Assessment of predictabilityis an important aspect of evaluating adverse drug reactions
(ADRs).
• ADRs can be categorized into two types based on predictability:
– Type-1 (predictable)
– Type-2 (unpredictable) ADRs.
• Type-1 ADRs are more common and are related to the pharmacological effects of the
drug. These reactions are often dose-dependent and can be anticipated as they are
part of the known safety profile of the drug.
• For example, dryness of mouth caused by drugs with anticholinergic properties (like
atropine, benztropine, etc) is a type-1 ADR.
4.
Type-2 ADRsare rare and unpredictable, and they are not related to the
pharmacological effects of the drug.
These reactions are often caused by individual susceptibility or immune
response to the drug.
For instance, anaphylactic shocks caused by penicillin or chloramphenicol-
induced aplastic anaemia are type-2 ADRs.
Predictability assessment of ADRs is crucial in distinguishing between these
two types of reactions and helps in understanding the safety profile of a drug.
5.
Factors Influencing Predictability:
1.Pharmacology of the Drug: Drugs with a narrow therapeutic index or known side-effect profiles
allow more predictable ADRs.
2. Patient Factors: Age, genetics, renal or hepatic function, and concurrent diseases can alter the
predictability of ADRs. For instance, elderly patients are more prone to predictable ADRs due to
altered drug metabolism.
3. Dose: Higher doses increase the likelihood of predictable, dose-dependent ADRs.
4. Drug-Drug Interactions: Known interactions that alter drug levels or effects can predict ADRs (e.g.,
serotonin syndrome when combining SSRIs and MAO inhibitors).
Examples of Predictable ADRs:
– NSAIDs causing gastrointestinal bleeding in high doses or long-term use.
– Opioids causing respiratory depression at higher doses.
– ACE inhibitors causing cough due to accumulation of bradykinin.
6.
Preventability of ADRs
•Preventability refers to the possibility of avoiding an ADR through appropriate drug selection, dose adjustment, monitoring,
or other interventions. The assessment of preventability is crucial in improving patient safety, as preventable ADRs reflect
gaps in healthcare delivery.
Types of Preventable ADRs:
– 1. Preventable ADRs: Occur due to errors in prescribing, dispensing, administration, or patient non-compliance.
– Examples: Overdosing, prescribing a drug despite known allergies, or failing to adjust dose for renal impairment.
– 2. Non-Preventable ADRs: Occur despite appropriate drug use and adherence to guidelines.
– Examples: Unexpected allergic reactions, rare idiosyncratic reactions (e.g., Drug-Induced Liver Injury DILI).
Factors Affecting Preventability:
– Patient Information: Incomplete patient history, such as not knowing a patient’s allergy or not screening for
contraindications.
– Monitoring: Lack of proper therapeutic drug monitoring or failure to adjust therapy in response to lab results (e.g., INR
monitoring with warfarin).
– Guideline Adherence: Not following established clinical guidelines for drug use or ignoring drug safety alerts.
– Patient Education: Patients not being informed about how to take medications correctly or not understanding warning signs
of ADRs.
7.
Tools for AssessingPreventability
1. Schumock and Thornton Criteria: Widely used criteria to determine whether an ADR is
preventable, based on factors like inappropriate drug selection, lack of monitoring, or patient non-
adherence.
• Examples of preventable ADRs based on these criteria:
– Prescribing a contraindicated drug.
– Inadequate monitoring of drug levels (e.g., failure to monitor lithium levels).
– Not discontinuing a drug when contraindications become apparent.
2. Preventability Assessment Flowcharts: These tools provide structured guidance for assessing
preventability by asking questions related to drug selection, patient monitoring, and adherence to
treatment protocols.
• Examples of Preventable ADRs:
– Warfarin-related bleeding due to inadequate INR monitoring.
– Hypoglycemia in a diabetic patient due to inappropriate insulin dosing without considering their diet
or activity level.
– Nephrotoxicity due to improper dose adjustments of a renally cleared drug in a patient with kidney
disease.
8.
3. Assessing Predictabilityand Preventability in Practice
Predictability Assessment:
– 1. Known Drug Profiles: Use the drug’s pharmacokinetics and pharmacodynamics to predict
possible ADRs.
– 2. Patient-Specific Factors: Consider underlying health conditions, age, genetic factors (e.g., testing
for HLA-B5701 in patients taking abacavir to prevent hypersensitivity reactions), and drug
interactions.
– 3. Dose and Duration: Higher doses and prolonged use increase the risk of predictable ADRs.
– 4. Clinical Practice Guidelines: Follow dosing guidelines, monitor for known side effects, and
screen for risk factors.
