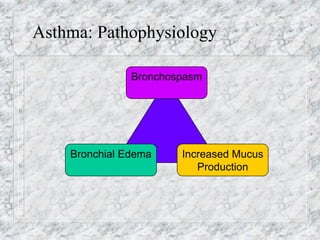
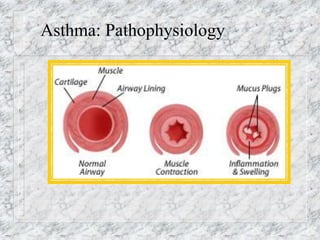
This document discusses several common pediatric respiratory emergencies. It begins by noting that respiratory issues are the leading cause of pediatric hospital admissions and deaths in the first year of life outside of congenital abnormalities. It then provides details on the pediatric respiratory system and risks for failure. Specific conditions covered include croup, epiglottitis, asthma, bronchiolitis, and foreign body airway obstruction. For each condition, it discusses pathophysiology, signs and symptoms, risk factors, and management strategies. Throughout it emphasizes the importance of maintaining the airway, providing oxygenation and ventilation support, and using caution with bronchodilators in critically ill pediatric patients.