1) Abdominal tuberculosis poses a diagnostic challenge due to its nonspecific symptoms. It is increasingly common and can involve the gastrointestinal tract, peritoneum, lymph nodes or solid organs.
2) Tubercle bacilli typically spread from the lungs or ingested materials to the abdominal cavity via the bloodstream or lymphatics. This can cause caseating granulomas and lesions in the abdomen.
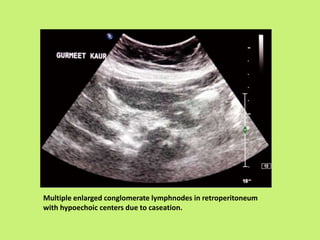
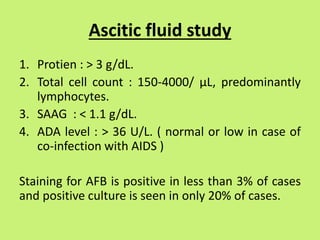
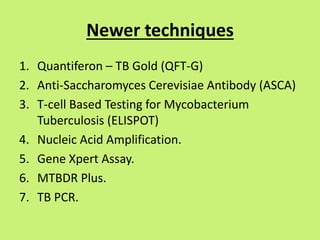
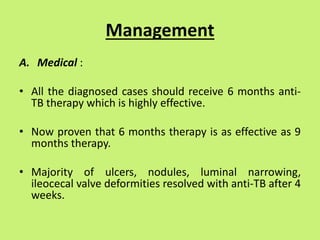
3) Common presentations include abdominal pain, fever, weight loss, and ascites or abdominal masses. Imaging shows lymphadenopathy, bowel thickening or strictures, and ascites. Diagnosis relies on clinical suspicion plus histology, microbiology or response to antitubercular treatment.

















![Ileo cecal TB presentation -SRK Sir[final-2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ileocecaltbpresentation-srksirfinal-2-250219184143-cbd9c4b9-thumbnail.jpg?width=640&height=640&fit=bounds)










































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)