Preventability Assessment:
– 1. Thorough Patient History: Identify allergies, contraindications, or co-morbid conditions before
prescribing drugs.
– 2. Therapeutic Drug Monitoring: Implement regular monitoring for drugs with narrow therapeutic
indices (e.g., warfarin, lithium).
– 3. Adherence to Guidelines: Use clinical guidelines and decision support tools to ensure proper drug
choice, dosing, and monitoring.
– 4. Patient Education: Educate patients on how to take medications correctly and on early signs of
ADRs (e.g., educating patients on how to manage insulin therapy to prevent hypoglycemia).
– 5. Regular Follow-Up: Ensure timely follow-up, particularly for high-risk medications or patient
populations.
9.
4. Improving Predictabilityand Preventability of ADRs
Pharmacogenomics:
• Pharmacogenomic testing is an emerging tool that improves both
predictability and preventability by identifying genetic factors influencing
drug metabolism, response, and ADR risk. For instance:
• HLA-B5701 testing prevents hypersensitivity to abacavir.
• CYP2D6 genotyping helps prevent ADRs with drugs metabolized by the
CYP450 system (e.g., codeine).
Risk Minimization Strategies:
• Dose Adjustments: Adjust doses in patients with renal or hepatic impairment to
prevent predictable ADRs (e.g., adjusting vancomycin in patients with renal
dysfunction).
• Pre-treatment Screening: Testing patients for specific risk factors (e.g., renal
function tests before using NSAIDs) can reduce preventable ADRs.
• Regulatory and Clinical Monitoring:
• Black Box Warnings: Educating healthcare providers on drugs with known risks,
encouraging regular review of patient medications, and using clinical decision-
support systems to alert prescribers about potential ADRs.
• Reporting ADRs: Spontaneous ADR reporting systems (like MedWatch or
EudraVigilance) are crucial for identifying patterns of ADRs, improving
predictability.
The Schumock andThornton Preventability Assessment Scale (S-T PAS) is a tool developed by
Schumock and Thornton in 1992 to evaluate the preventability of adverse drug reactions (ADRs).
• This tool has become widely used in clinical research and practice.
• The S-T PAS consists of six categories that assess the preventability of ADRs. These categories
include
1. Medication appropriateness
2. Dosing and duration
3. Drug-drug interactions
4. Patient allergies
5. Sensitivities
6. Monitoring
7. Administration errors.
Each category is assigned a score, and the total score determines the preventability of the ADR.
12.
• The higherthe score, the more preventable the ADR. The S-T PAS helps
healthcare providers to identify areas for improvement in medication management,
such as medication selection, dosing, and monitoring.
• It also helps to evaluate the impact of medication errors and implement strategies
to prevent future errors. However, the S-T PAS has limitations. It requires a
comprehensive understanding of the patient's medical history and medication
regimen, which may not always be available.
• Additionally, it does not consider other factors that may contribute to the
preventability of ADRs, such as patient adherence to medication regimens.
13.
• The modifiedform of the preventability assessment tool is commonly used nowadays.
• It assesses whether the adverse drug reaction (ADR) is preventable and classifies it into three
categories:
1. definitely preventable
2. probably preventable
3. non-preventable
• The tool consists of two sections:
– Section A with five questions
– Section B with four questions
• The answers are either "yes" or "no". If any answer in section A is "yes", the ADR is classified
as "definitely preventable".
• If all answers in section A are "no", then section B is used. If any answer in section B is "yes",
the ADR is classified as "probably preventable".
• If all answers in section B are "no", then section C is used, and the ADR is classified as "non-
preventable".
14.
