Adverse Drug Reactions:
Common: Anginal pain, excitability, headache, flushing,
muscular weakness, restlessness, sweating, vomiting,
weight loss
Less Common: Cramps, diarrhea, nervousness, insomnia,
palpitations, tachycardia
Rare: Arrhythmias, decreased bone density (women),
papilledema, seizures, tremors
Drug Interactions:
Monitor closely with:
Decreases metabolism of Theophylline (hypothyroidism)
Enhances therapeutic effect of the following drugs:
Anticoagulants e.g. Warfarin, Tricyclic Antidepressants
e.g. (stimulatory effect)
Increases metabolism of Levothyroxine, increasing its
requirements in hypothyroidism:
Phenobarbital, Phenytoin, Rifampicin
Increases risk of adverse or toxic effects of Levothyroxine:
Piracetam (confusion, irritability, and sleep disorders)
Increases risk of adverse or toxic effects of the following
drugs:
Tricyclic Antidepressants (arrhythmogenic effect)
Reduces therapeutic effect of Levothyroxine:
Selective Serotonin Reuptake Inhibitors
Avoid concomitant use with:
Decreases serum concentration of Levothyroxine:
Aluminum Hydroxide [administer at least 4 hours apart],
Bile Acid Sequestrants [administer 4 hours prior to
Colesevelam; administer at least 1 hour before or 4–6
hours after Cholestyramine]
Decreases serum concentration of Levothyroxine:
Calcium Polystyrene Sulfonate [separate dosing or
administer Calcium Polystyrene Sulfonate rectally],
Lanthanum [administer at least 2 hours apart],
Magnesium Salts [administer at least 4 hours apart],
Multivitamins / Minerals (with ADEK, Folate, Iron)
[administer at least 4 hours apart], Sevelamer, Sodium
Polystyrene Sulfonate [separate dosing or administer
Sodium Polystyrene Sulfonate rectally], Sucroferric
Oxyhydroxide](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-242-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
199
Reduces absorption of Levothyroxine, reducing its
therapeutic effect, resulting to hypothyroidism:
Calcium Salts [administer at least 4 hours apart],
Ciprofloxacin, Ferrous Salts [administer at least 4 hours
apart], Orlistat, Raloxifene, Simethicone
Reduces therapeutic effect of Sodium Iodide I 131
Administration: Should be taken in the morning on an empty
stomach, at least 30–90 minutes before food intake.
The tablet may be crushed and suspended in 5 to 10 mL
water, however, this must be used immediately.
Pregnancy Category: A
ATC Code: H03AA01
ANTITHYROID PREPARATIONS
Rx PROPYLTHIOURACIL
Oral: 50 mg tablet
An antithyroid agent derived from thiourea. It inhibits the
peripheral conversion of thyroxine to triiodothyronine in
the tissues.
Indication: Treatment of hyperthyroidism
Contraindication: Breastfeeding patients
Dose:
Hyperthyroidism, by mouth, ADULT, initially 300–400 mg
daily in 3 equally divided doses at 8-hour intervals;
Severe hyperthyroidism and/or very large goiters, by mouth,
ADULT, 400 mg daily; some may require 600–900 mg
daily; maintenance dose is usually at 100–150 mg daily
in 3 equally divided doses; ADOLESCENT and CHILD >10
years, initially 150–300 mg daily in 3 equally divided
doses, then maintain at 50 mg twice daily when
euthyroid; CHILD 6–10 years, initially 50–150 mg daily
in 3 equally divided doses, then maintain at 50 mg twice
daily when euthyroid.
Precautions:
WARNING: Severe liver injury and acute liver failure
(sometimes fatal) were reported, requiring liver
transplantation in some patients, including
pregnant women. Reserve use of PTU for
patients who cannot tolerate methimazole or in
whom radioactive iodine therapy or surgery are
not appropriate.
Treatment of choice when antithyroid is
indicated during to or just prior to first trimester
of pregnancy due to the risk of fetal
abnormalities associated with the use of
methimazole.
