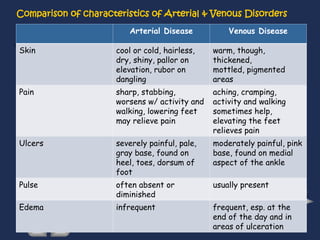
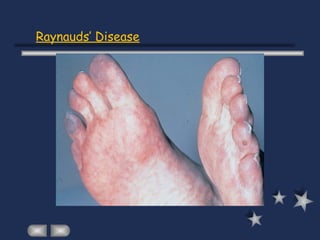
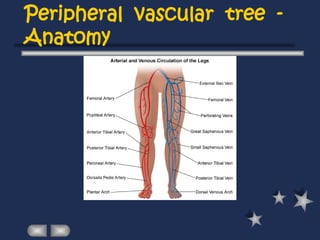
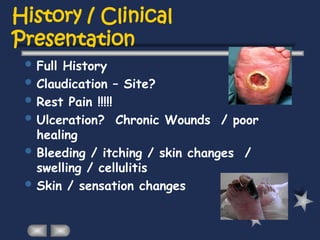
The document provides an overview of peripheral vascular diseases, detailing the structure and function of arteries and veins, and discussing arterial and venous insufficiencies. It highlights risk factors, comparisons of arterial and venous disorders, and specific conditions such as arteriosclerosis obliterans and Raynaud's phenomenon. Additionally, it covers the examination and assessment techniques for diagnosing these vascular issues.