Downloaded 55 times

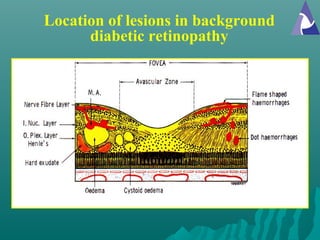
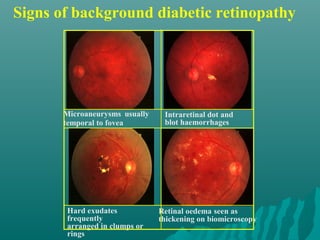
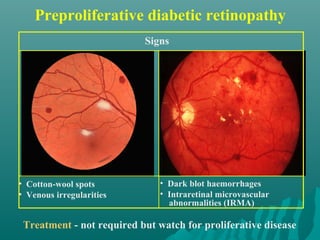
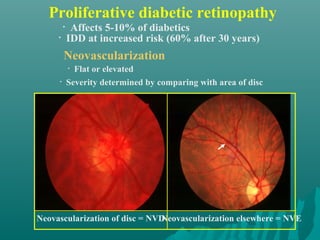
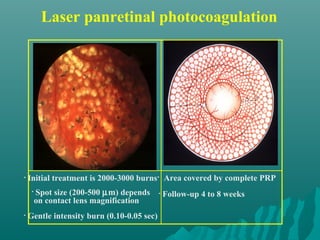


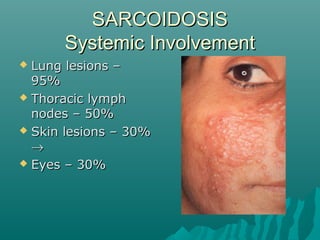
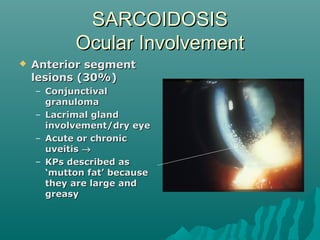
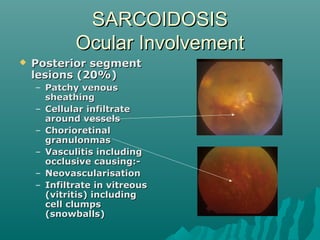
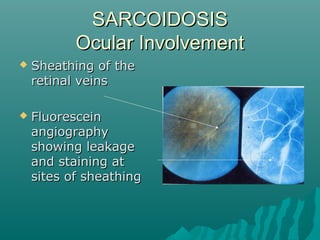
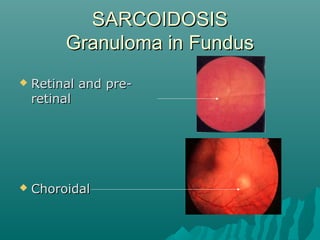
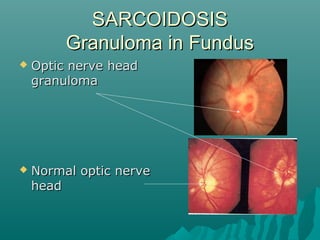
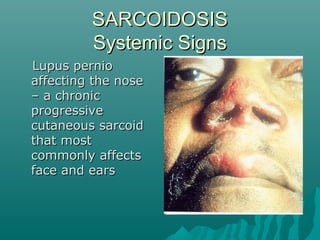
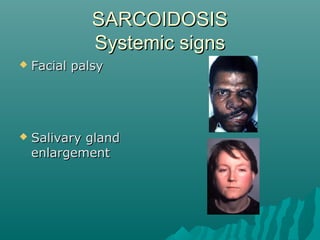
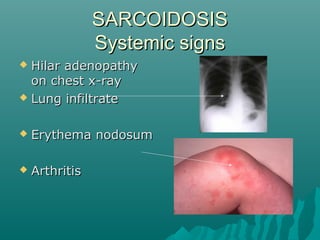
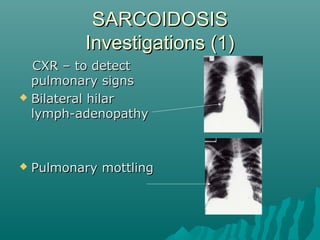