Bleeding; Bone marrow suppression (discontinue if
significant bone marrow suppression occurs, particularly
agranulocytosis or aplastic anemia);
Dermatologic toxicity;
Hypothyroidism;
Lupus-like syndrome;
Nephritis;
Interstitial pneumonitis; Vasculitis
Adverse Drug Reactions: Allergy, periarteritis, edema,
vasculitis (ANCA-positive, cutaneous, leukocytoclastic),
drowsiness, headache, drug fever, neuritis, paresthesia,
vertigo, alopecia, dermal ulcer, erythema nodosum,
exfoliative dermatitis, pruritus, skin pigmentation, skin
rash, Stevens-Johnson syndrome, toxic epidermal
necrolysis, urticaria, ageusia, dysgeusia, nausea, salivary
gland disease, stomach pain, vomiting, agranulocytosis,
aplastic anemia, granulocytopenia,
hypoprothrombinemia, acute hepatic failure,
hemorrhage, leukopenia, lymphadenopathy,
thrombocytopenia, hepatitis, hepatotoxicity, jaundice,
arthralgia, lupus-like syndrome, splenomegaly, myalgia,
acute renal failure, glomerulonephritis, nephritis;
interstitial pneumonitis, pulmonary alveolar hemorrhage;
fever
Drug Interactions:
Avoid concomitant use with:
Increases risk of adverse or toxic effects of the following
drugs:
Clozapine (agranulocytosis), Dipyrone (agranulocytosis
and pancytopenia)
Reduces therapeutic effect of the following drugs:
BCG, Intravesical, Sodium Iodide I 131 [discontinue
antithyroid therapy 3–4 days prior to sodium iodide I 131
administration], Vitamin K Antagonists [e.g. Warfarin
(anticoagulant effect)]
Pregnancy Category: D
ATC Code: H03BA02
SULFUR-CONTAINING IMIDAZOLE
DERIVATIVES
Rx METHIMAZOLE (THIAMAZOLE)
Oral: 5 mg and 10 mg tablet
A thioamide used as an antithyroid agent that inhibits the
synthesis of thyroid hormones by blocking iodine
oxidation in the thyroid gland.
Indications: For hyperthyroidism; for long-term use (1–2
years) to induce remission in small goiters;
hyperthyroidism associated with Graves’ disease
Contraindications: Previous agranulocytosis to
methimazole; drug-induced nephritis or polyarteritis
nodosa; liver disease; blood disorders, such as
granulocytopenia and aplastic anemia
Dose:
Hyperthyroidism, by mouth, ADULT,
Mild hyperthyroidism, initially 15 mg daily in 3 divided
doses, approximately every 8 hours;](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-243-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
200
Moderately severe hyperthyroidism, 30–40 mg daily;
Severe hyperthyroidism, 60 mg daily;
Maintenance, 5–15 mg daily as a single dose, continue
for 12–18 months to induce remission, or for 6–12
months to prepare patients for definitive therapy in the
form of surgery or radioactive iodine therapy;
CHILD, initially 0.4 mg/kg daily in 3 divided doses,
maintenance: 0.2 mg/kg daily in 3 divided doses;
suggested dosing based on the age:
Population Daily Dose (mg)
Infants 1.25
Children 1–5 years 2.5–5
Children 5–10 years 5–10
Children and
Adolescents 10–18 years
10–20
Dose Adjustment:
Renal Impairment:
For mild-to-moderate renal impairment, dose reduction is
warranted
For severe impairment, refer patient to a specialist.
Hypothyroidism:
Adjust dose to maintain euthyroid state. Monitor THS and
free T4 levels.
Precautions:
Hypoprothrombinemia;
Bone marrow suppression;
Bleeding;
Aplastic anemia;
Thrombocytopenia;
Leukopenia;
Leukocytoclastic vasculitis and positive vasculitis
(discontinuation immediately if vasculitis develops
during therapy);
Dermatologic toxicity (discontinue if exfoliative dermatitis
develops);
Urticaria;
Infection (discontinue at signs of infections, e.g., fever, sore
throat, mouth ulcer, and clinical evidence of
neutropenia;
Hepatic necrosis (hepatitis, fever);
Encephalopathy (discontinue in the presence of hepatitis;
transaminase >3 times upper limit of normal);
Lupus-like syndrome;
Pregnancy (first trimester: can cause fetal harm; high risk of
agranulocytosis if doses >40 mg/day).
Adverse Drug Reactions:
Common: Pruritus, rash
Less Common: Abnormal loss of hair, arthralgia, edema,
epigastric distress, headache, loss of taste,
lymphadenopathy, neuritis, paresthesia, pigmentation,
pruritus, sialadenopathy, urticaria, myalgia, nausea,
vertigo, vomiting
Rare: Agranulocytosis, alopecia, aplastic anemia, drug
fever, granulocytopenia, hypoprothrombinemia,
hepatitis, jaundice, myopathy, nephritis, lupus-like
syndrome, periarteritis, thrombocytopenia
Drug Interactions:
Monitor closely with:
Enhances therapeutic effect of Methimazole:
Anticoagulants e.g. Warfarin
Increases risk of adverse or toxic effects of Methimazole:
Macrolide Antibiotics e.g. Azithromycin (QT-prolongation)
Avoid concomitant use with:
Increases risk of adverse or toxic effects of the following
drugs:
Clozapine (agranulocytosis), Dipyrone (agranulocytosis and
pancytopenia)
Increases serum concentration of Tizanidine [initiate
Tizanidine at 2 mg and increase in 24 mg increments
based on patient response]
Reduces therapeutic effect of the following drugs:
BCG (Intravesical), Sodium Iodide I 131 [discontinue
Methimazole 3–4 days before Sodium Iodide I 131
administration], Vitamin K Antagonists e.g. Warfarin
(anticoagulant effect)
Administration: May be taken with food or milk to reduce
stomach upset.
