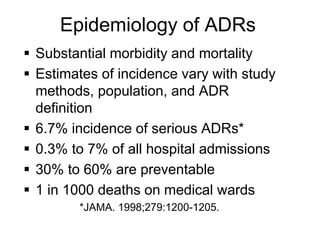
1) Adverse drug reactions (ADRs) are unintended harmful effects of drugs that occur at normal dosages for treatment or diagnosis. They can range from mild to severe or life-threatening.
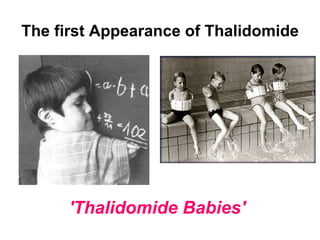
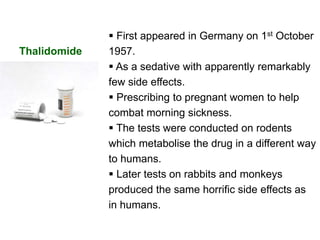
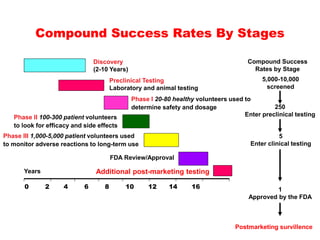
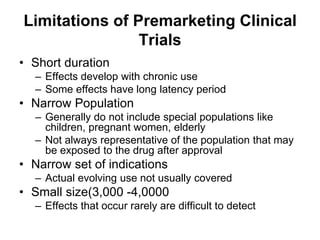
2) Thalidomide caused birth defects in the late 1950s when taken by pregnant women for morning sickness, highlighting limitations of pre-market drug testing like short duration and narrow populations studied.
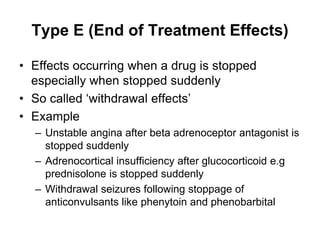
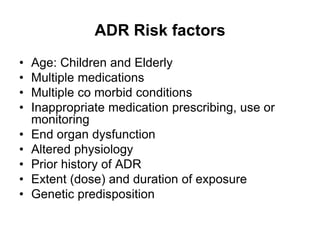
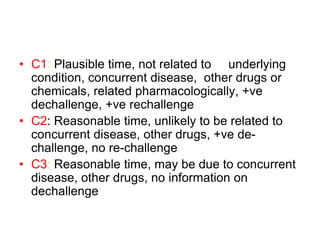
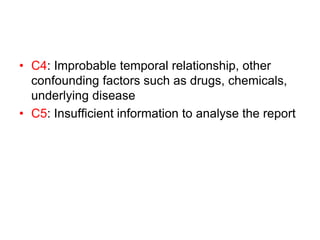
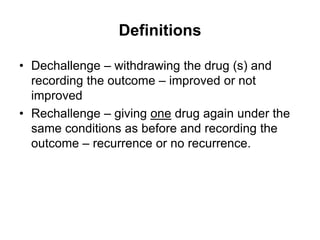
3) ADRs are classified based on onset, severity, and type. Type A reactions are dose-dependent and predictable while Type B are unpredictable and potentially life-threatening. Causality assessment considers factors like temporal relationship and de-challenge/re-challenge responses.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