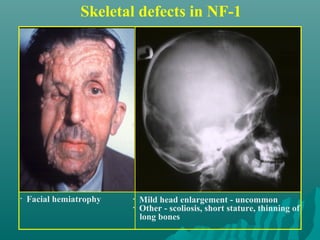
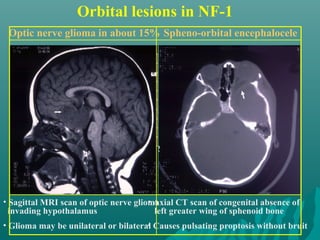
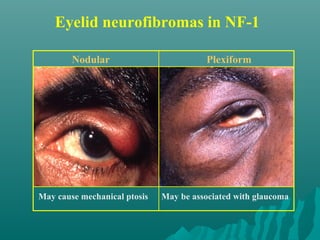
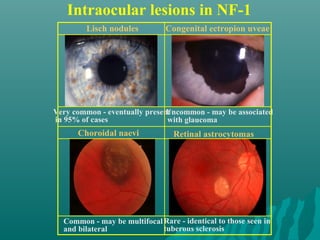
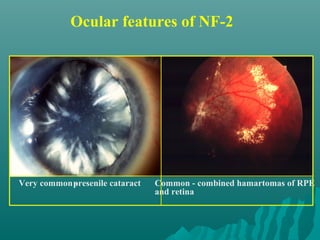
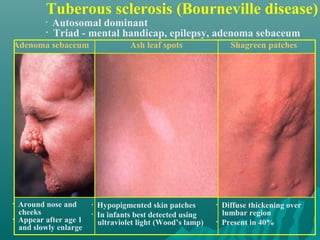
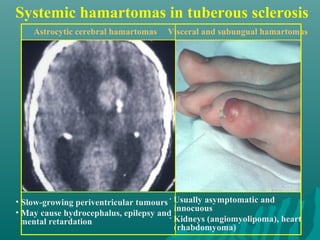
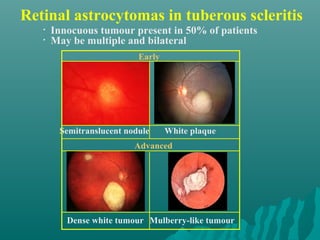
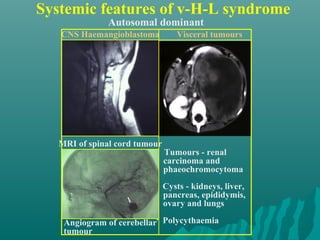

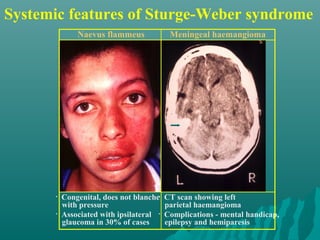
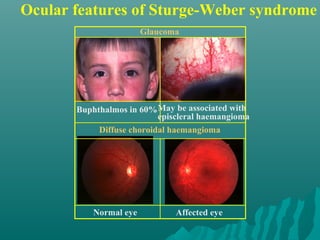
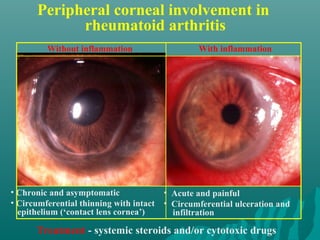
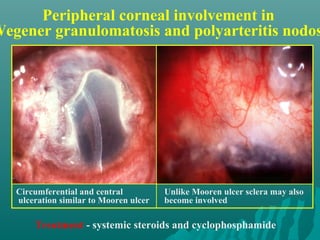
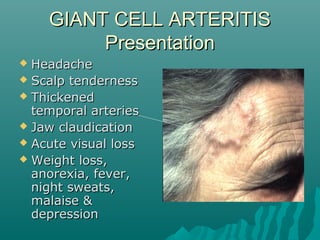
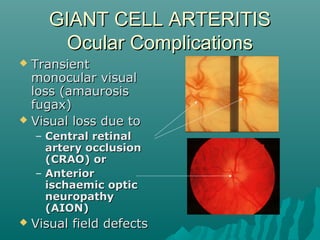









This document discusses common systemic diseases that can affect the eye, including infectious diseases like toxoplasmosis and tuberculosis, and non-infectious diseases like diabetes, connective tissue diseases, and vasculitides. It provides details on diabetic retinopathy, including risk factors, stages of progression from background retinopathy to proliferative retinopathy, and treatment with laser panretinal photocoagulation. It also summarizes ocular features and systemic signs of sarcoidosis, phakomatoses including neurofibromatosis, tuberous sclerosis, von Hippel-Lindau syndrome, and Sturge-Weber syndrome. Giant cell arteritis is also briefly discussed.


































































