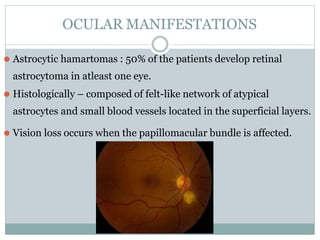
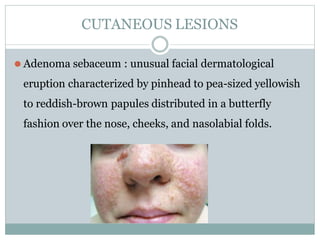
The document defines phakomatoses as multisystem disorders that affect the central nervous system, eyes, and skin with characteristic lesions and hamartomas. Common phakomatoses include neurofibromatosis types 1 and 2, tuberous sclerosis, Von Hippel-Lindau syndrome, Sturge-Weber syndrome, and Wyburn-Mason syndrome. Neurofibromatosis type 1 is characterized by café au lait spots and Lisch nodules on the iris. Tuberous sclerosis causes retinal astrocytic hamartomas and adenoma sebaceum skin lesions. Von Hippel-Lindau syndrome features retinal capillary hemangioblastomas and central

























































![[DSC Europe 25] Borko Kozomora - Optimizing business workflows with advances ...](https://cdn.slidesharecdn.com/ss_thumbnails/hbgekyb0txw0xpo4yfml-borko-kozomora-leading-ai-transformation-260122103838-cc29ee38-thumbnail.jpg?width=640&height=640&fit=bounds)