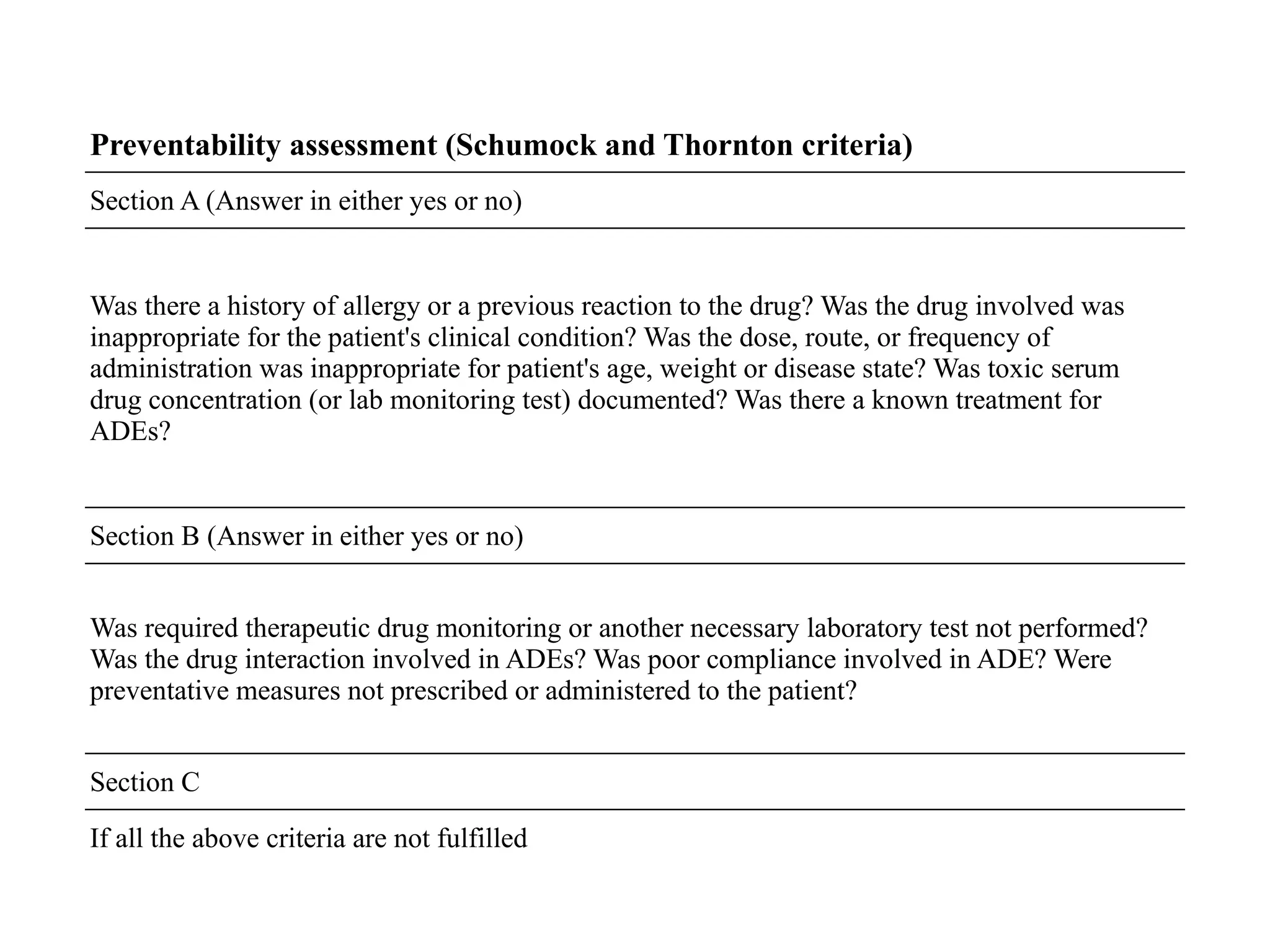
Preventability assessment (Schumockand Thornton criteria)
Section A (Answer in either yes or no)
Was there a history of allergy or a previous reaction to the drug? Was the drug involved was
inappropriate for the patient's clinical condition? Was the dose, route, or frequency of
administration was inappropriate for patient's age, weight or disease state? Was toxic serum
drug concentration (or lab monitoring test) documented? Was there a known treatment for
ADEs?
Section B (Answer in either yes or no)
Was required therapeutic drug monitoring or another necessary laboratory test not performed?
Was the drug interaction involved in ADEs? Was poor compliance involved in ADE? Were
preventative measures not prescribed or administered to the patient?
Section C
If all the above criteria are not fulfilled
15.
• Reporting adversedrug reactions (ADRs) is imperative not only for ensuring optimal patient
care but also for the generation of signals that contribute to drug safety monitoring and
regulatory decision-making.
• In undertaking this review, our objective was to provide a comprehensive overview of the
diverse methods available for the causality assessment of ADRs, aiming to elucidate their
respective benefits and limitations.
• While widely utilized in clinical practice, the WHO causality assessment scales and the
Naranjo probability scale are often favoured due to their accessibility and familiarity.
• However, despite their widespread use, challenges persist, including issues related to
reproducibility, sustainability, and validity.
• It is evident that no single causality assessment tool has achieved universal acceptance across
all clinical contexts, highlighting the ongoing need for research and innovation in this critical
area of pharmacovigilance.









![establishing_pv_centers_in_industry_AND_NATIONAL_PROGRAMME[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/establishingpvcentersinindustryandnationalprogramme1-230725101256-d16cc241-thumbnail.jpg?width=640&height=640&fit=bounds)






















































