Pregnancy Category: D
ATC Code: H03BB02
IODINE THERAPY
Rx IODINE
Oral: aqueous iodine solution (Lugol's solution)
5% iodine, 10% potassium iodide (total iodine = 130
mg/mL), 30 mL
An anti-hyperthyroid agent that acts by reducing of the
thyroid gland through various mechanisms, such as the
reduction of vascularity, a firming of the glandular tissue,
and shrinkage of the size of individual cells.
Indication: Antidote to thyroid block following radiation
emergency
Contraindications: Dermatitis herpetiformis;
hypocomplementemic vasculitis, nodular thyroid
condition with heart disease
Dose:
Antidote, by mouth, ADULT (including pregnant and lactating
women), 130 mg once daily for 10–14 days or until risk
of exposure is gone; CHILD, dose should continue for
10–14 days or until risk of exposure has passed; dose
based on age:
Population
Dose (mg
once daily)
1 month and below 16.25
>1 month – 3 years 32.5
>3 years – 12 years 65
>12 years and adolescent
weighing less than 68 kg
65](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-244-320.jpg)
![H
SYSTEMIC HORMONAL PREPARATIONS, EXCLUDING SEX HORMONES AND INSULINS
201
>12 years and adolescent
weighing at least 68 kg
130
Precautions:
Allergy to iodine or potassium iodide;
Skin reactions;
Hypothyroidism;
Adrenal insufficiency, including Addison disease;
Bronchitis;
Cardiac disease;
Myotonia congenital;
Renal impairment tuberculosis.
Adverse Drug Reactions: Cardiac arrhythmia, confusion,
fatigue, fever, numbness, tingling sensation, skin rash,
urticaria, hyperthyroidism (prolonged use),
hypothyroidism (prolonged use), goiter, myxedema,
diarrhea, enlargement of salivary glands, gastric
distress, GI hemorrhage, metallic taste, nausea,
stomach pain, vomiting, lymphedema, thyroid adenoma,
weakness, dyspnea, hypersensitivity reaction
(angioedema, cutaneous and mucosal hemorrhage,
serum sickness-like symptoms), wheezing, iodine
poisoning (prolonged use, high doses)
Drug Interactions:
Monitor closely with:
Increases risk of adverse or toxic effects of the following
drugs:
ACE Inhibitors e.g., Enalapril, Aliskiren
Angiotensin II Receptor Blockers e.g. Losartan, Heparin
(hyperkalemic effect)
Increases risk of adverse or toxic effects of the following
drugs:
Lithium (hypothyroid effect), Nicorandil (hyperkalemic
effect)
Avoid concomitant use with:
Increases risk of adverse or toxic effects of the following
drugs:
Eplerenone (hyperkalemic effect), Potassium-sparing
Diuretics (hyperkalemic effect)
Reduces therapeutic effect of the following drugs:
Sodium Iodide I 131 [discontinue Iodine 3 to 4 days prior
to Sodium Iodide I 131 administration], Vitamin K
Antagonists e.g. Warfarin (anticoagulant effect)
Administration: Administer with food or milk to decrease
gastric irritation. Dilute in a glassful of water, fruit juice,
or milk.
Pregnancy Category: D
ATC Code: H03CA
Rx PROPRANOLOL
Oral: 10 mg and 40 mg tablet (as hydrochloride)
A non-selective beta-adrenergic blocker that competitively
blocks response to beta adrenergic stimulation.
Indications for thyroid diseases are considered as off-
label use.
Indications: Management of thyroid storm, thyrotoxicosis
Contraindications: Uncompensated congestive heart failure
(unless the failure is due to tachyarrhythmias being
treated with propranolol); cardiogenic shock; severe
sinus bradycardia; sick sinus syndrome or heart block
greater than first degree (except in the presence of a
functioning artificial pacemaker); bronchial asthma
Dose:
Thyroid storm, by mouth, ADULT, 60–80 mg every 4 hours.
Thyrotoxicosis, by mouth, ADULT, 10–40 mg/dose every 6–
8 hours; ADOLESCENT and NEONATE, 10–40 mg per
dose every 6 hours.
Administration: To be taken on an empty stomach.
Do NOT withdraw abruptly, particularly in patients with CAD.
Gradually taper dose to avoid acute tachycardia,
hypertension, and/or ischemia.
See individual entry for Propranolol under Cardiac Therapy
– Antiarrhythmics, Class II Antiarrhythmics in Chapter 3:
Cardiovascular System for further information.
Pregnancy Category: C
ATC Code: Not available](https://image.slidesharecdn.com/philippinenationalformulay8thed-220912120445-87e0040a/85/Philippine-National-Formulay-8th-Ed-pdf-245-320.jpg)